
Abstract

Mononucleosis (MN) is a systemic infection caused by the Epstein-Barr virus (EBV), which often results in a high viral concentration within the palatine tonsils and adenoids. Exudative debris plus tonsillar and adenoid hyperplasia is produced by infiltration of leukocytes. 1 Protracted aggressive MN infections can result in tonsil enlargement within the oropharynx leading to severe snoring and restless sleeping with respiratory pauses, further leading to hypopnea or obstructive sleep apnea (OSA).
Treatment options for OSA include hospitalization and, when severe, placement into an intensive care unit (ICU) for observation and reduction of hypoxia and airway support. The pulse oximeter readings often decrease during sleep and when fatigue impairs respiratory efforts. Supportive measures include supplemental oxygen by mask or nasal cannula, steroids, nasopharyngeal airway, and occasionally intravenous antibiotics to reduce secondary infections. We present a series of cases treated successfully with intracapsular tonsillectomy and adenoidectomy (T&A) during acute phase of MN.
Our first patient, a 17-year-old female, presented to the emergency department for evaluation of worsening throat pain, muffled voice, bilateral cervical lymphadenopathy, inability to swallow, and halitosis over the preceding 7 days. Five days prior, her pediatrician confirmed the diagnosis of MN. On evaluation, examination revealed 4+ “kissing” tonsils bilaterally with thick green exudates and midline uvula. Ultrasound of the neck did not detect intratonsillar or peritonsillar abscesses. She was admitted for treatment with intravenous antibiotics and steroids. By day 3, she had experienced worsening of symptoms with worsening fevers. Computed tomography of the neck with contrast demonstrated diffuse enlargement of tonsils and adenoids with 0.7-cm-diameter ring-enhancing collection in the left inferior peripheral tonsil and additional multiple bilateral enhancing foci concerning for developing multiple microabscesses within tonsils (Figure 1). After discussion with parents on day 4, the patient was taken to the operating room for intracapsular T&A by microdebrider.
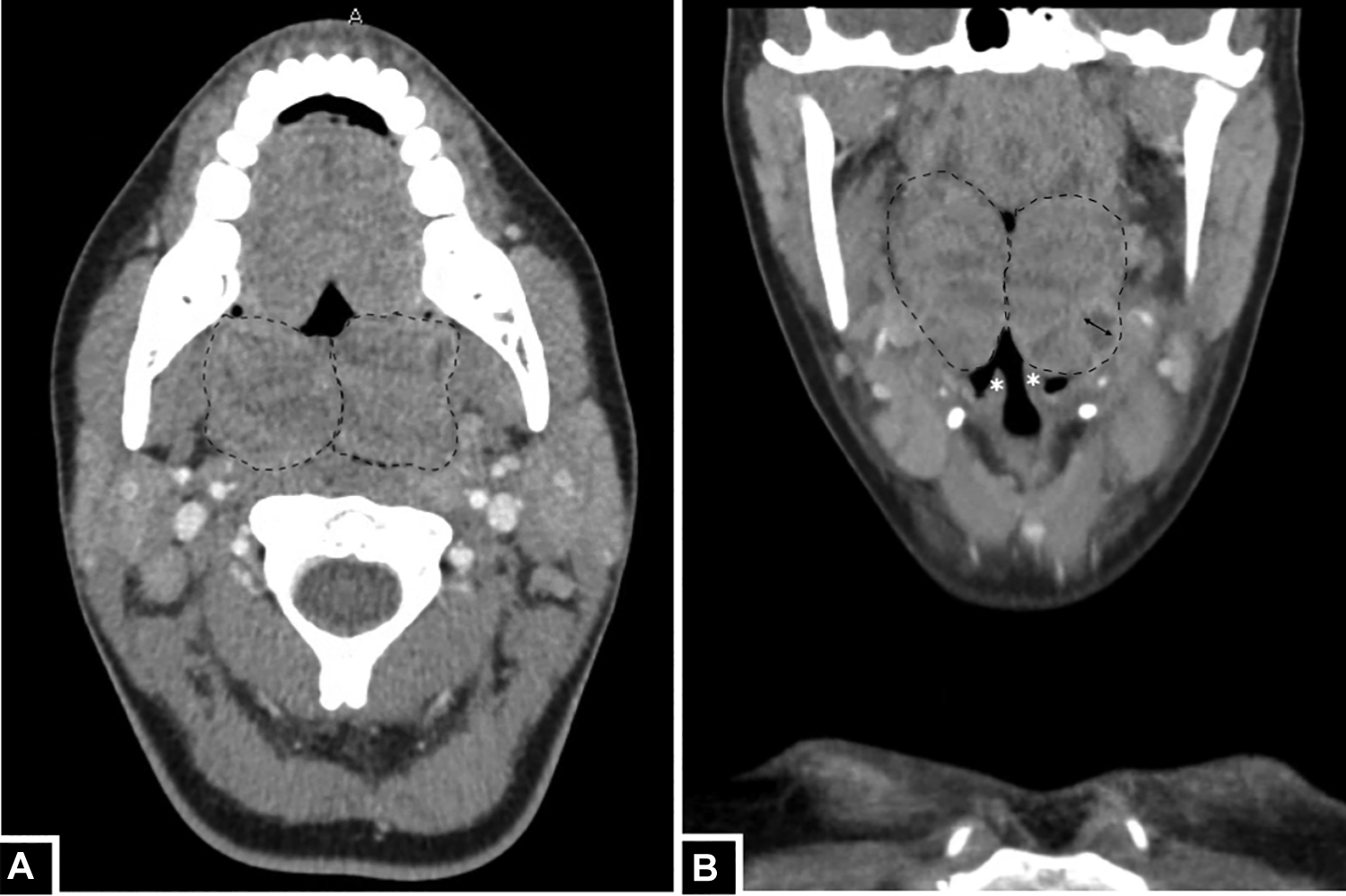
Severely enlarged tonsils (outlined) in axial (A) and coronal (B) computed tomography of the neck with contrast images. Enlarged tonsils extend inferiorly toward the epiglottis (*) and demonstrate intratonsillar abscess (bidirectional arrow).
Our second patient, a 17-year-old male, presented to the emergency department for evaluation of sore throat, muffled voice, bilateral cervical lymphadenopathy, and difficulty swallowing. Diagnosis of MN was previously confirmed by his pediatrician and he had completed an oral steroid taper without relief. Physical examination revealed enlarged 4+ palatine tonsils and neck ultrasound predicted right peritonsillar abscess. The boy was admitted for treatment with intravenous antibiotics and steroids. Despite this medical management, he continued to experience significant symptoms. On hospital day 3, intracapsular T&A by microdebrider was successfully completed (Figure 2).
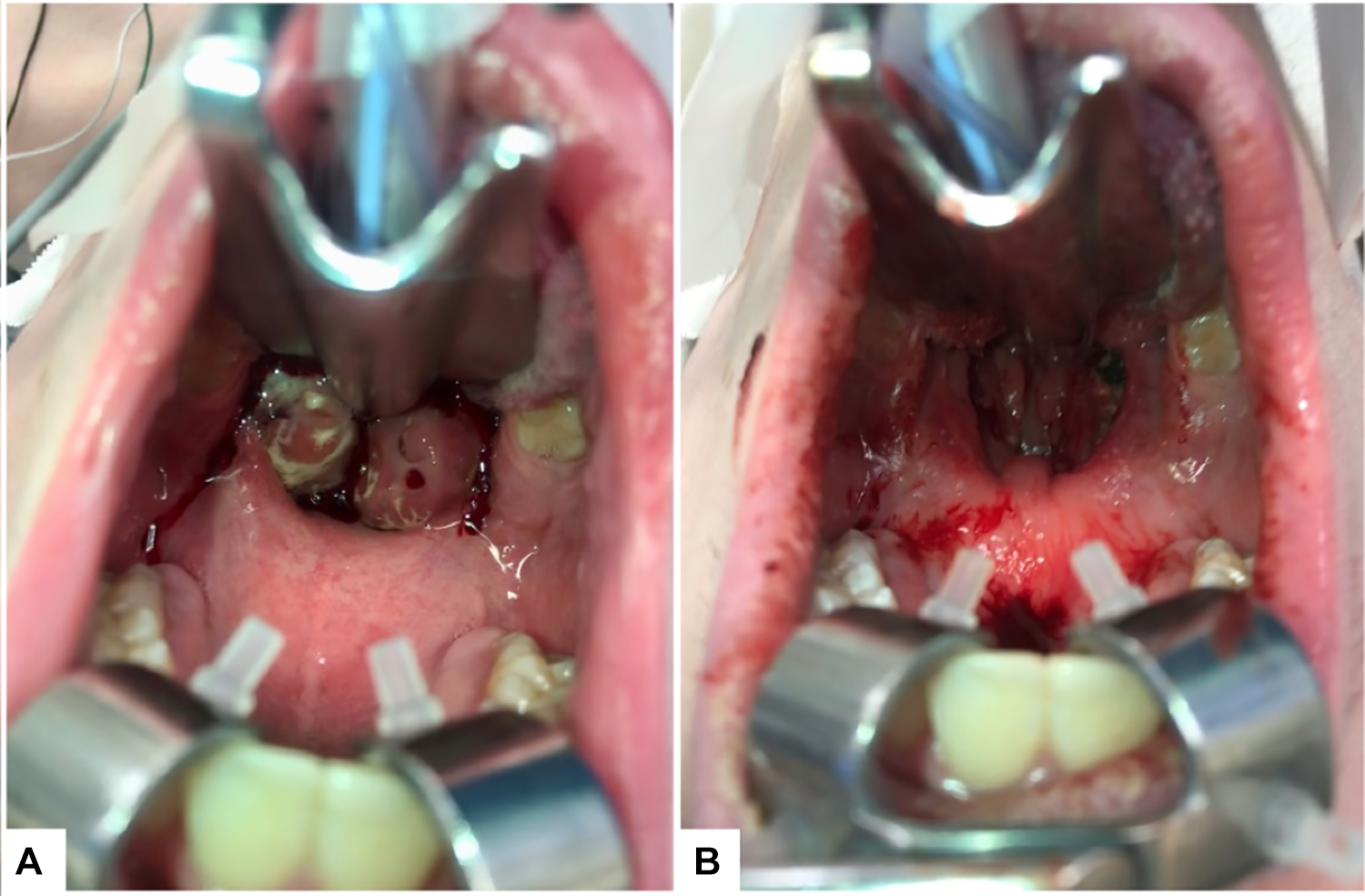
Oropharynx before intracapsular tonsillectomy and adenoidectomy (T&A) demonstrating severe obstruction (A) and after intracapsular T&A with patent airway (B).
Intracapsular T&A by microdebrider included induction under general anesthesia with orotracheal intubation. The right and left tonsils were removed sequentially by intracapsular tonsillectomy down to the capsule. Adenoids were also shaved using microdebrider at 1500. Hemostasis was obtained with suction cautery on the first side, prior to proceeding in the second side. Quikclot packing was placed in each tonsillar fossae and adenoid pad and subsequently removed. Adequate hemostasis was achieved prior to removal of the endotracheal tube by anesthesia.
Of the potential sequelae of MN, including fevers, fatigue, cervical lymphadenopathy, and hepatosplenomegaly, it is airway obstruction that often leads to hospitalization for aggressive medical management. 1 When significant tonsillar hypertrophy leads to persistent upper airway obstruction, surgical interventions should be considered. 2 Adenoidectomy can further relieve obstruction in cases with concurrent adenoid blockage. In our patients, intracapsular T&A was essential in relieving obstructive airway symptoms to meet ICU and hospital discharge criteria.
When considering removing tonsils and adenoids in this patient population, the best surgical approach should minimize the risk of hemorrhage. Many past studies have focused on comparing traditional electrocautery tonsillectomy to intracapsular T&A in patients with chronic obstructive airway symptoms, particularly OSA. Intracapsular T&A results in faster recovery time and return to normal diet due to decreased postoperative pain. 3 Slightly increased intraoperative blood loss during intracapsular tonsillectomy technique was found to be of no medical significance. 3 Vicini et al 4 demonstrated significant decreased postoperative bleeding in their microdebrider T&A and a decreased readmission rate of 0.2% in the microdebrider group compared to 6.4% in the electrocautery group.
In our cases of severe obstructive MN tonsillitis, our patients underwent intracapsular T&A with prompt improvement in symptoms including breathing, voice, ability to swallow, and pain. Neither case experienced postoperative bleeding, recurrence of symptoms, or required readmission. In conclusion, we suggest that intracapsular T&A utilizing microdebrider is a preferred option for severe MN with upper airway obstruction refractory to medical management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.