
Abstract

A 37-year-old man complained of recurrent aural fullness in the left ear and requested for placement of a new ventilation tube owing to repetitive middle ear effusion (MEE). He had previously been diagnosed with left-sided MEE and had undergone ventilation tube procedures thrice in the previous 6 years. Regular follow-up visits to several general otolaryngologists and previous nasopharyngoscopy examinations had revealed no conclusive causes of his Eustachian tube dysfunction. Otoscopy examination confirmed the presence of left-sided MEE and a normal appearance of the right side. Nasopharyngoscopy showed smooth nasopharyngeal mucosa without gross tumor lesions; however, a slightly asymmetrical anterior bulging of the left torus tubarius associated with a slit-like obstructive pharyngeal orifice was noted (Figure 1A). Subsequent magnetic resonance imaging showed a well-circumscribed and homogeneous cystic mass lesion, located in the left superior parapharyngeal space, that is, infratemporal fossa (Figure 1B and C), representing an uncommon cause of persistent MEE. The hyperintense T2-weighted and hyperintense T1-weighted features suggest its proteinaceous fluid content.
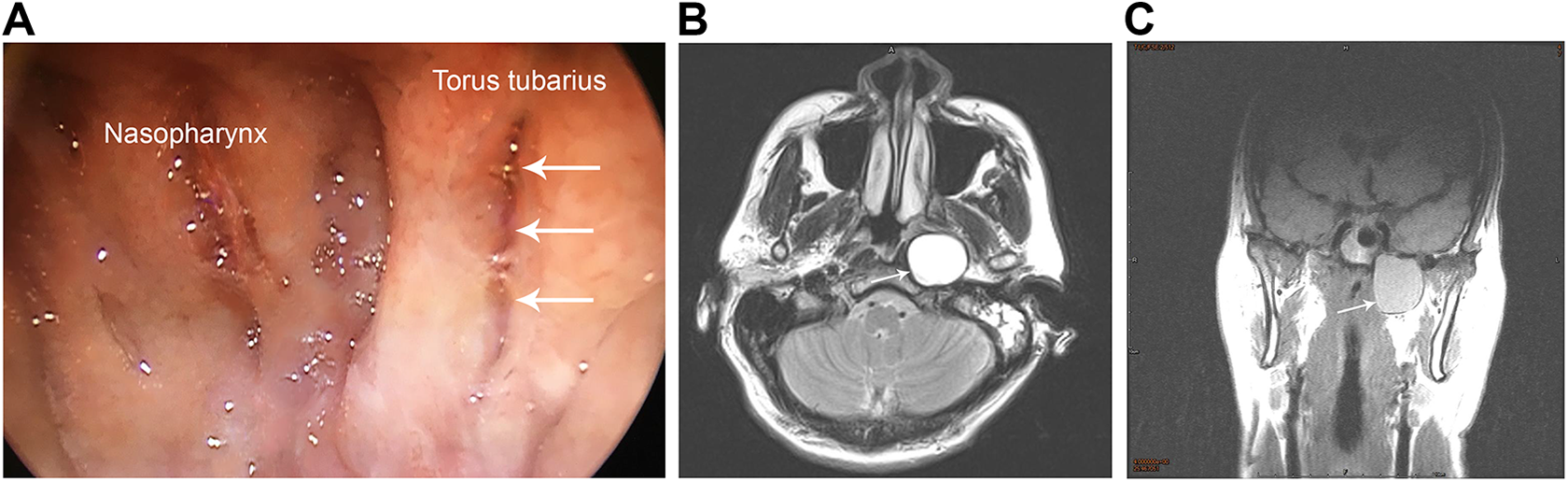
A, Nasopharyngoscopy revealed the left torus tubarius apparently pushed anteriorly, and the pharyngeal orifice showed a slit-like appearance (arrows). B, Axial T2-weighted MRI showed a well-circumscribed hyperintense lesion in the left superior prestyloid parapharyngeal space (arrow). C, Coronal T1-weighted scan revealed a relatively hyperintense (compared with muscle) cystic lesion (arrow) lying in the left infratemporal fossa and pushing the carotid sheath posterolaterally. MRI indicates magnetic resonance imaging.
Considering the morbidity and potentially adverse effects of an aggressive surgical procedure, 1 the treatment choice for this patient was nasopharyngeal navigator-assisted endoscopic marsupialization. For preventing unmanageable complications, we excluded carotid artery aneurysm, hemangioma, and lesions from the central nervous system based on imaging results obtained before the surgery. Fluid content was confirmed during operation, and histopathology revealed an epithelial lining cyst. At the 10-month follow-up, the patient remained asymptomatic and MEE free.
The differential diagnosis of fluid-containing cystic lesions in the parapharyngeal space should include branchial cleft cyst, cystic hygroma, and oncocytic cyst. 2 Cystic hygroma, characterized by dilated lymph channels with endothelial lining, and oncocystic cysts, characterized by oncocytic epithelium with eosinophic cytoplasm, were excluded based on histopathology in the present case. Both image study and histopathology suggested the presence of a branchiogenic cyst. Previous literatures also reported branchial cleft cyst in the parapharyngeal space, causing symptoms such as MEE, sore throat, and cranial nerve palsies that lead to dysphagia and dysarthria.2-4
Persistent unilateral MEE should alert physicians regarding possible noninflammatory, neoplastic causes that compromise Eustachian tube function. Tumors such as nasopharyngeal carcinoma should be excluded first because it shares several symptoms with MEE at its initial presentation. 5 It is noteworthy that endoscopic views of a smooth nasopharyngeal mucosa tend to overlook possible submucosal or deep neoplasms adjacent to the Eustachian tube orifice, as observed in the present case. In the aspect of anatomy, the Eustachian tube is composed of 2 portions, the bony portion, which lies within the petrous part of the temporal bone, and the cartilaginous portion, which lies within the infratemporal fossa and attaches to the sphenoid bone superiorly. 6 Therefore, the differential diagnosis of persistent unilateral MEE should include not only the nasopharyngeal level or luminal malfunction but also mass lesions located at the infratemporal fossa or the petrous part of the temporal bone. 7 Moreover, communication of the subarachnoid space with the middle ear can be a nonobstructive cause of MEE. The present case highlights the importance of thorough head and neck examinations and radiographic evaluations in patients with unexplained persistent unilateral MEE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.