
Abstract
Introduction:
The aim of the current systematic review is to update the pooled survival outcome of patients with T2 glottic carcinoma treated with either laser surgery (CO2 transoral laser microsurgery [CO2 TOLMS]), radiotherapy (RT), or open partial laryngectomy (OPL).
Methods:
A systematic search was performed using the MEDLINE database, Scopus, and Google scholar. The inclusion criteria were studies of patients with T2N0 glottic tumor, treated with either primary CO2 TOLMS, definitive curative RT, or primary OPL, and with reported oncological outcome at 5 years calculated with a Kaplan-Meier or Cox regression method.
Results:
The results of the current review show that local control (LC) is higher with OPL 94.4%, while there are no differences in LC at 5-year posttreatment for patients treated with RT, compared to those treated with CO2 TOLMS (respectively, 75.6% and 75.4%). Primary treatment with OPL and CO2 TOLMS results in higher laryngeal preservation than primary treatment with RT (respectively 95.8%, 86.9%, and 82.4%).
Conclusion:
First-line treatment with OPL and CO2 TOLMS should be encouraged in selected T2 patients, because it results in higher laryngeal preservation and similar LC compared to primary treatment with RT. The involvement of the anterior commissure in the craniocaudal plane and T2b impaired vocal cord mobility have a poorer prognosis and LC compared to patients with T2a tumors for both CO2 TOLMS and RT.
Keywords
Introduction
Early glottic cancer (Tis-T2) is a highly treatable disease with excellent survival rates. Many studies examined treatment outcomes for “early stage” laryngeal cancer, grouping those treated for carcinoma in situ (Tis), T1a, T1b, and T2 tumors, but most of the data for early laryngeal cancer are dominated by T1 and Tis cases. 1,2 However, T1 and T2 glottic cancer are heterogeneous with different growth rates and tendency to infiltrate, and the therapy achieves different results in terms of both oncological and functional outcomes.
Available treatment options include CO2 transoral laser microsurgery (CO2 TOLMS), open partial laryngectomy (OPL), or radiotherapy (RT). To date, there is no clear evidence regarding the effectiveness of surgical treatment (CO2 TOLMS and OPL) over RT, including a recent Cochrane analysis. 1 -6
The aim of the current systematic review is to compare single-modality treatments for patients with T2 glottic carcinoma through the analysis of survival outcomes, local control (LC), and laryngeal preservation (LP) in patients treated with either CO2 TOLMS, RT, or OPL.
Materials and Methods
Search Strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 2 independent researchers conducted a literature search on articles published as of August 2019 using 3 different databases (PubMed, Scopus, and Google Scholar) with combinations of the following terms: laryngeal cancer, early glottic carcinoma/tumor, laryngeal squamous cell carcinoma, CO2 TOLMS, RT, and OPL on articles published between January 1990 and August 2019.
Eligibility and Inclusion Criteria
The inclusion criteria were clinical studies in patients with glottic squamous cell carcinoma staged as a T2N0 according to the Union for International Cancer Control’s (UICC) TNM Classification of Malignant Tumours—8th edition 7 treated with either primary CO2 TOLMS, curative RT, or primary OPL, and with reported oncological outcomes at 5 years calculated with a Kaplan-Meier or Cox regression method. Exclusion criteria were articles not written in English, studies with less than 10 patients, with concurrent chemoradiotherapy, those describing surgery combined with adjuvant therapy, and those describing surgery or RT as salvage therapy.
Data Extraction
Title and abstract of selected papers were carefully read according to the inclusion and exclusion criteria, and duplicates were removed. The full text of the included studies was reviewed with extraction of following data: (1) patient number, (2) average follow-up time (months), (3) treatment, and (4) 5-year oncological outcome in terms of LC and LP.
Study Quality
The levels of evidence of the included articles were scored according to the standards by Wasserman et al 8 as follows: level I: randomized controlled trials, level II: prospective study with internal control group, level III: retrospective study with internal control group, level IV: case series without an internal control group, and level V: consensus or expert opinion without critical appraisal.
Results
Search Results
The results of the search are summarized in Figure. 1. The initial search identified 3464 studies on MEDLINE database, Scopus, and Google scholar. Articles published after the 1990s were selected and imported into a reference management software (Endnote, Clarivate Analytics). After the removal of duplicates, 2258 publications were identified. Papers were screened in title and abstract, and 249 manuscripts were reviewed in full text. Sixty-one studies met the inclusion criteria; of these, 38 RT papers, 19 CO2 TOLMS studies, and 4 OPL article provided 5-year oncological outcome data for 1452 patients treated with CO2 TOLMS, 3365 patients treated with RT, and 366 patients treated with OPL.
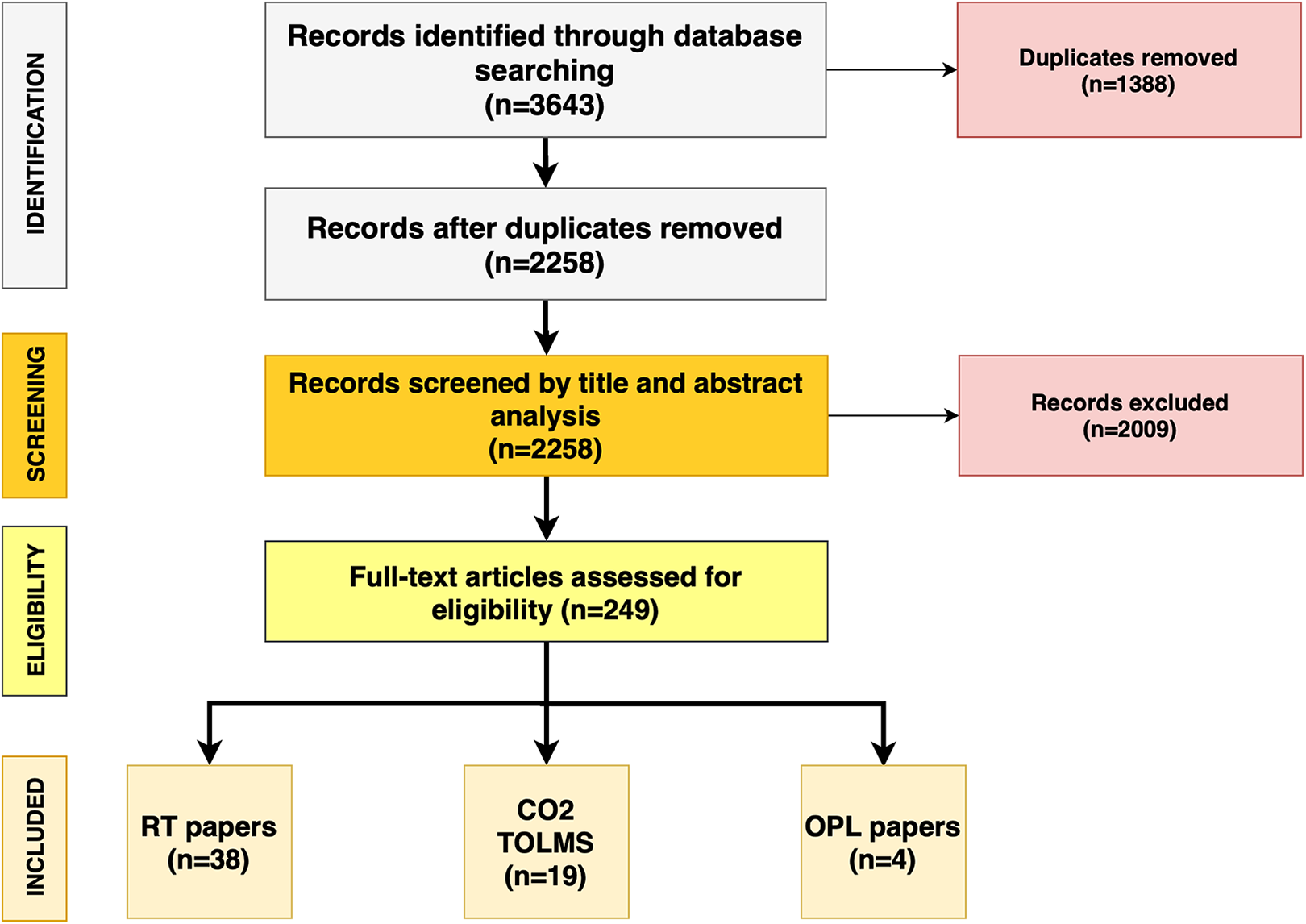
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram followed in this review. The diagram shows the information flow through the different phases of the review and illustrates the number of records that were identified and included.
Study Characteristics
All 61 included studies were published in peer-reviewed journals and were case series without an internal control group, a level IV evidence. No randomized controlled trials studies were identified.
Oncological Outcomes
Tables 1, 2, 3, and 4 show the oncological results of patients treated with either CO2 TOLMS, RT, or OPL in the studies included in this systematic review. The results of the analysis show that weighted averages of LC was higher with OPL (94.4%), while there were no differences in LC at 5 years for patients treated with RT, compared to those treated with CO2 TOLMS (respectively, 75.6% and 75.4%). Primary treatment with OPL and CO2 TOLMS resulted in higher LP in the long term compared to primary treatment with RT (respectively, 95.8%, 86.9%, and 82.4%).
Oncological Outcomes of Patient Treated With Radiotherapy.
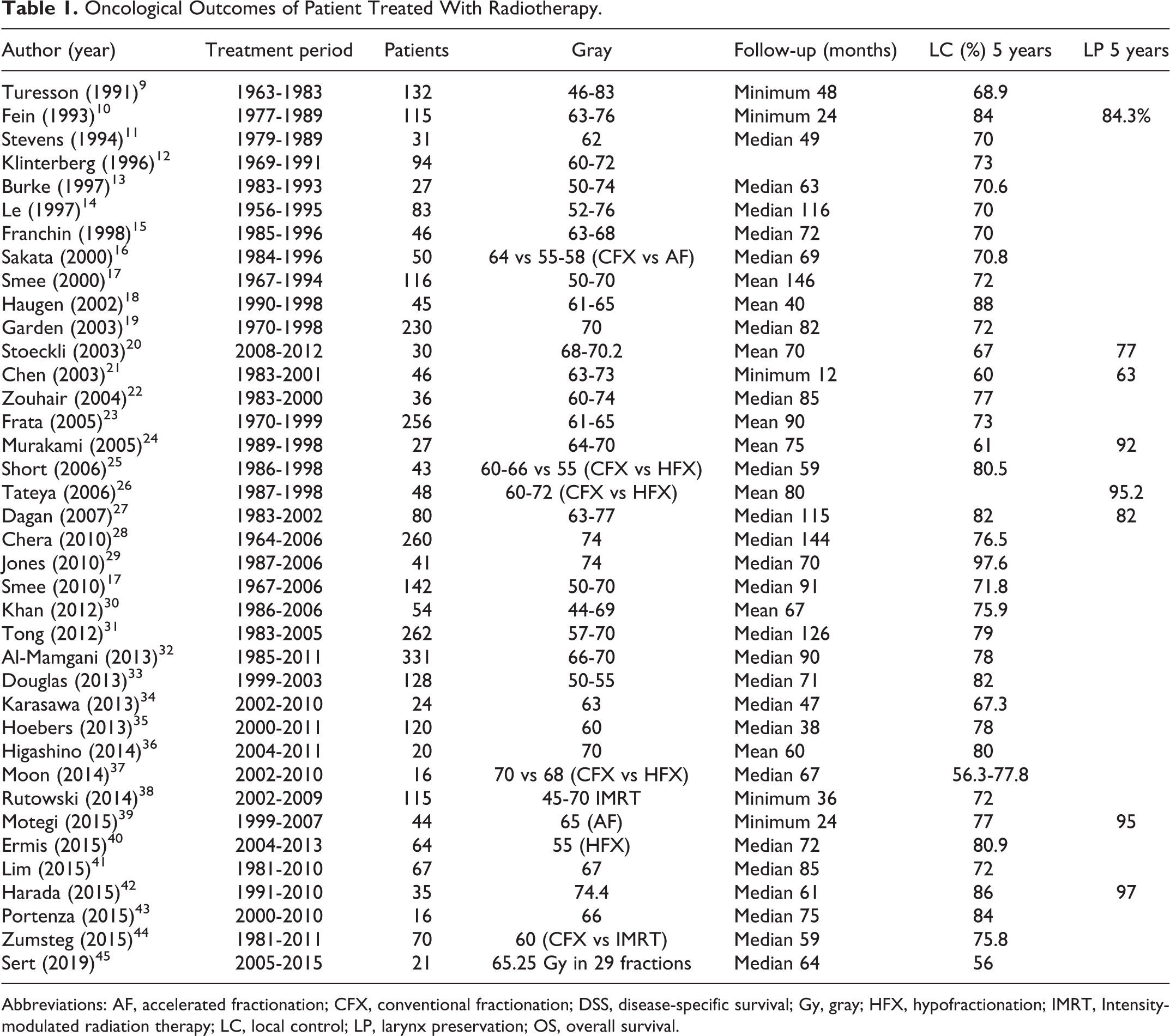
Abbreviations: AF, accelerated fractionation; CFX, conventional fractionation; DSS, disease-specific survival; Gy, gray; HFX, hypofractionation; IMRT, Intensity-modulated radiation therapy; LC, local control; LP, larynx preservation; OS, overall survival.
Oncological Outcomes of Patient Treated With CO2 Transoral Laser Microsurgery.
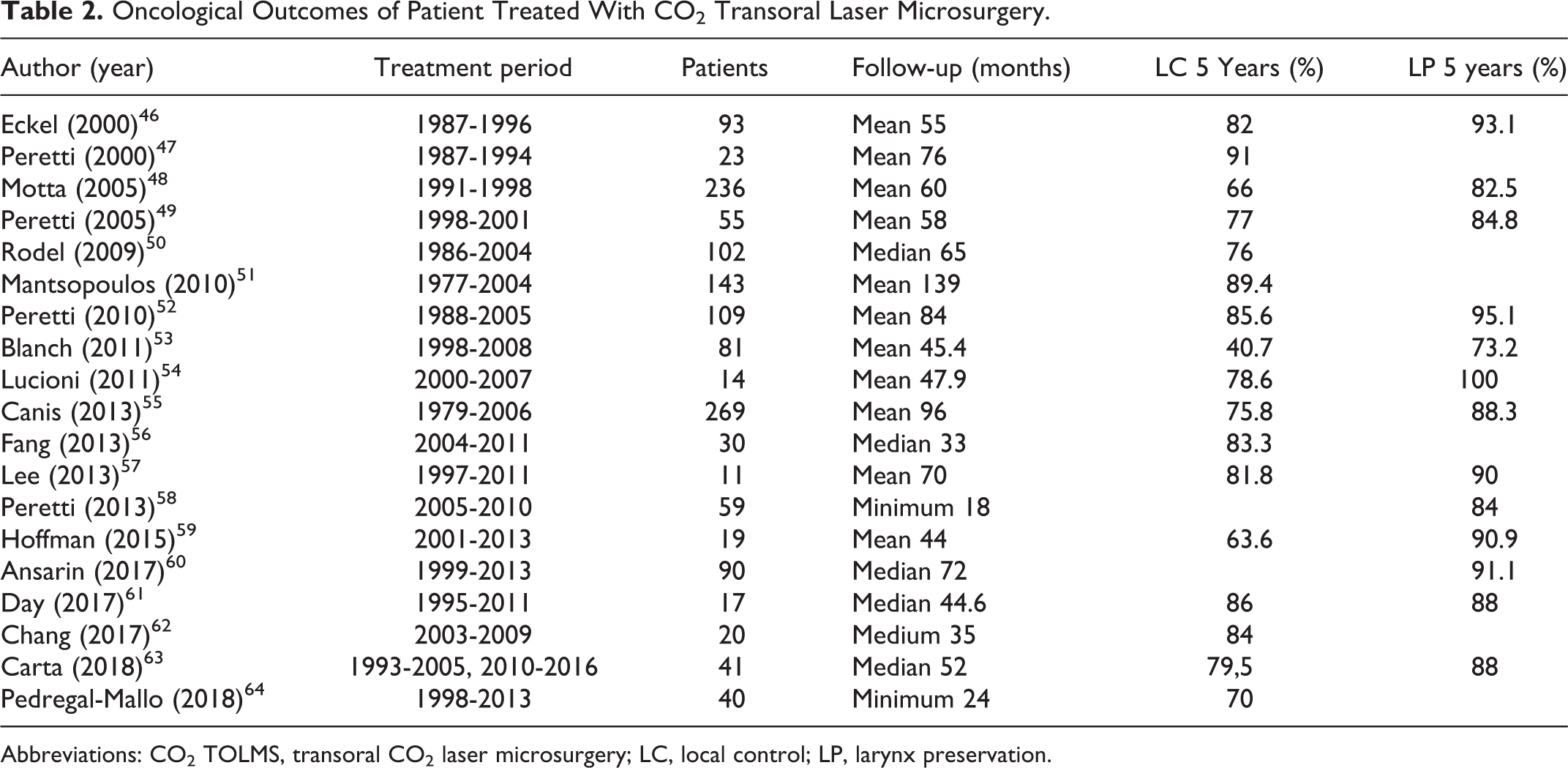
Abbreviations: CO2 TOLMS, transoral CO2 laser microsurgery; LC, local control; LP, larynx preservation.
Oncological Outcomes of Patient Treated With OPL.

Abbreviations: LC, local control; LP, laryngeal preservation; OPL, open partial laryngectomy.
Weighted Averages of the Oncological Outcomes for CO2 TOLMS, RT, or OPL.
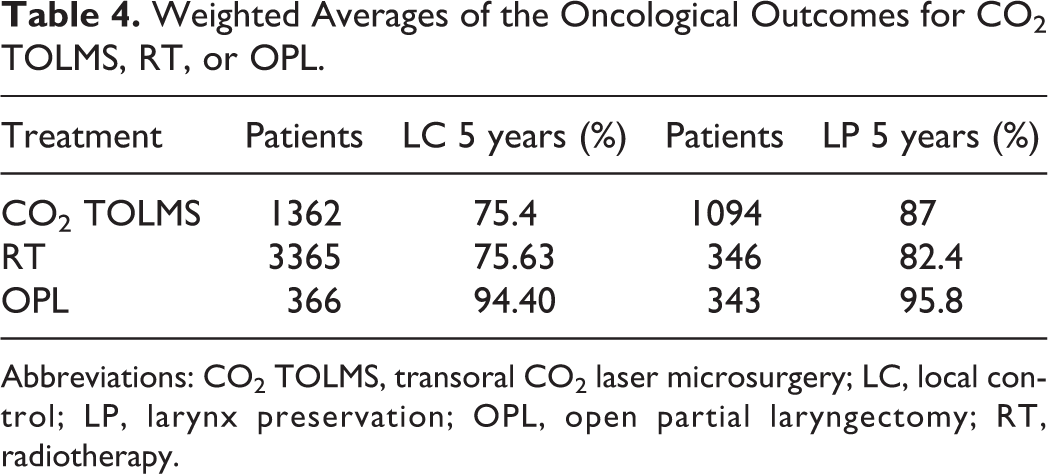
Abbreviations: CO2 TOLMS, transoral CO2 laser microsurgery; LC, local control; LP, larynx preservation; OPL, open partial laryngectomy; RT, radiotherapy.
Discussion
The main treatment modalities for early glottic carcinomas include CO2 TOLMS, RT, and OPL; however, there is no clear evidence regarding the effectiveness of one treatment over the other. 1 -4 The results of the current review show that weighted averages for LC and LP is higher with OPL (94.4% and 95.8%) compared to CO2 TOLMS (75.4% and 87%) and RT (75.6% and 82.4).
Our systematic review shows that the number of patients treated with OPL was lower than that of patients treated with CO2 TOLMS and RT; this suggests that the role of open surgery for management of laryngeal cancer has gradually decreased during the past 20 years probably because of the worse functional outcomes as voice quality and swallowing results. The development of CO2 TOLMS and improvements in delivery of RT have replaced the previously standard techniques of OPL for early cancer. In the recent years, CO2 TOLMS has received a great consensus, as the use of CO2 TOLMS as a primary treatment is more cost-effective than OPL or RT, 69 -71 and it is usually performed as a day case procedure. Moreover, a number of optical and molecular examining technologies have been developed over the last few years to improve tumor detection and tumor margin identification. One of the most implemented techniques in clinical practice is narrow-band imaging (NBI); a significant reduction of positive superficial margins was found in patients treated with intraoperative use of NBI (52%) compared to patients treated without intraoperative NBI (28.6%; P < .05). 72
Laryngeal Preservation
The CO2 transoral laser microsurgery resulted in higher LP compared to RT; this can be explained by the preservation of physiological cartilage barriers. Furthermore, laser surgery can be repeated or followed by other treatment protocols (eg, RT or OPL) in patients with recurrent disease. Contrarily, both RT and OPL in primary glottic carcinoma may lead to treatment limitations in case of recurrence, making organ preservation more unlikely. In addition, patients undergoing salvage surgery post-RT have a greater number of complications than patients post-CO2 TOLMS. Overall complication rate in salvage surgery post-RT ranges from 5% to 78% with the most common complication being pharyngocutaneous fistula formation occurring in as many as 73% of cases in the salvage setting. 73,74
Local Control
Evidence confirms that patients with T2b and vocal cord mobility have a poorer prognosis and LC compared to patients with T2a tumors for both CO2 TOLMS 3,55 and RT 9,10,13,27,28,30,75,76 while data on OPL are not enough to evaluate the oncological outcomes in these patients. In a recent case series, Succo et al 65 affirmed that OPL is safer in case of T2b compared to CO2 TOLMS; however, it led to more dysfunctional sequelae. The authors concluded that OPL should be performed in selected patients affected by glottic cT2 with impaired mobility of vocal cords and suspected extension to the paraglottic space (PGS). Rucci et al 77 observed that the dorsal compartment of the glottic site is in close proximity to the paraglottic space. The internal cricoarytenoid ligaments oppose for a short length of time to the penetration of early glottic cancer into the paraglottic space toward the cricoarytenoid joints. Lesions invading the paraglottic space should be correctly classified as T3 during the preoperative evaluation with a transnasal flexible videofiberscope and magnetic resonance imaging. 78 Poorer prognosis seems to be associated mainly with tumor infiltration of the posterior paraglottic space resulting in fixation of the arytenoid joint and not with impaired mobility from vocal fold muscle infiltration or pure tumor bulk. 6
Involvement of the Anterior Commissure
The treatment of the T2 glottic cancer with involvement of anterior commissure (AC) is also controversial. Laccourreye et al 79 found that among 416 patients with T1 or T2 laryngeal cancers undergoing vertical partial laryngectomies, the failure rate was 23% if the AC was involved; higher than at other anatomic subsites. Studies on CO2 TOLMS 52 -54,58,59,63 and studies on RT 20,21,24,25,76 analyzed the involvement of the AC and concluded that its involvement did not result in a significantly lower overall survival rate. However, Hoffmann et al (96 patients) and Carta et al (105 patients), in large sample-sized studies, revealed a significantly increased risk for local recurrences in patients with extensive infiltration of the AC. 59,63,80
The vertical plane of the AC has been identified as a laryngeal subsite at risk for local treatment failures. 81 -84 In the ventral compartment, cancer can easily diffuse superficially along the ventral mucosa containing blood vessels and glands; this diffusion usually follows a cranial-to-caudal direction. Moreover, if cancer reaches in depth the Broyles tendon, it can invade adjacent structures. Therefore, an early-stage carcinoma with involvement of the AC could penetrate the cartilage transforming a T1 tumor into a T4 switch, thus representing a contraindication for CO2 TOLMS. The impact of the AC involvement on prognosis in laryngeal cancer remains a topic with inconsistent results in the literature; a detailed stratification of tumors involving the AC needs to be investigated in further studies for all treatment modalities. 85
Limits of the Study
The main limitation of this review is the vast heterogeneity of selected studies. Radiotherapy studies have a large variety in technique, fraction size, and overall dose, while CO2 TOLMS studies did not describe which resections were performed during surgery. Furthermore, there are no randomized trials or comparison studies; all the selected studies are retrospective case series. For this reason, formal statistical analysis and meta-analysis are inappropriate. It is very important to underline that in the majority of studies on CO2 TOLMS, there was some selection of patients. Large T2 tumor or tumor with the involvement of AC may not be suitable for a transoral approach, and treatment must be individualized according to patient anatomy. Finally, there was heterogeneity in treatment details, treatment period, study design, and follow-up for both treatment modalities.
Conclusions
The current first-line treatments for early laryngeal cancer are CO2 TOLMS and RT, while the role of OPL has greatly diminished in the last 20 years. This review suggests that CO2 TOLMS should be encouraged in selected T2 patients, because LC is comparable but primary treatment with CO2 TOLMS results in higher LP compared to primary treatment with RT. In conclusion, data suggest that involvement of the AC in the craniocaudal plane and T2b impaired vocal cord mobility have a poorer prognosis and LC compared to patients with T2a tumors for both CO2 TOLMS and RT. Open partial laryngectomy should be proposed in selected patients affected by glottic cT2 with impaired mobility of vocal cords and suspected extension to the PGS. Further studies on cancers with the involvement of AC and impaired vocal cord are necessary to clarify their impact on oncological outcomes, and prospective randomized controlled studies for both treatment modality are required to confirm these results.
Footnotes
Authors’ Note
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.