
Abstract

Renal cell carcinoma (RCC) is the most common malignant kidney tumor and originates from the renal cortex. 1 Metastatic disease may affect up to 18% of patients on presentation and commonly involves the lungs, bone, liver, and brain.2,3 Two prior case reports have documented metastatic RCC to the trachea resulting in respiratory distress.4,5 In the modern era of immunotherapy, patients with metastatic RCC are being treated with a class of immune checkpoint inhibitors known as anti-programmed death receptor-1 (anti-PD-1) axis inhibitors. 6 These medications disinhibit T-cell antitumor function, which can subsequently lead to a constellation of systemic side effects. 7 A small subset of patients on these medications may have atypical treatment responses including “hyperprogression”—a rapid increase in tumor growth compared to the expected growth rate 8 —and “pseudoprogression,” which represents a tumor flare characterized by transient tumor growth followed by decreased total burden. 9 When located in the airway, tumor hyperprogression can quickly become life-threatening. We present a case of endoscopic management of metastatic RCC to the trachea resulting in respiratory distress due to an atypical treatment response to anti-PD-1 therapy.
A 68-year-old Filipino male with long-standing widely metastatic RCC presented as a referral to Otolaryngology Clinic due to the incidental finding of tracheal lesion on surveillance computed tomography (CT) imaging (Figure 1A). He had been undergoing treatment with anti-PD1 inhibitor pembrolizumab 3 months prior to evaluation. In-office flexible fiber-optic bronchoscopy demonstrated an exophytic hypervascular endotracheal mass causing approximately 40% airway obstruction. Over the course of the next few weeks, the patient became increasingly symptomatic presenting to the emergency department with hoarseness, cough, hemoptysis, and stridor. Repeat CT (interval 3 weeks) demonstrated tumor growth (Figure 1B). He was admitted for definitive airway management.
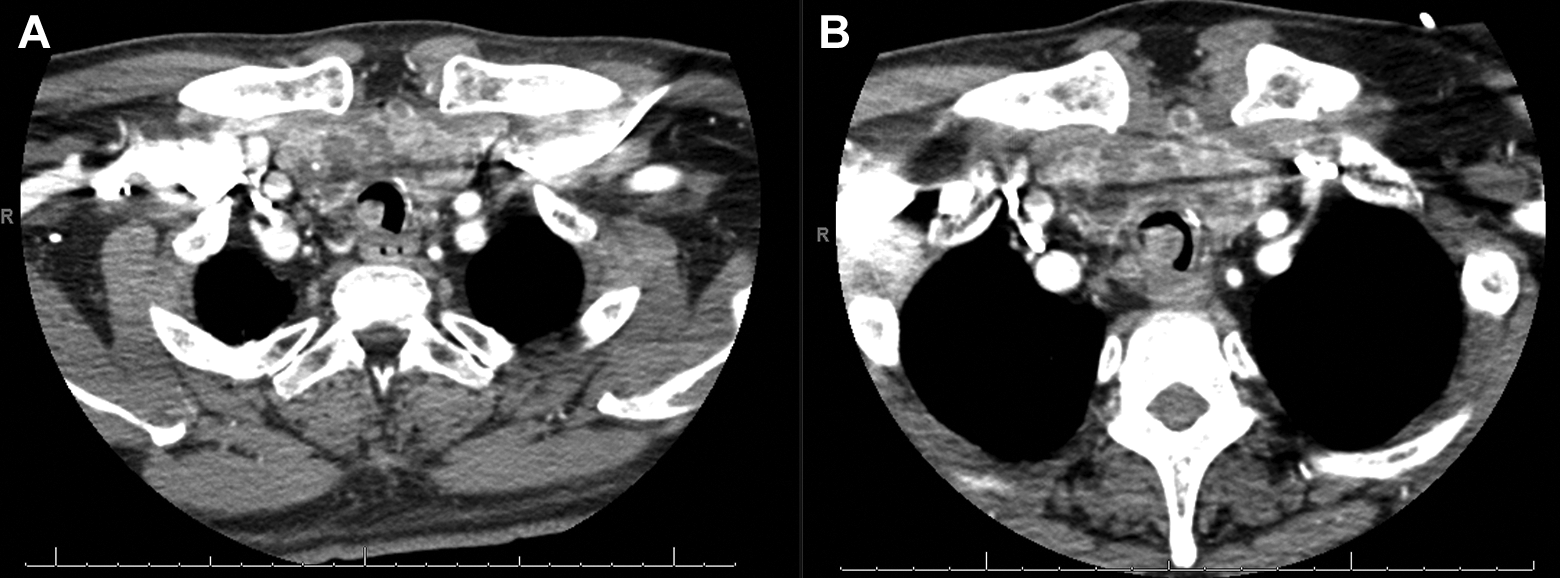
A, Axial computed tomography (CT) of the chest soft tissue window demonstrating proximal tracheal mass. B, Axial CT of the chest soft tissue window demonstrating interval growth of tracheal mass over 3 weeks.
The patient was taken to the operating room (OR) for definitive airway management. Initially, spontaneous ventilation was attempted, but airway obstruction quickly ensued. After suspension laryngoscopy with supraglottic jet ventilation failed to adequately ventilate the patient, a rigid ventilating bronchoscope was inserted which revealed a friable multilobulated mass nearly filling the tracheal lumen (Figure 2A). A flexible fiber-optic Nd:YAG laser bronchoscope was passed through the rigid bronchoscope to quickly coagulate the proximal surface of the tumor mass followed by debulking with optical forceps (Figure 2B). To minimize further bleeding from the friable tumor, the remaining volume of disease was treated in a piecemeal fashion using cryoablation, resulting in substantial improvement in airway patency (Figure 2C). The patient was reintubated, transferred to the intensive care unit, and returned to the OR postoperative day 1. KTP laser bronchoscopy (flexible laser bronchoscopy passed through rigid laryngoscope) was performed to ablate a small volume of residual tumor followed by extubation. Histopathological examination demonstrated clear cells within the tracheal parenchyma consistent with known RCC surrounded by a robust mixed inflammatory infiltrate (Figure 3) consistent with tumor hyperprogression. The patient was subsequently treated with adjuvant fractionated radiation therapy to the trachea and continues anti-PD-1 immunotherapy.
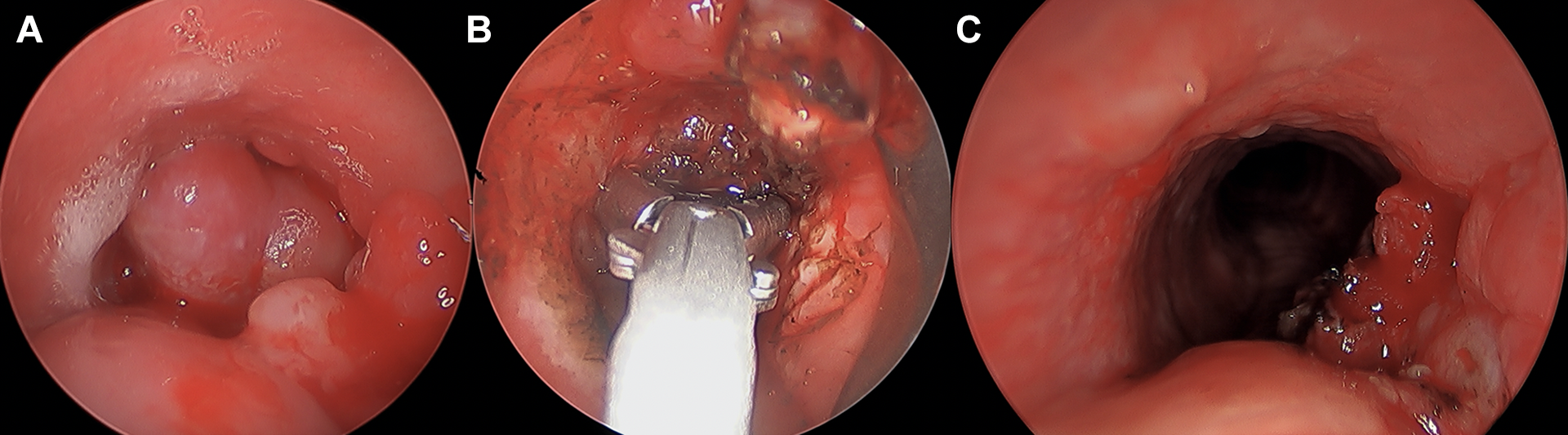
A, Rigid bronchoscopic view of proximal trachea with large friable tumor obstructing over 95% of the tracheal lumen 3 cm distal to the glottis. B, Rigid bronchoscopic view of the proximal trachea demonstrating cupped forceps debridement of metastatic renal cell carcinoma (RCC). C, Rigid bronchoscopic view of proximal trachea demonstrating significant debulking of metastatic RCC and restoration of functional tracheal airway after Nd:YAG laser, cryosurgery, and cupped forceps debridement.
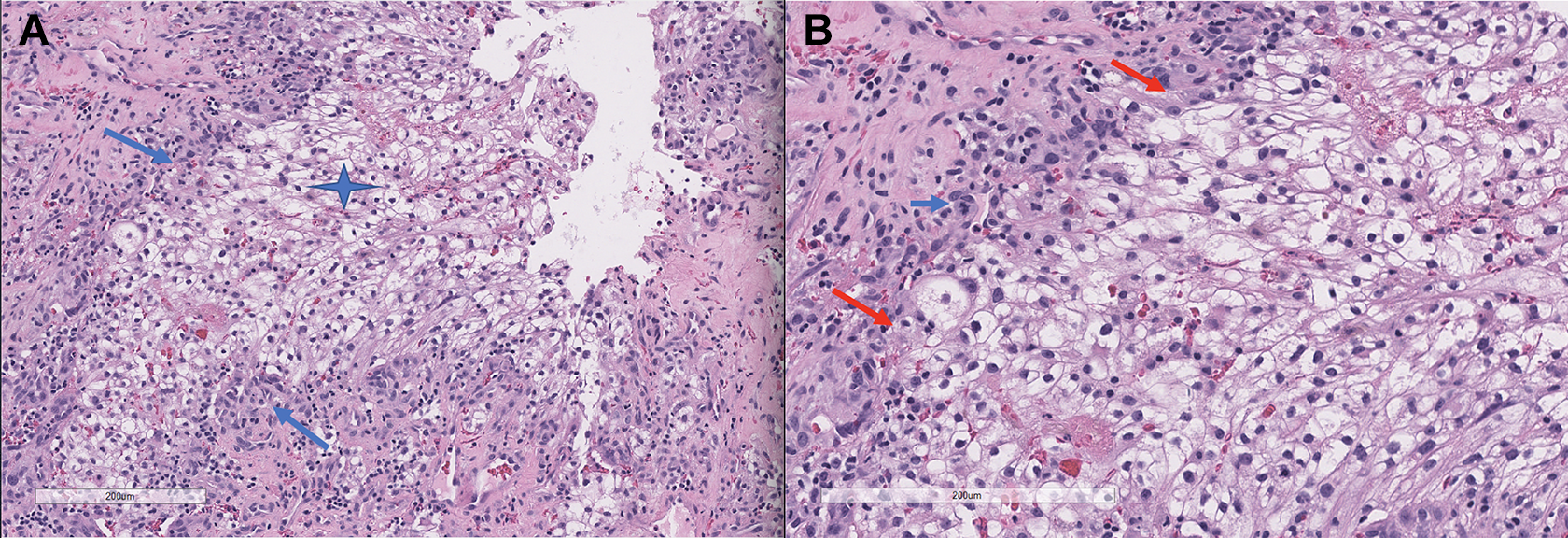
A, H&E ×10. Intermediate power view of metastatic renal cell carcinoma, clear cell type (blue star) within the larynx. A marked mixed inflammatory infiltrate of lymphocytes and neutrophils surrounds the tumor (blue arrows). B, H&E ×20. High power view of metastatic renal cell carcinoma composed of large clear cells. Note the prominent mixed inflammatory infiltrate of atypical lymphocytes (red arrows). A mitotic figure is noted (blue arrow).
The clinical manifestations of endotracheal tumors are variable, ranging from a mild cough and dyspnea to acute respiratory failure. Diagnosis can be delayed for months or even years due to symptoms that can mimic asthma. In-office flexible bronchoscopy is an important point-of-care tool that allows rapid diagnosis when airway neoplasm is suspected. A tracheal mass in an adult is most likely a primary malignancy, with squamous cell carcinoma and adenoid cystic carcinoma being the first and second most common pathologies, respectively. 10 Despite a paucity of documented cases of metastatic RCC to the trachea, in a patient with known RCC and tracheal mass, clinical suspicion for a metastatic process should remain until histopathologic diagnosis is achieved.
Treatment of metastatic lesions of the trachea can be divided into (1) acute airway management and (2) definitive and/or palliative therapy with surgery, chemotherapy/immunotherapy, radiotherapy, or some combination of these modalities. Surgical treatment with segmental tracheal resection is typically reserved for primary tracheal tumors. 11 In the case of metastatic disease, the primary objective is to provide a secure and reliable airway. Many techniques have been described including the use of surgical lasers (CO2, KTP, Nd:YAG), electrosurgical snare, argon plasma coagulation, cryosurgery, surgical debulking with cold steel, and endotracheal stents with the goal of improving airway patency.12-17
To the best of our knowledge, this is the first report of an RCC metastasis presenting as a tracheal mass exhibiting behavior consistent with tumor hyperprogression on anti-PD-1 immunotherapy. Awareness of this clinical entity is important for the airway surgeon, and treatment may require urgent intervention and tools outside the typical armamentarium of the otolaryngologist.
Footnotes
Author’s Note
This study was accepted for poster presentation at the Combined Otolaryngology Spring Meetings, American Broncho-Esophagological Association Virtual Poster Session, May 15, 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.