
Abstract
Purpose:
Precise knowledge of the level of the vocal fold as projected on the external thyroid cartilage is of critical importance for the performance of many surgical approaches. This study aims to identify the level of the anterior commissure, as well as the lengths of the vocal muscle and arytenoid cartilage in Turkish population.
Materials and Method:
Specimens were collected after autopsy from the Council of Forensic Medicine. One hundred human larynges (52 men, 48 women; age range: 25-80 years) were dissected under a stereomicroscope. Projection of the vocal fold was analyzed in relation to the superior thyroid (A) and the inferior border of the thyroid cartilage (B). Then, the larynx was dissected parallel to the level of the vocal fold to measure the length of the vocal muscle (C) and the length of the interarytenoid space (D).
Results:
The mean value of the “a” was 9.15 ± 1.99 mm in male and 9.38 ± 3.43 mm in female. Mean value of the “b” was 10.54 ± 1.73 mm and 8.88 ± 1.81 mm in male and female, respectively. The mean value of the parameter corresponding the length of vocal muscle which was “c” was found 15.00 ± 3.18 mm in male and 12.88 ± 4.12 mm in female. The mean value of the interarytenoid space “d” was 8.31 ± 1.76 mm in male and 8.13 ± 1.90 mm in female. Comparing between genders, no statistical differences were observed in parameters of a, c, d, a + b, a + b/2 (P > .05). However, the difference with female and male for the parameters of b and c + d was statistically significant (P < .05).
Conclusion:
Our results indicate that the anterior commissure projects slightly above the midline height for male and at the level to slightly below in female subjects in Turkish population.
Introduction
The larynx is divided into 3 main areas as supraglottic, glottic, and subglottic spaces. The paired vocal folds reside at glottis which is also called transglottic space. 1 Right and left vocal cords unite to form the anterior commissure at the front and it adheres to the inner surface of the thyroid cartilage. They are attached to the vocal process of the arytenoid cartilage posteriorly. As an important component of the larynx, the vocal fold is active during voice production, respiration, and airway protection. 2 Precise knowledge of the laryngeal dimensions is necessary for treatment and surgical procedures of laryngeal and voice diseases. 3
Thyroplasty type I was first proposed by Isshiki et al in 1974, which is also described as lateral compression. Thyroplasty type I aims to shift the vocal cord medially through deformation of the thyroid cartilage. 4 This method was indicated for laryngeal diseases resulting from imperfect closure of the glottis during phonation without swelling or tumor of the vocal fold. More commonly, thyroplasty type I is also indicated for unilateral vocal cord paralysis. 4 Surgery aims to medialize and augment the paralyzed vocal fold and the underlying soft tissue by pushing cartilage inward through a window dissected on the thyroid cartilage. Previous research reports that the most common reason for failure in thyroplasty type I is window misplacement (too high posteriorly). 5 Also, during laryngeal framework surgery, an overly high implant position might harm the false vocal cord or end in the Morgagni’s ventricle. Therefore, an accurate estimation of the level of the vocal fold relative to the thyroid cartilage is important.
The purpose of this study is to determine the level of the anterior commissure and length of the vocal muscle and arytenoid cartilage and establish the normative values in the Turkish Population and to compare these data already available in the literature.
Materials and Methods
Cadaveric Material
Specimens were collected after autopsy from the Council of Forensic Medicine, which is an official department of the Ministry of Justice (Data proc. num. 2004/19—19.01.2004), Turkey. Necessary permissions were gathered, and all dissections were performed in line with the laws of the Republic of Turkey. One hundred human larynges, none of which had laryngeal injuries because of trauma or were implicated in the cause of their death, were obtained from autopsy (52 men, 48 women; mean age 48 and 37, respectively).
Dissection Procedure
Before starting the measurements, the 100 larynges were divided along the midline posterior with a vertical incision of the cricoid lamina and the adjacent soft tissue. One needle was inserted at the position of the anterior commissure which is the junction of the vocal cords anteriorly and passed from the endolarynx to the thyroid ala externally (Figures 1-3). Measurements were made of the position of the needle in relation to the superior thyroid notch (A) and the inferior thyroid notch (B). Then, the larynx was dissected parallel to the level of the vocal fold to measure the length of the vocal muscle (C) and the length of the interarytenoid space in sagittal plane (D;Figure 4). These locations were adapted from the previous studies.5-7 For morphometric measurements, Digital calliper (Altas 905, 150 mm) were used. Each parameter was measured twice by same observer and in case of different values the average was recorded.
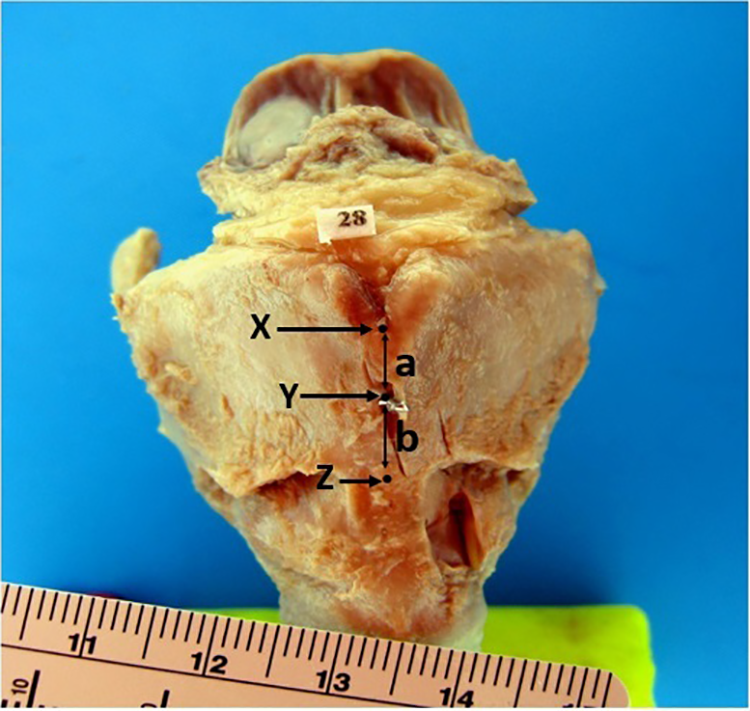
Anterior view. a, the distance between anterior commissure and superior thyroid notch; b, the distance between anterior commissure and inferior thyroid notch; X, superior thyroid notch; Y, anterior commissure; Z, inferior border of thyroid cartilage.
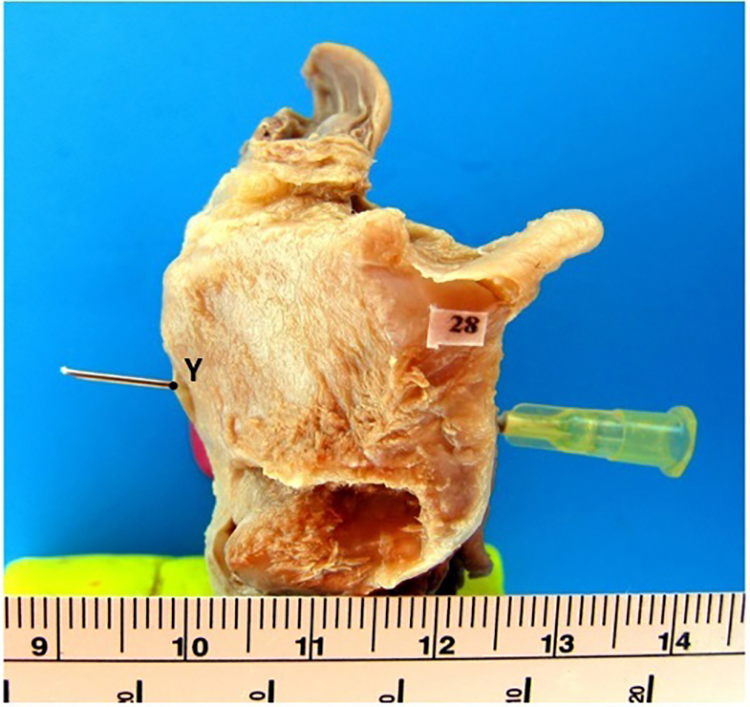
Lateral view. a, the distance between anterior commissure and superior thyroid notch; b, the distance between anterior commissure and inferior thyroid notch; X, superior thyroid notch; Y, anterior commissure; Z, inferior border of thyroid cartilage.
Statistics
Mean values for all samples were calculated with 95% CIs, and P values <.05 were regarded as statistically significant. Kolmogorov-Smirnov test was used for normality test. Nonparametric Mann-Whitney U test was used to evaluate the differences between the parameters and calculating means and standard deviations. Statistical analyses were performed using NCSS (Number Cruncher Statistical System) 2007 Statistical Software.
Results
These measurements included, aside from an evaluation of the whole organ, identification of the anterior commissure of the thyroid cartilage, and length of the vocal muscle (vocal fold) and interarytenoid space. Data are presented separately for male and female subjects (distances in millimeters).
Table 1 shows the minimum, maximum, mean values, and sample sizes for every parameter for both sexes. Table 2 shows the mean values and the statistical results of the laryngeal measurements in males and females. The results provide mean values, standard deviations, and sample sizes. Data are given for every parameter separately for both sexes. No statistical differences were observed, and the measurements were presented as “a, c, d, a + b, c + d” and age in male and female groups (P > .05). However, the mean value of “b” is greater in men (10.54 mm) than in women (8.88 mm). This value is statistically significant (P < .05).
The Measurement of the Laryngeal Framework.a
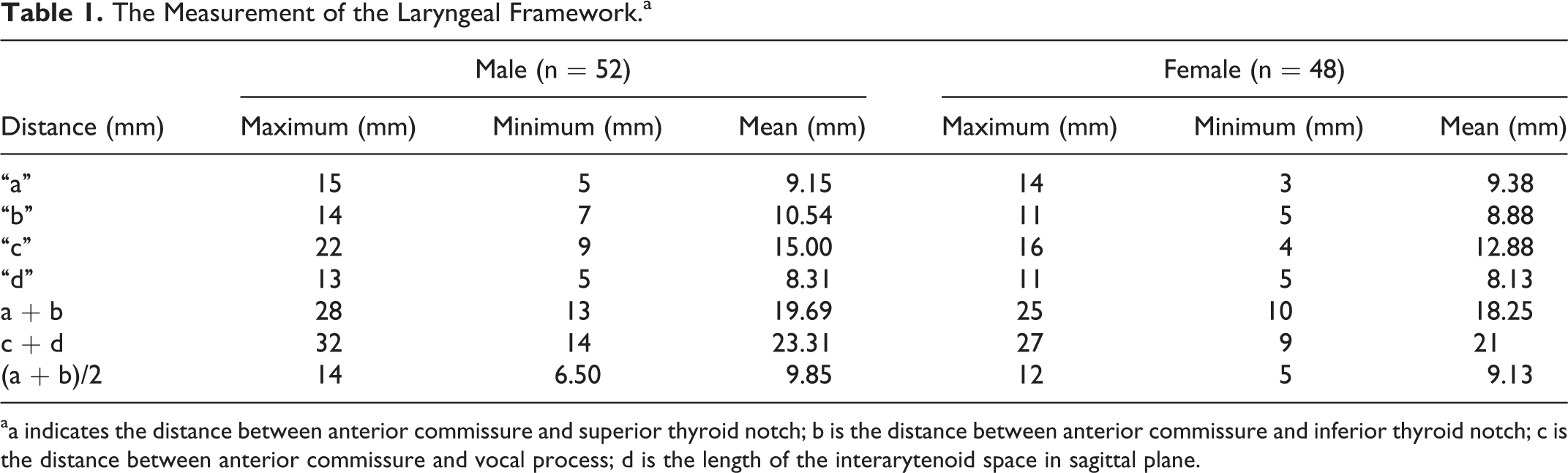
aa indicates the distance between anterior commissure and superior thyroid notch; b is the distance between anterior commissure and inferior thyroid notch; c is the distance between anterior commissure and vocal process; d is the length of the interarytenoid space in sagittal plane.
The mean value of the midline height at the anterior thyroid cartilage which is a + b/2 was found 9.85 mm in male and 9.13 mm in female. This difference was statistically not significant (P > .05).
However, the mean value of c + d value was 23.31 and 21.00 mm in male and female, respectively, and the difference is statistically significant (P < .05).
Laryngeal Measurements.a
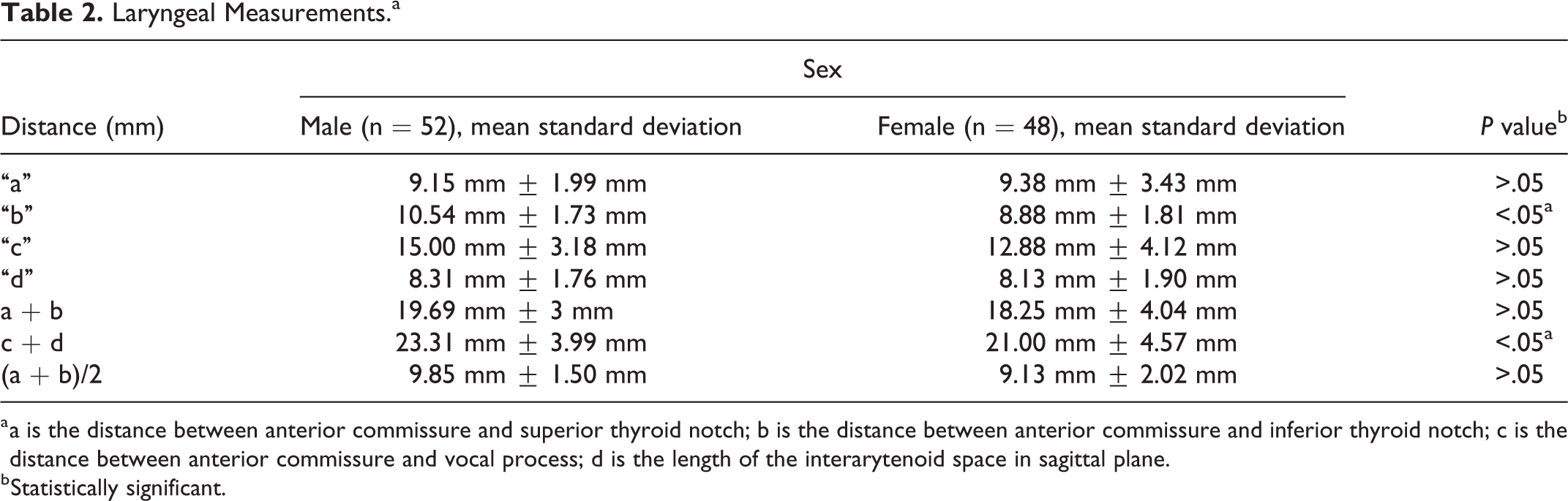
a a is the distance between anterior commissure and superior thyroid notch; b is the distance between anterior commissure and inferior thyroid notch; c is the distance between anterior commissure and vocal process; d is the length of the interarytenoid space in sagittal plane.
b Statistically significant.
Discussion
In cases of vocal cord paralysis, treatment is planned according to the cause of paralysis and the resulting functional failure from it.8,9 Treatment aims to improve sound quality and prevent aspiration. In the treatment of unilateral palsy, medialization by injection or thyroplasty type 1 (medialization laryngoplasty) is applied. Medialization laryngoplasty is a laryngeal framework surgery method that was first proposed by Isshiki et al in 1974. 9 In the procedure, a cartilage window at the level of the vocal cord is opened on the thyroid cartilage, and with the help of an implant placed inside it, paraglottic area tissues on the paralytic side are brought to the midline to obtain a stable vocal cord surface, where the opposite vocal cord can make contact.8,10
Medialization and lateralization treatments have been going on for a long time without a change in methodology.
11
However, all methods have their drawbacks.
11
For this reason, to minimize complications related to morphological differences, precise knowledge of the vocal fold level is essential for these surgical interventions. In this study, we aimed to create an index of these distances in Turkish population with an approximately equal number and the largest number of male–female subjects among the literature. According to Isshiki et al,
4
“an anatomical study on the human cadaver larynx indicated that the anterior commissure of the vocal cords (upper surface) is positioned almost at the level of the midpoint between the thyroid notch and lower margin of the thyroid cartilage or slightly higher than that level.”
The distance from the anterior commissure to the inferior border of the thyroid cartilage was indicated as “b” in our study. This metric value was the only one showing statistically significant differences among genders. Here, we report values of 10.54 ± 1.73 for males and 8.88 ± 1.81 for females. Cinar et al reported the mean value of this distance as 11.5 mm in males and 8.1 mm in females. 5 Enver et al reported these values as 10.27 ± 2.96 and 7.86 ± 1 for males and females, respectively. 6
There have been many different mathematical approximations for the projection of the vocal fold. 12 Although Isshiki suggested that the vocal fold could be found with a line parallel to the midline of the thyroid cartilage, Koufman and Isaacson and Tucker et al propose that this line is at the superior margin of the thyroid cartilage.12-15 Netterville et al recommended a window of 3 mm superior to the caudal border of the thyroid cartilage.12,16 Meiteles et al 17 recommended that “thyroid cartilage incision for supraglottic laryngectomy should be made on a line joining the juncture of the upper one third and lower two-thirds of the midline length and the juncture of the upper one third and lower two-thirds of the oblique line. This will ensure a position above the level of the anterior commissure and the true vocal cord.”
Thus, there seems to be a lack of consensus on the recommendations. To evaluate this, a ratio is being used as distance from superior thyroid notch to the anterior commissure and the midline height from the superior thyroid notch to the inferior thyroid border. 5 Cinar et al reported this ratio as 0.41 in men and 0.38 in women, with no statistical difference between the genders. 5 The same ratio was reported as 0.53 ± 0.05 in females and 0.54 ± 007 in males by Enver et al for the thyroid cartilage inferior border to the anterior commissure. 6 Again, all 3 of these studies report minimal differences in results concerning the study group of the same population. All 3 studies report that the anterior commissure is above the midline for both male and female subjects. We have calculated this ratio as 0.46 for male and 0.51 for female showing that anterior commissure is above the midline in male and at the level to slightly below in females. Interestingly, Sprinzl et al 18 reported that most of the male samples (19 of 24) reside below the midline and most of the female samples resides at midpoint (17 of 21). Other samples were reported in different levels with different ratios. These results show that each author reported different results compared to Isshiki. Sprinzl et al 18 proposes possible ethnological differences for all different evaluations. However, our results show that difference may occur interpopulational too in terms of the projection of anterior commissure. It is also stated that formalin preservation artifacts may be effective in slight differences of the groups. 18
Vocal cord length is particularly important for singers as one of the key elements of voice recognition can be inferred. 19 It is important in pitch range and timbre of the voice. 19 The length changes according to their physiologic situation, such as the pitch of the voice and phonation intensity. 17 Also, it is significantly changes in terms of other parameters such as body length, neck diameter, and especially habitual fundamental frequency during speech in different voice categories. 20 Larsson and Hertegård 20 reported that bass/baritone group had significantly longer vocal folds than the soprano singers. Also, male subjects reported to have longer vocal folds than females. 20 Additionally, in another study, no relationship was reported between vocal cord measurements and healthy person’s body mass index. 21
It is obvious that vocal fold length is not stable in living people. So that, examination of vocal fold dimensions is not easy in vivo. 20 For this reason, most studies related to this value are obtained either directly from the cadavers or from radiologic images. 22 Previously, this length was given as 22.09 ± 3.07 in males and 17.55 ± 0.92 in females in a German population. 7 The same distance was reported as 24.46 ± 2.66 in males and 17.91 ± 2.15 in females for a South American population. 23 The mean vocal cord lengths in Enver et al’s study was 20.77 ± 3.75 mm in males and 16.43 ± 1.51 mm in females. A recent study from Egypt reported the whole vocal fold lengths as 24.9 ± 2.5 for males 17.5 ± 2.2 for females in the patients of laryngeal carcinoma. 2 In our study, the distance of c + d was 23.31 ± 3.99 for males and 21.00 ± 4.57 for females, and the difference between genders was statistically significant (Figures 3 and 4).
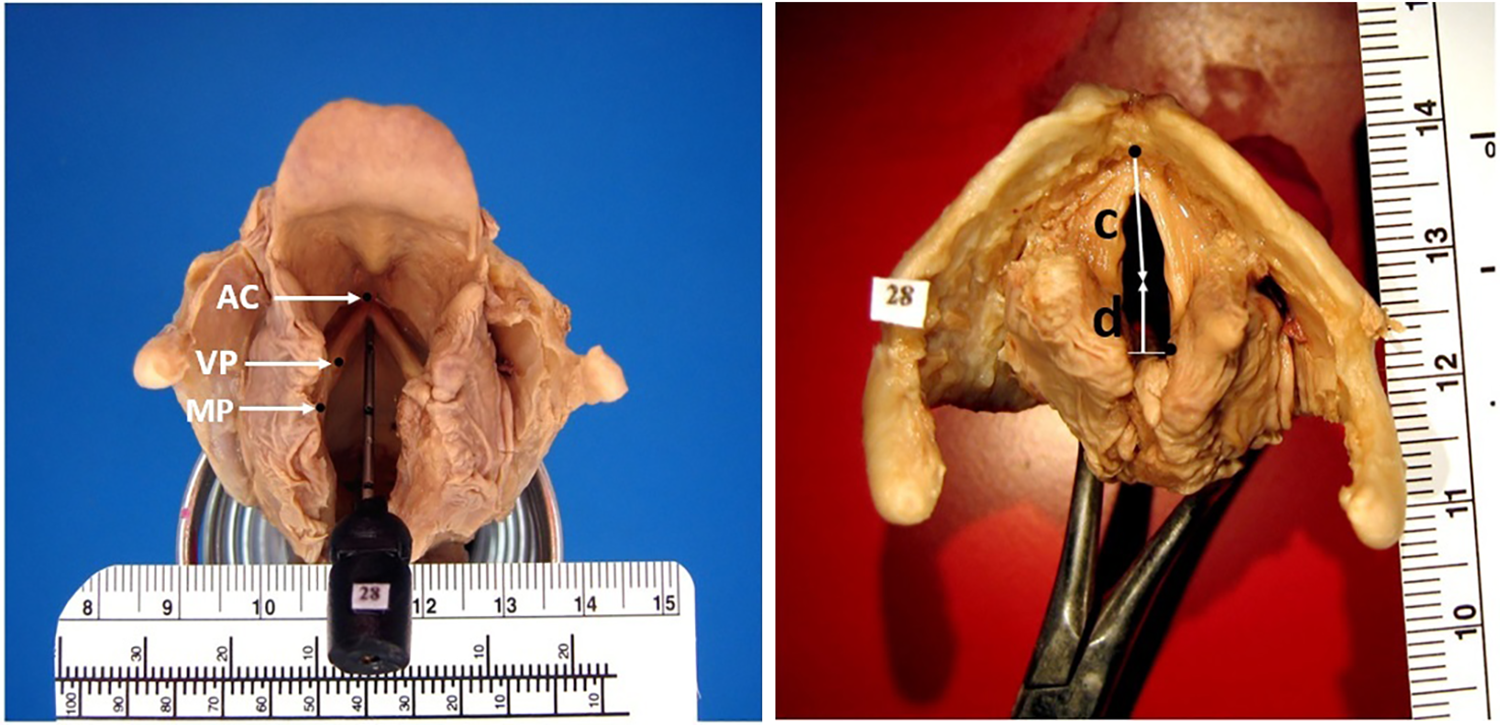
(both posterosuperior view). AC indicates anterior commissure; c, the distance between anterior commissure and vocal process; d, the length of the interarytenoid space in sagittal plane; MP, muscular process (arytenoid cartilage); VP, vocal process (arytenoid cartilage).
There are studies evaluating the true and false vocal cord length via different methods such as direct measurement on the images taken at microlaryngoscopy, radiography, computed tomography, or high-frequency sonography.3,22,24 Results of these measurements were not included in this discussion for comparison because of the technical differences and the possible differences in terms of cadaver tissue shrinkage.
Limitations of the Study
Even though, this study included a relatively equal number of male/female subjects, increasing both groups would improve the accuracy of the results. Different age groups such as children, adolescent, adult groups’ evaluation within and among the populations would also reflect the developmental aspect. One another pitfall of the study was the great variability of measures, landmarks, and labeling of measuring across different studies. Also, measurement of the mid membranous vocal fold at thyroid ala would be beneficial for medialization window guidance.
Conclusion
Data gathered from multiple populations might help guide interventions addressing the vocal fold. A most important result of our study is the difference between the laryngeal distance among and within the population. According to our results, the anterior commissure is slightly above the midline height for male and at the level to slightly below for female subjects. Our results also show that projection of the anterior commissure is highly variable even in same population which also should be taken into consideration.
Footnotes
Authors’ Note
This article does not contain any studies with human participants or animals performed by any of the authors. The cadaveric studies do not require ethical committee application in Turkey. Yet, all procedures performed in studies were with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. G.O. contributed to project development, data collection, manuscript writing and editing. Z.L. contributed to data analysis, manuscript writing and editing. A.O. contributed to data analysis, manuscript writing.
Acknowledgments
The authors would like to thank The Ministry of Justice, The Council of Forensic Medicine Turkey for the consent of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.