
Abstract
Objectives:
(1) To determine how otologic/neurotologic surgeons counsel patients with superior semicircular canal dehiscence (SSCD). (2) To understand the plethora of presenting symptoms associated with SSCD and appropriate management. (3) To suggest appropriate management; oftentimes avoiding surgery.
Methods:
This was a survey study of both community and academic physicians. A 23-question survey was distributed to all members of the American Neurotological (ANS) and American Otologic Societies (AOS) via email in the Fall of 2018. A total of 54 responses were received from a possible pool of 279 for a response rate of 19.4%. Inferences were made about the population through sample proportions and confidence intervals.
Results:
All respondents use computed tomography (CT) in diagnosing SSCD and 11.1% use CT exclusively. Cervical vestibular evoked myogenic potential (VEMP; 77.8%) are used more often than ocular VEMPs (38.9%). Magnetic resonance imaging (7.4%) is used infrequently; 96.3% of surgeons surveyed have seen patients with SSCD on imaging that are asymptomatic. Following surgical treatment, respondents reported balance issues and mild-to-moderate high-frequency sensorineural hearing loss (88.4%); 32.6% reported that the majority (>50%) of their patients needed further intervention after surgery, typically aggressive vestibular rehabilitation.
Conclusions:
There is a discrepancy in the systematic approach to SSCD between both the surgeons and the published literature. Patients with SSCD on ultra-high-resolution CT may have myriad symptoms while others are asymptomatic, and surgery may lead to additional complications. We will present a methodical recommendation to assist in the management of patients with SSCD depending upon their symptoms. This may improve patient selection, counseling, and outcomes.
Keywords
Introduction
Since its initial description in 1998, the diagnosis and management of superior semicircular canal dehiscence (SSCD) has been challenging. Radiographic evidence of SSCD is relatively common; however, the condition may present with myriad symptoms—or none at all—thus lending to its diagnostic and management difficulties. 1 Several surgical approaches have been described with varying results in terms of efficacy and complications. Pooling the experiences of practicing otolaryngologists may lead to better outcomes in patients with this often-debilitating condition.
Symptoms of SSCD
In the original article, SSCD was thought to primarily manifest with vestibular symptoms due to the introduction of a third mobile window into the inner ear. 1 Among these symptoms were sound-induced vertigo or oscillopsia (Tullio phenomenon), pressure-induced vertigo (Hennebert sign), chronic disequilibrium, and unsteadiness. 1 Since then, auditory symptoms, including conductive hearing loss, conductive hyperacusis, pulsatile tinnitus, aural fullness, ocular-induced sounds, migraine associated symptoms, and autophony, have been described.2-4 Bone conduction hyperacusis, autophony, pulsatile tinnitus, vertigo, and aural fullness are the most common of these symptoms.4-7 Sound- and/or pressure-induced vertigo and oscillopsia, bone conduction hyperacusis, and chronic disequilibrium are the most debilitating and troubling symptoms for patients. 7 Despite the wide array of symptoms described in SSCD, the prevalence lacks a clear pattern. Some patients with confirmed SSCD on radiological imaging present with only 1 symptom in isolation, such as disabling aural fullness, or a lack of symptoms altogether. This lack of a symptom pattern contributes to controversy regarding the diagnosis, presentation, and management of SSCD.
Diagnosis and Management of SSCD
The gold standard for diagnosis of SSCD is an ultra-high-resolution collimated helical computed tomography (CT) scan with reformation of images in the plane of the superior semicircular canal (SSC). Another modality includes T2-weighted fast-spin echo magnetic resonance imaging (MRI).4,8-10 On clinical examination, patients may have lateralization of Weber test to the symptomatic ear as a result of conductive hearing loss with normal stapedius reflexes, a negative Rinne test with bone conduction greater than air, Tulio phenomenon, and Hennebert sign.3,4,6,8 Demonstration of a third mobile window include negative bone conduction thresholds on pure tone audiometry, low cervical vestibular evoked myogenic potential (VEMP) thresholds, high ocular VEMP amplitudes, and elevated summating potential to action potential ratios on electrocochleography (ECOG) without sensorineural hearing loss.5,7,11-15
Management of SSCD ranges from noninvasive to invasive options. Noninvasive options include extensive counseling, medications, and vestibular rehabilitation. Invasive options include surgical plugging and/or resurfacing of the dehiscent bone over the SSC through transmastoid or middle cranial fossa (MCF) approaches or a round window (RW) plugging procedure. Among these, plugging and resurfacing through the MCF approach seems to be the most effective approach, thus most commonly utilized. 16 Other colleagues have reported success with transmastoid procedures without plugging of the SSC. 17 Surgical treatment is usually reserved for patients with debilitating or disabling symptoms, although these specific symptoms remain unclear.
The Present Study
Currently, there are no established guidelines for the diagnosis and management of SSCD. Given the plethora of symptoms and the range of diagnostic modalities and treatments for these patients, it appears that many practicing otolaryngologists may offer different options for patients. Thus, a survey was administered to glean insight from the members of the AOS and AOS regarding the details and nuances of the strategies for helping patients with SSCD. These strategies were then compared to the current literature regarding diagnosis, presentation, and management of SSCD.
Patients and Methods
Survey and Distribution
The Institutional Review Board (IRB) at Advent Health and University of Central Florida College of Medicine deemed this study as research involving surveys and no direct human involvements and was thus exempt from the IRB process. A review of the literature published between 1998 and 2018 pertaining to SSCD presentation, management, and outcomes was completed. The observations from this review were used in conjunction with clinical experience to inform the questions of a 23-item survey (Appendix A) created with Qualtrics (Qualtrics, Provost, Utah). The survey covered topics including patient presentation, workup, management preferences, and operative outcomes. This was distributed to 279 practicing otolaryngologists via the biannual survey administered by the ANS and AOS in October 2018. The survey remained open until May 2019. Fifty-four responses were collected and recorded anonymously by the Qualtrics survey platform.
Statistical Analysis
The distributions of responses were recorded and analyzed using descriptive statistics. Further inferences about the population were made through sample proportions and CIs. SAS (SAS Institute, Cary, North Carolina) was used for all statistical calculations.
Results
Survey Response Population
Fifty-four responses were collected out of a pool of 279 practicing otolaryngologists for a response rate of 19.4%: 14.8% (± 9.5%) of respondents make less than 5 diagnosis of SSCD per year, 35.2% (± 12.7%) make 6 to 10 diagnoses per year, 24.1% (± 11.4%) make 11 to 20 diagnoses per year, and 25.9% (± 11.7%) make over 20 diagnoses per year.
Symptoms and Patient Characteristics
According to our sample of otolaryngologists (n = 54), almost all patients presenting with sound-induced vertigo (98.2% ± 3.6%) and pressure-induced vertigo (90.7% ± 9.3%) should undergo further evaluation for the possibility of SSCD (Table 1; Figure 1A). Other common presenting symptoms warranting evaluation include pulsatile tinnitus (85.2% ± 9.5%), bone conduction hyperacusis (81.5% ± 10.4%), autophony (83.3% ± 9.9%), conductive hearing loss (64.8% ± 12.7%), and aural fullness that does not respond to treatment for eustachian tube dysfunction (57.4% ± 13.2%).
Approximately how many patients do you diagnose with SSCD per year?
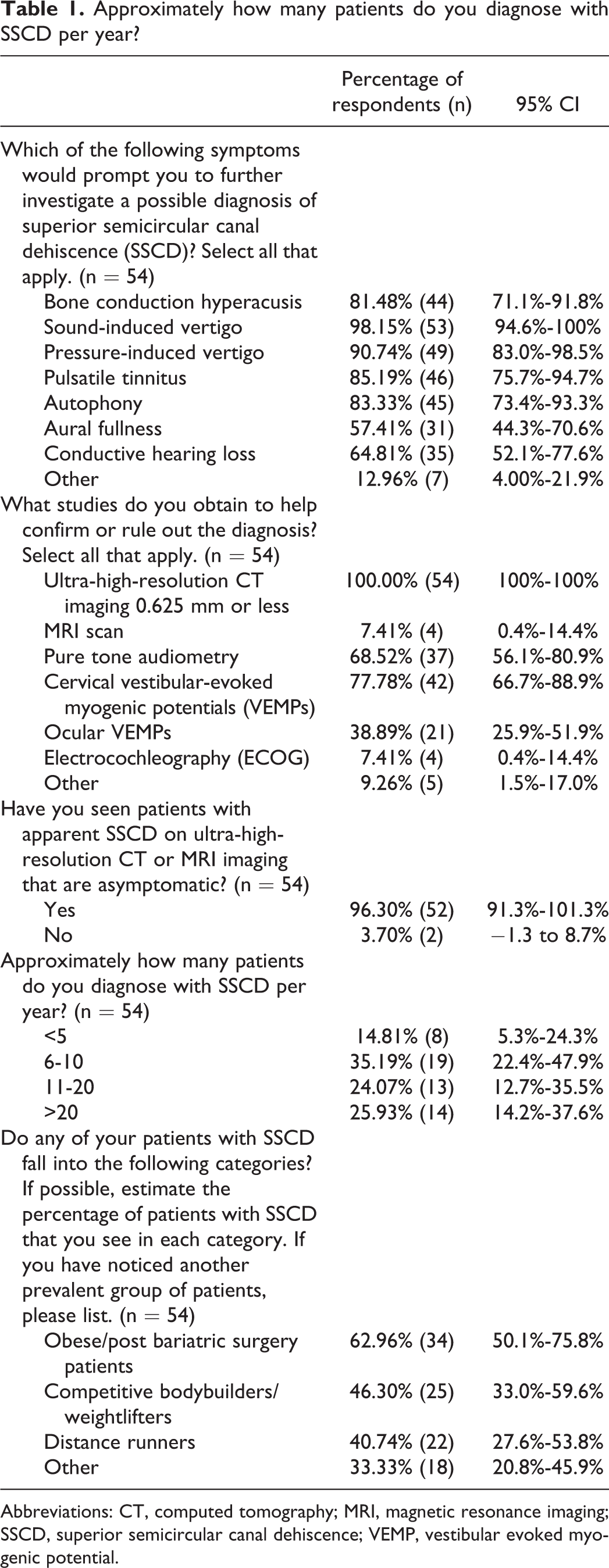
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; SSCD, superior semicircular canal dehiscence; VEMP, vestibular evoked myogenic potential.
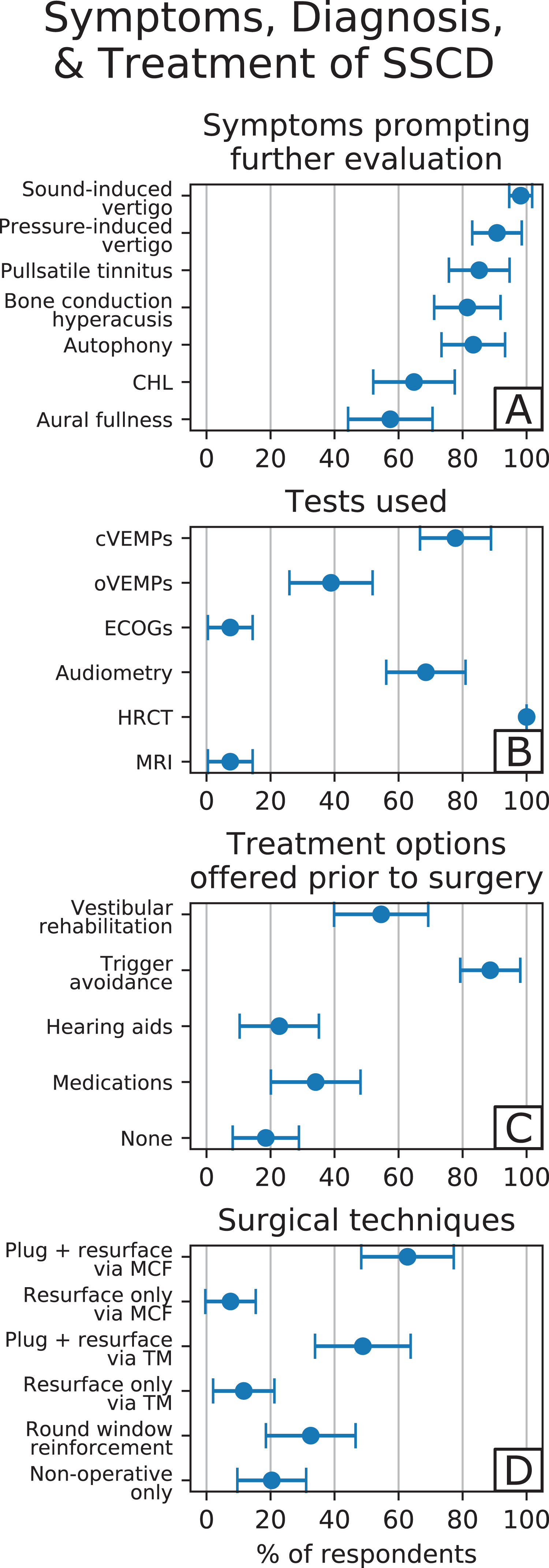
Symptoms, diagnosis, and treatment of superior semicircular canal dehiscence (SSCD). Dots represent the percentage of respondents indicating usage of the corresponding modality, and the lines are the calculated confidence intervals for the population derived from the sample. A, Symptoms prompting further evaluation of SSCD. B, Most common diagnostic tests utilized. C, Treatment options offered prior to recommending surgical management of SSCD. D, The most common surgical techniques used for SSCD treatment.
Many surgeons surveyed recommend surgical management for vestibular symptoms (92.6% ± 7.0%) or auditory symptoms (72.2% ± 11.9%) in isolation. Few recommend surgical management for conductive hearing loss (5.5% ± 6.1%) or sensorineural hearing loss (1.9% ± 3.6%) alone. Only 5.5% (± 6.1%) do not recommend surgery for 1 symptom in isolation.
Many patients with SSCD fall under the following categories: obese or post-bariatric surgery (63.0% ± 14.1%), bodybuilders or weightlifters (46.3% ± 13.3%), and long-distance runners (40.7% ± 13.1%). While the exact mechanism of this phenomenon is unknown, one possible explanation could be increased strain induced by extra body mass or the nature of these activities.
Diagnostic Modalities
All respondents (n = 54) use ultra-high-resolution CT imaging with slice sizes of 0.625 mm or less to diagnose SSCD (100%); 11.1% (± 8.4%) use CT alone (Table 1; Figure 1B). However, 96.3% (± 5.0%) of respondents have seen patients with apparent SSCD on CT imaging that are asymptomatic. Additionally, several surgeons admitted to seeing SSCD on CT, operating on these patients and finding no actual SSCD, suggesting that volume averaging in CT scanning remains an issue and hence provides further recommendations toward the thinnest scans possible. A minimal number of respondents use MRI (7.4% ± 7.0%) for diagnosis. To demonstrate the presence of a third mobile window, 77.8% (± 11.1%) use cervical VEMPs, 38.9% (± 13.0%) use ocular VEMPs, 7.4% (± 6.9%) use ECOGs, and 68.5% (± 12.4%) use audiometry. Majority of respondents (83.3%) utilize the combination of CT scans and VEMPs for diagnosis.
Management
Many respondents treat symptoms prior to recommending surgery (81.5% ± 10.4%; Table 2). Common modalities include trigger avoidance (88.6% ± 9.4%), vestibular rehabilitation (54.5% ± 14.7%), medications (34.1% ± 14%), and hearing aids (22.7% ± 12.4%; Figure 1C). Common medications include antiemetics, antihistamines, tricyclic antidepressants, benzodiazepines, and migraine prophylaxis medications.
Survey Results Pertaining to the Indications for Surgical Management of SSCD.
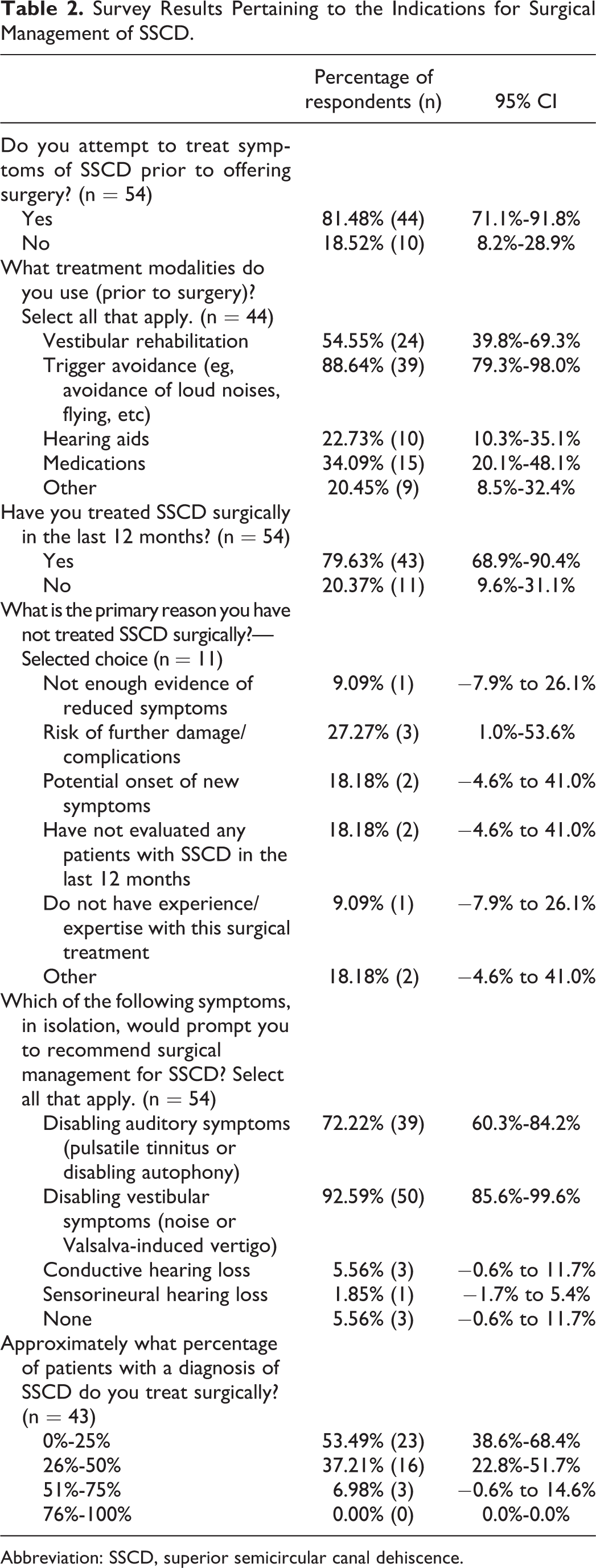
Abbreviation: SSCD, superior semicircular canal dehiscence.
Although 79.6% (± 10.7%) have treated SSCD surgically in the past 12 months, most respondents treat less than half of SSCD patients surgically (90.7% ± 8.7%). Of those who did not treat surgically (n = 11), many feared risk of further damage (27.3% ± 7.9%) and new symptom onset (18.1% ± 22.8%).
Plugging and resurfacing the dehiscent SSC using the MCF (62.8% ± 14.4%) and transmastoid approach (48.8% ± 14.9%) are the most common surgical techniques (Table 3; Figure 1D). Fewer respondents resurface only, without plugging, using both the MCF (7.5% ± 7.9%) and the transmastoid approaches (11.6% ± 9.6%). Additionally, 32.6% (± 14.0%) perform RW reinforcement. The majority of those who plug and resurface using MCF (51.2% ± 18.8%) and transmastoid approaches (47.6% ± 21.4%) have done less than 10 surgeries throughout their entire career.
Survey Results Pertaining to Surgical Approaches to SSCD.
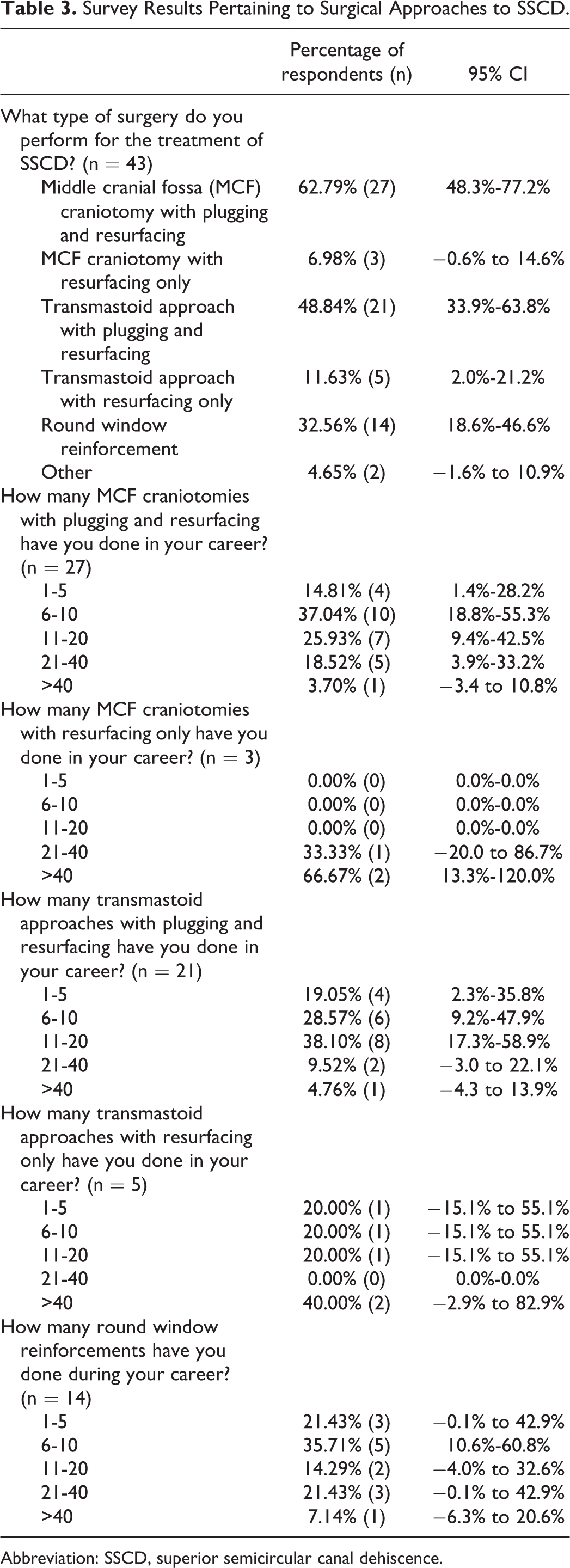
Abbreviation: SSCD, superior semicircular canal dehiscence.
Surgical Outcomes
In all, 32.6% (± 14.0%) of respondents state that over half of their patients require additional treatment after surgery (Table 4; Figure 2A); 20.9% (± 12.2%) see new-onset sensorineural hearing loss in 11% to 30% of patients treated, while all see balance issues (Figure 2B). Of all, 63.2% (± 21.7%) of respondents tell their patients that hearing loss will be permanent, while all respondents tell their patients that balance issues will last less than 12 weeks.
Survey Results Pertaining to the Outcomes Following Surgery for SSCD.
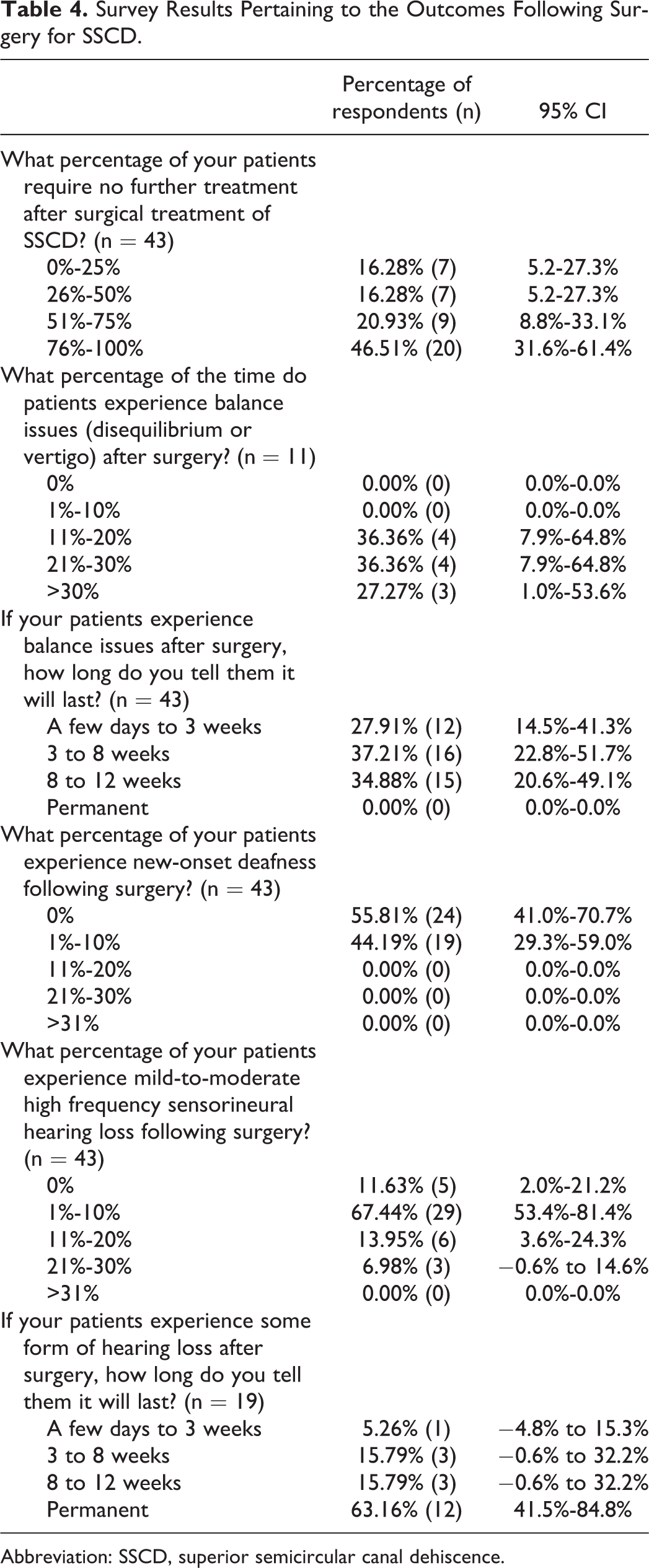
Abbreviation: SSCD, superior semicircular canal dehiscence.
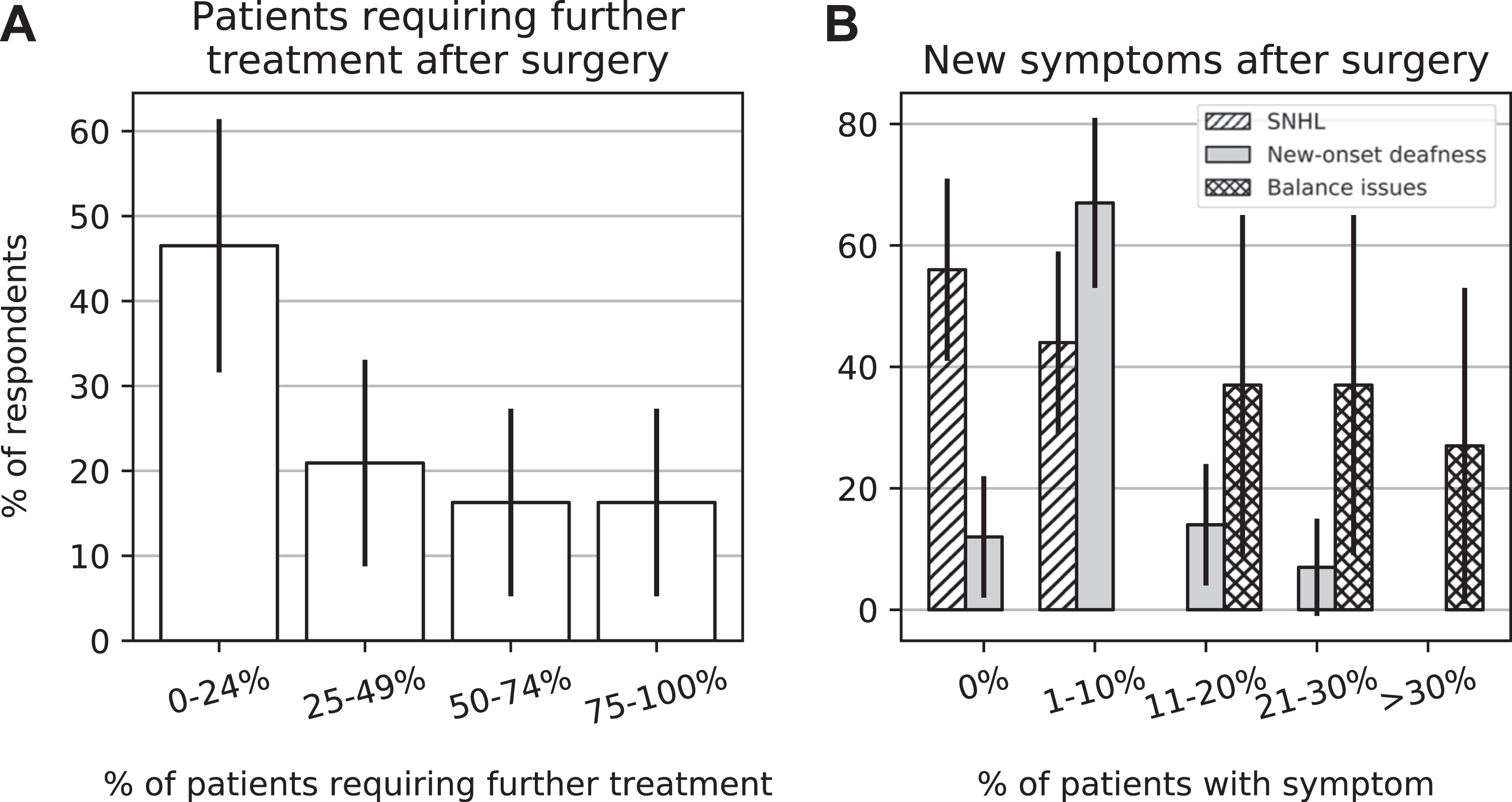
Postoperative outcomes. Postoperative outcomes, including need for additional treatment and the onset of new symptoms. Error bars are the calculated confidence intervals for the population derived from our sample. A, Percentage of patients requiring further treatment after surgery for superior semicircular canal dehiscence (SSCD). B, The percentage of patients with onset of new, specific symptoms after surgical management of SSCD.
Discussion
Patients with SSCD present with a diverse range of symptoms or no symptoms at all, thus creating a diagnostic and management challenge. To better understand these challenges, the practices of survey respondents are compared to a proposed diagnostic criterion for SSCD by Ward and colleagues in 2017, which included at least 1 symptom consistent with SSCD, CT proof of a dehiscence, and at least 1 electrophysiologic test supportive of a third mobile window. 18 This survey reveals that practicing surgeons are following the proposed diagnostic criteria in some cases but extending beyond or falling short in others.
Symptoms in the proposed criteria include bone conduction hyperacusis (ie, autophony), sound-induced vertigo, pressure-induced vertigo, and/or pulsatile tinnitus. 18 These were also the 4 leading symptoms to prompt respondents in this study to evaluate for SSCD. Out of these symptoms, autophony was the least common to prompt further evaluation despite being the most common presenting symptom of SSCD according to the literature.5,19 On the contrary, sound- or pressure-induced vertigo were the most common symptoms to prompt further evaluation of SSCD, but recent studies have revealed that less than half the patients with SSCD experience these symptoms.5,20 Patients—in our study and in the literature—also present with symptoms extending beyond this list, including aural fullness and conductive hearing loss.5,19-21 These symptoms should be considered for addition to the list of symptoms in a proposed diagnostic criteria for SSCD: they are present in nearly half of the patients in some studies and prompt 60% of respondents in this survey to evaluate for SSCD. Similarly, 96.3% of respondents have seen confirmed SSCD on CT imaging in patients who are asymptomatic, indicating that SSCD is often found incidentally in asymptomatic patients. Practicing otolaryngologists should be made aware of the plethora of presenting symptoms of SSCD, or no symptoms at all, to direct diagnoses.
Regarding the imaging portion of the criterion, all respondents in this survey utilized CT to prove dehiscence. Both CT imaging and one test to identify the presence of a third mobile window are recommended. However, 11% of respondents use CT alone in the diagnosis without any additional testing for a third mobile window. This is concerning due to the 80% false-positive rate of CT as documented in the literature. 22 Some argue that CT scans should only be ordered for those with high suspicion for SSCD, not as a screening tool, and should not be used alone in the diagnosis.5,8,18,22 This could result in unnecessary surgical management, as patients should not undergo surgery for SSCD solely based on CT findings. Magnetic resonance imaging is another option for clinicians that is not included in the proposed diagnostic criterion for SSCD. Despite a 96% sensitivity and 98% specificity, only a limited number of respondents utilize this technique. 10 Addition of this test to the proposed criterion should also be considered. This reveals that practicing otolaryngologists may not be utilizing the most efficacious means to diagnose SSCD.
According to the criterion, tests recommended to indicate a third mobile window in SSCD include audiometry, ocular or cervical VEMPs, or electrocochleography, which should be used alongside CT scan to confirm a diagnosis. 18 In this sample, the majority utilize VEMPs over electrocochleography and audiometry. Specifically, respondents use cervical VEMPs more often than ocular VEMPs. However, studies reveal that ocular VEMPs are more suitable than cervical VEMPs in the diagnosis of SSCD.13,15 Additionally, over 20% of respondents do not test the presence of a third mobile window with these tests. One study revealed that the combination of both high-resolution CT and a VEMP test can reduce the false-negative rate, suggesting that VEMP be used as a screening test, even though it can be positive in other disorders, and CT as a confirmatory test. 8 Almost 80% of respondents utilize this combination of tests. This survey reveals that practicing otolaryngologists may not be utilizing adequate third mobile window testing in combination with imaging to appropriately diagnose SSCD.
Otolaryngologists treat SSCD both symptomatically and surgically. According to this survey, options for treatment prior to surgery include trigger avoidance, vestibular rehabilitation, medications, and hearing aids. Patients seek surgical treatment if symptoms are debilitating and symptomatic management is inadequate. According to the literature, these debilitating symptoms are usually vestibular in origin.7,18 However, 72.2% of respondents in this survey offer surgical treatment for auditory symptoms in isolation, which indicates that auditory symptoms are a source of debilitation in these patients. As far as surgical approach, most respondents use either an MCF or a transmastoid approach to plug and resurface the dehiscent canal, which, according to the literature, offers the best possible outcomes.2,4 However, many still solely resurface the dehiscent canal or perform RW reinforcements, resulting in a higher percentage of patients requiring additional treatment after surgery; most have noted that RW plugging helps approximately 25% of their patients, well within the realm of placebo.
Postoperatively, most respondents indicated that over 25% of their patients required further treatment. Additionally, a significant number reported that many patients experience permanent sensorineural hearing loss and balance issues—findings that are consistent with the current literature.7,23 According to these findings, one bothersome symptom preoperatively is often swapped for an additional symptom postoperatively. These symptoms include perturbed vestibular function, benign paroxysmal positional vertigo, new-onset tinnitus, and oscillopsia.2,7,19,24-26 This requires serious consideration and strong counseling of our patients to ensure they have realistic expectations. Consequently, many respondents have not treated SSCD surgically in the past 12 months due to the risk of further damage and potential onset of new symptoms. Future studies should clearly define the symptoms warranting surgical treatment to ensure that benefits of surgery outweigh the risks.
In addition to symptoms, diagnostic modalities, and management of SSCD, this research reveals interesting characteristics and potential modifiable risk factors of patients with the condition. Over half the respondents notice that many of their patients with SSCD are obese or post-bariatric surgery. Under half notice bodybuilders or weightlifters and long-distance runners. The latter supports the theory that SSCD could be due to minor head trauma or barotrauma. 4 This could not only lead investigators to discover the potential etiology of SSCD but also lead practicing otolaryngologists to assist patients in modifying risk factors.
Participation in this study was limited to active members of the ANS and AOS, introducing sampling bias and limiting generalizability beyond the societies. A recall bias would also be present if respondents relied on their memory rather than records to answer questions. Additionally, there may be a selection bias if members of the ANS and AOS who do not manage patients with these symptoms declined to respond. Our response rate may in turn be much higher than 20% when excluding those who do not see this condition from the total number of surgeons who received this survey.
Although this study lacks the ability to define the exact symptoms and test results warranting surgical treatment due to the aforementioned limitations, there do appear to be several gaps between the practices solicited by respondents and the practices described in the literature. Narrowing these gaps could help to ensure the benefits of surgery outweigh the risks. In general, the minimum requirement for offering surgical options should include the presence of debilitating vestibular symptoms, radiographic evidence of SSCD, and a positive third-window test. Further evaluation of this criteria—specifically on the surgical outcomes of patients with all 3 findings—would provide physicians with a more definitive guideline regarding SSCD management.
Footnotes
Appendix A
Authors’ Note
This article was presented at the American Academy of Otolaryngology-Head and Neck Surgery Foundation Annual Meeting, September 15-18, 2019, New Orleans, LA, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.