
Abstract

Ear, nose, and throat (ENT) procedures carry a high risk of aerosol generation and COVID-19 transmission. In COVID-19 patients, a high viral load exists soon after symptoms begin, especially in the nasal region. The viral load in asymptomatic patients is similar to that in symptomatic patients, highlighting asymptomatic patients’ role in transmission of the disease. 1 However, many reports on transmission are anecdotal and based on personal experiences.
During the outbreak, routine examinations that included laryngoscopy/endoscopic nasal/nasopharyngeal examinations and laryngostroboscopy were reserved only for selected cases. 2 All ENT procedures can produce sneezing and coughing, causing the production of aerosol droplets. In addition to other aerosol-generating procedures (eg, intubation and bronchoscopy) that are mostly performed in “healthy” controls, in the COVID-19 outbreak, patients were admitted to health centers and examined by ENT specialists, posing a great risk of contamination to medical personnel. 3 Contamination of the examination department and equipment was also possible. Observational reports from Wuhan/China indicated that ENT specialists comprised the largest group of infected medical staff. 4 Other reports indicated that primary care and emergency department doctors were most commonly affected among health care workers, raising important concerns about the primary factors for transmission and appropriate use of personal protective equipment (PPE).
Both factors are essential from the perspective of ENT staff. The ENT procedures should be performed in a negative pressure room with the aid of full PPE. However, negative pressure chambers are generally limited in most facilities and their use can be costly; additionally, the staff members are still close to the patient, which creates a transmission risk. Herein, we present a modification of a unit from Tofaş Türk Otomobil Fabrikası AŞ, Istanbul, 5 which is mainly used for the collection of nasopharyngeal swabs. We modified the unit for ENT examinations (Figures 1– 3). The overall details of chamber are listed here: https://drive.google.com/drive/folders/1m99ev9H9zNxDTLwrxyBT7j1bN6a2uKFZ. 6

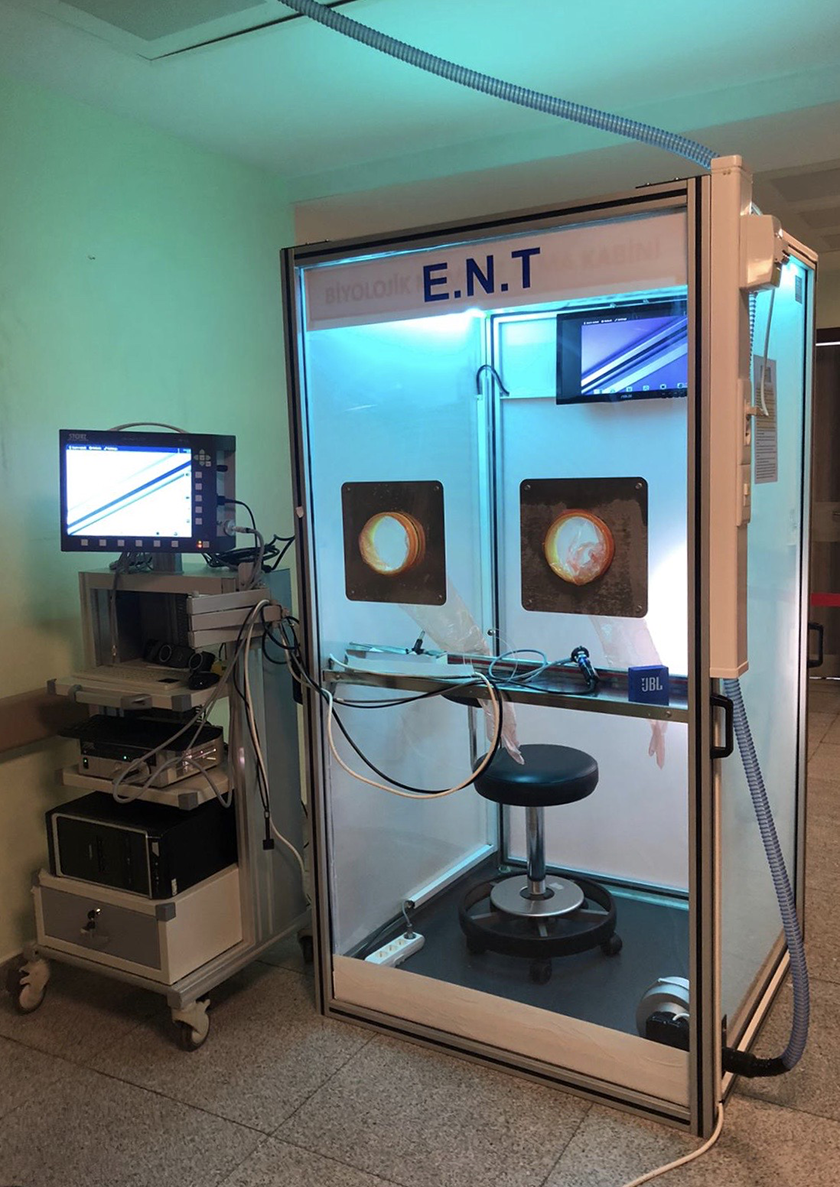
Examination in a closed chamber ear, nose, and throat unit.

Back view of the ear, nose, and throat unit.
Sterilisation was 2 step procedure. This step only showed the UV-C sterilisation phase.
Dimensions 107 × 100 × 200 cm.
Two-sided UV-C lamps for disinfection on both sides of the roof (254 nM).
Air inlet in the ceiling protected by a filter.
Exhaust system in the ceiling with an aspirating fan. The vented air is directed into the hospital’s central environmental suction climate system and treated from central system.
Isolation of the room to prevent the flow of air droplets outside.
A Bluetooth speaker in the room to allow communication between the examiner and patient (JBL Go; Harman International Industries).
An additional screen was located behind the patient to facilitate the physical examination and connected to a Storz Telepack system (Karl-Storz).
For time-sensitive and emergent examinations of patients with a suspected high viral load, we use this closed unit to protect health care workers. The patient enters the closed room via the back door and the fan is turned on to create negative pressure. The physician also wears PPE for the routine examination: either a combination of N95 mask/eye protector/gown/face protector/gloves or a powered air-purifying respirator (Dräger X-plore 8000; Draeger Inc). Next, the patient’s oropharyngeal region is anesthetized with topical gel and the nasal cavity is anesthetized with cotton pledgets in order to eliminate aerosol generation. The ENT examination is focused on certain areas and completed as quickly as possible. After the procedure, the patient leaves the room and the endoscope is placed in a metal carrying container, after which the room is UV sterilized for 5 minutes, then further sterilized with 78% ethanol. The room sterilisation procedure is 5 minutes UV-C than 78%ethanol cleaning (endoscopes taken from the room at this stage) than 5 minutes UV-C again. Than room is kept empty for 3 hours . An additonal 5 minutes of UV-C sterilisation was done before each patient. Total 15 minutes UV-C was given to the room.
Since there are no studies on sterilization dynamics for COVID-19 specifically, we chose the 3-hour interval according to previous reports dealing with similar pathogens. For example, UV-C effectively inactivated the virus previously. 7 Presterilization use of UV-C was addressed in previous studies. 8 Bedell et al 7 reported that 5 minutes of exposure with a UV-C emitter resulted in undetectable levels of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in droplets or a percent reduction of >99.999%. However, UV-C should not replace standard disinfection procedures. 8 Bedell et al 7 also reported that UV-C was most effective when used along with terminal cleaning of hard surfaces and sterilization using 78% ethanol. Previously, various chemicals were found to effectively inactivate SARS-COV, including 78% ethanol. 9 The second 5-minute UV-C sterilization was done to prevent transmission from the health care worker into the room. Since a recent article indicated that the virus can remain viable for up to 3 hours in air, we suggest waiting at least 3 hours between examinations. 10 During that time, the doors remain closed and the indoor fans continue to create negative pressure. After 3 hours, the next patient may enter following resterilization of the room with UV-C for 5 minutes.
The room allows us to avoid direct contact with the patient while performing all ENT examinations safely and effectively, including otoscopy, nasopharyngoscopy, and laryngoscopy/stroboscopy. The contaminated equipment and the room itself are sterilized with UV-C before the equipment is retrieved. The negative pressure in the room blocks aerosol dissemination.
Although clinicians are attempting to decrease the number of endoscopic examinations being performed, these procedures are necessary in certain groups of patients. 2 Closed chamber negative pressure ENT examination rooms should be used as a type of negative chamber room; however, these are often not accessible. The chamber we described above is not standard and it can be modified as required. For example, a back door might not be ideal or even possible for some examination rooms and its placement could be specified by users who order the chambers. Regardless, separating the examiner from the patient decreases the risk of transmission of disease between health care workers and their patients.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.