
Abstract
Purpose:
The variability of sphenoid pneumatization and its relationship with the surrounding structures has been suggested. The aim of this study was to examine the effect of the surrounding bony structures on the position of the sphenoid ostium (SO).
Methods:
A prospective radiological review of computed tomography images of paranasal sinuses of 150 patients (300 sides) was conducted. Parameters investigated included the presence of Onodi cells, sphenoid rostrum pneumatization, and the type of sphenoid pneumatization on the coronal and sagittal planes. Their effect was studied on the vertical and horizontal plane using lines of measurement 1 through 5.
Results:
The most common location of the SO on the horizontal plane was found to be in the middle third and was significantly affected by the rostrum pneumatization (P value <.001) and sphenoid pneumatization on the coronal plane (P value = .018). The location of the SO on the vertical plane was most commonly in the middle third. It was significantly affected by Onodi cell pneumatization (P value = .021) as well as the sphenoid height (P value <.001).
Conclusions:
Pneumatization of the sphenoid sinus and adjacent bony structures can affect the location of the SO. Presence of rostrum pneumatization and lateral sphenoid pneumatization shift the SO laterally. Presence of Onodi cell and low sphenoid roof shift the SO inferiorly. These variations need to be studied carefully before surgery in order to avoid operative complications.
Introduction
The sphenoid sinus is unique with its wide range of anatomical variations and proximity to some vital neurovascular structures, including internal carotid artery, optic nerve, cavernous sinus, and sella. Such a close anatomical relationship raises particular dangers during the surgery. Therefore, anatomical variations in the sphenoid sinus as well as clear anatomical landmarks are critical for the rhinologist and skull base surgeon to know to safely operate on.1,2
Sphenoid ostium (SO) is one of the principal landmarks when intervening the sinus. Natural ostium is the safest place to enter the sphenoid sinus without injuring adjacent structures.3,4 It has a close proximity to the skull base superiorly, septal branch of sphenopalatine artery inferiorly, and nasal septum medially. A better understanding of the position and characteristics of the SO with respect to the anterior sphenoid face and skull base is crucial. 5
Some authors described the variability of the sphenoid pneumatization and evaluated its relationship with the surrounding structures. 6 Others suggested different references that enable identification of the sphenoid ostia, including the posteroinferior end of the superior turbinate, 3 the distance from the nasal spine, 7 and the location on the anterior aspect of the sphenoid on the vertical axis. 8
Different patterns of pneumatization of the sinus itself and the adjacent structures can affect the location of the sinus ostium.6,9,10 However, the literature lacks reports on the impact of the horizontal pneumatization of sphenoid bone and the rostrum on the location of the ostium. Thus, the aim of this study was to examine the effect of the surrounding bony structures on the position of the natural sinus ostium on the horizontal and vertical plane.
Methods
A prospective radiological review of all computed tomography (CT) images of paranasal sinuses was conducted from January 2017 to February 2018 at King Fahad Medical City (KFMC), Riyadh, Saudi Arabia. Research ethics committee approval was obtained from KFMC institutional review board prior to commencing this project. No patient underwent CT scanning for the purpose of inclusion in this study. High-resolution axial CT images (100 kV, 120 mA, and 0.8 second rotation time) with slice thickness of 0.625 mm, and reconstructed sagittal and coronal images were reviewed by 2 otolaryngology physicians using the Centricity Enterprise Picture Software: Radiology Information Systems (General Electric Company). Separate analysis was done, and inter-rater reliability was calculated.
Patients under the age of 18 years who had nasal, paranasal sinuses, orbital, or skull base trauma/tumors were excluded. Patients who underwent previous endoscopic sinus surgery, anterior skull base surgery, or choanal atresia surgery were also excluded as well as patients with craniomaxillofacial anomalies. Patients with sinonasal polyposis, allergic fungal rhinosinusitis, or other sinonasal diseases hindering view of the SO were excluded as well.
The information gathered from each scan was as follows: Onodi cell pneumatization: defined as the most posterior of the ethmoid cells, which extend superolateral to the sphenoid sinus and is located between the skull base and the sphenoid sinus.11-13 Sphenoid rostrum pneumatization: defined as a triangular spine that is continuous with the sphenoidal crest on the anterior surface and is received in a deep fissure between the alae of the vomer. A distance of 4 mm or more between the alae of the rostrum is considered a pneumatization.
14
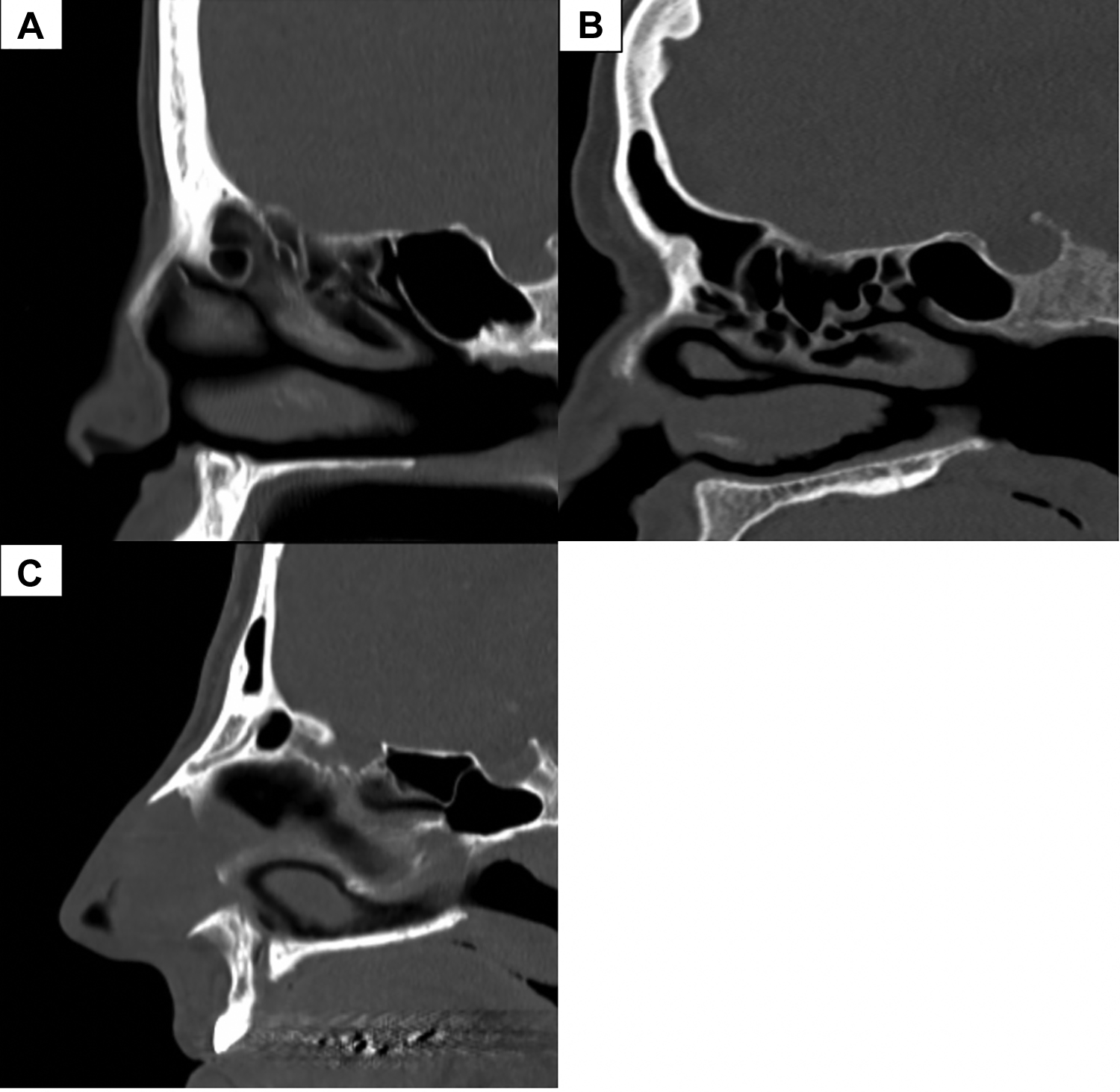
Sphenoid pneumatization on the sagittal plane: classified according to Hammer and Radberg into sellar, post-sellar, pre-sellar, and conchal type
15
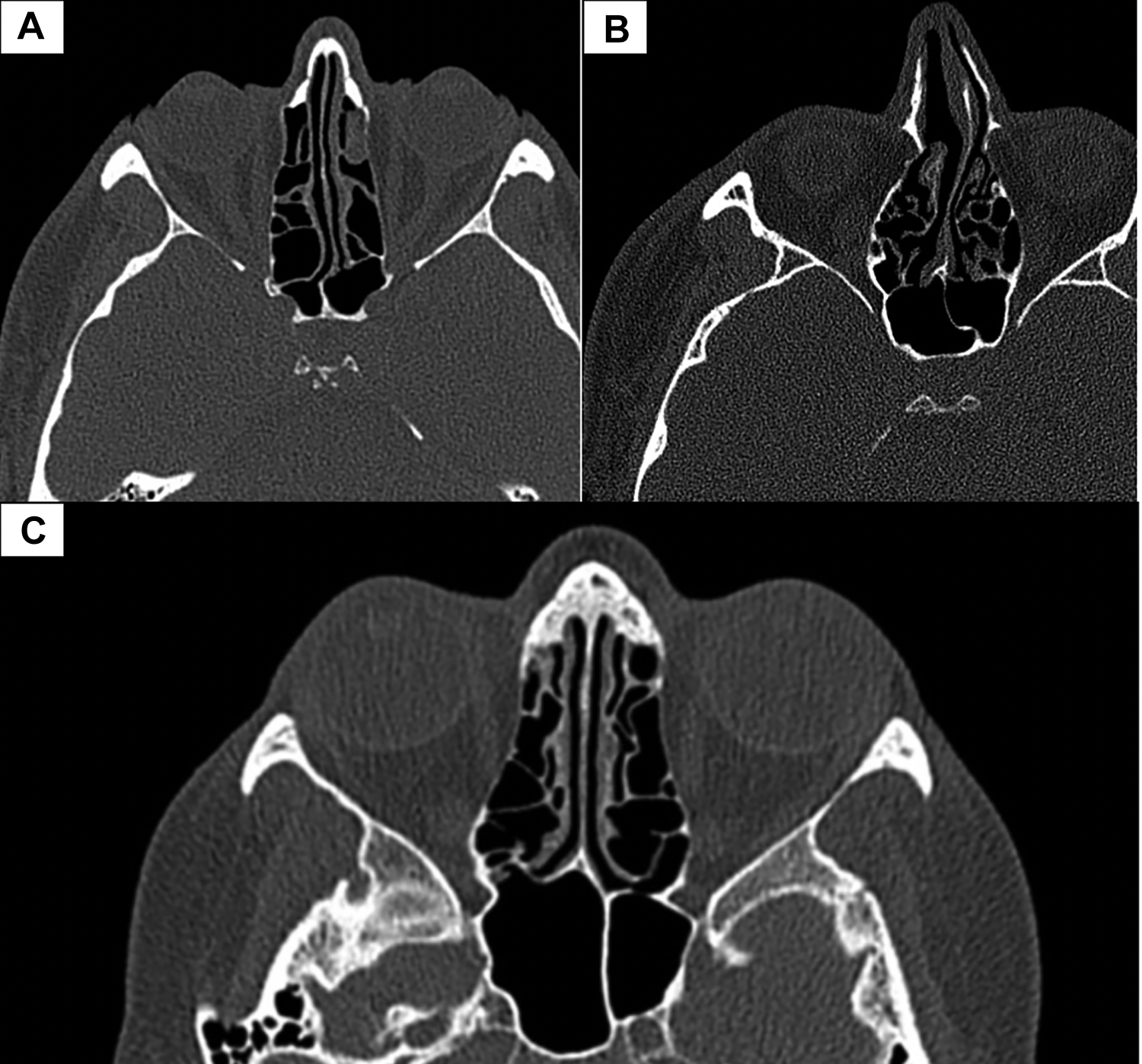
(shown in Figure 1). Sphenoid pneumatization on the coronal plane: classified according to Vaezi et al: type 1 (previdian) pneumatization, type 2 (intercanal) pneumatization, and type 3 (postrotundum) pneumatization
16
(shown in Figure 2).
The sinus pneumatization pattern was classified as conchal, presellar (A), sellar (B), or postsellar (C). There were no sinuses with conchal pneumatization in this study.
Pittsburgh type 1 (previdian), (B) Pittsburgh type 2 (intercanal), (C) Pittsburgh type 3 (postrotundum).
Distance measurements of the ostium in relation to the adjacent structures were taken as follows (displayed in Figure 3):
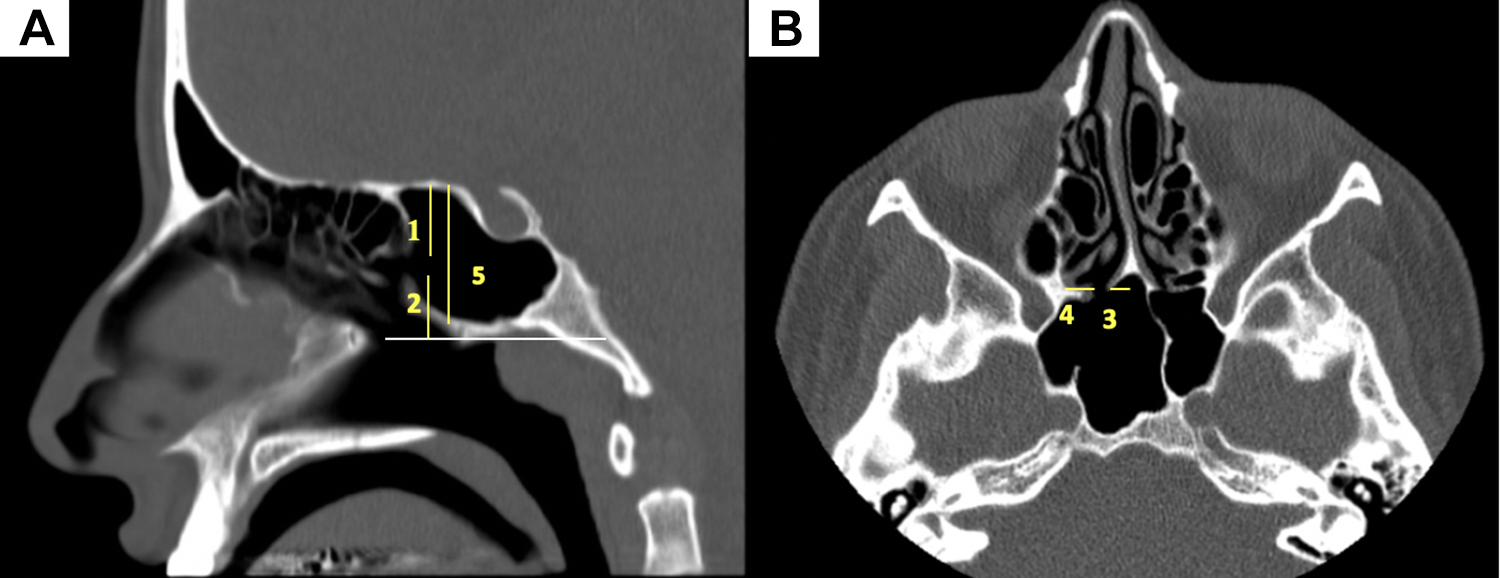
(A) Representation of lines 1, 2, and 5; (B) representation of lines 3 and 4.
Line 1: The vertical distance from the upper border of SO to the skull base.
Line 2: The vertical distance from the lower border of SO to the superior border of posterior choana.
Line 3: The horizontal distance from medial border of the SO to the septum.
Line 4: The horizontal distance from lateral border of the SO to the orbital bone.
Line 5: the vertical distance from sphenoid roof to the sinus base.
Furthermore, the sphenoid sinus ostium location was outlined on the parasagittal plane as upper, middle, or lower based on the vertical height of the sphenoid divided into 3 equal thirds. On the axial plane, the ostium was plotted on the medial, middle, or lateral location based on the distance from the midline to the lateral wall divided into 3 equal thirds.
The main outcome investigated was the effect of sphenoid rostrum and coronal pneumatization of sphenoid bone on line 3, line 4, and the horizontal location of SO. Secondary outcome was the effect of Onodi cell, line 5, and sagittal pneumatization of sphenoid bone on line 1, line 2, and the vertical location of sphenoid bone.
Statistical analysis was performed using SPSS software version 21. Means and standard deviations (SD) were obtained for continuous variables, whereas frequencies and percentages were computed for categorical variables. The t tests were used for continuous variables, and χ2 test was used for categorical variables. Comparison between quantitative variables was done using Pearson correlation and between 2 groups of continuous variables using independent samples t test. Multinominal logistic regression was used to determine the relationship between a set of indpendent variables and a nominal dependent variable which has atleast 3 groups.
Results
The analysis included 150 patients among which 300 sides were evaluated. The studied patients were between 18 and 80 years with a mean age of 39.6 ± 13.7 years. More females were included in the analysis: 97(55%). Two data sheets from 2 independent investigators were analyzed. Inter-rater reliability was calculated by κ statistics and showed substantial agreement (0.76). Measurements of the lines 1 to 5 are displayed in Table 1.
Description of the Parameters Investigated Including lines 1-5, Pneumatization Patterns and the Ostium location on the Vertical and Horizontal Planes.
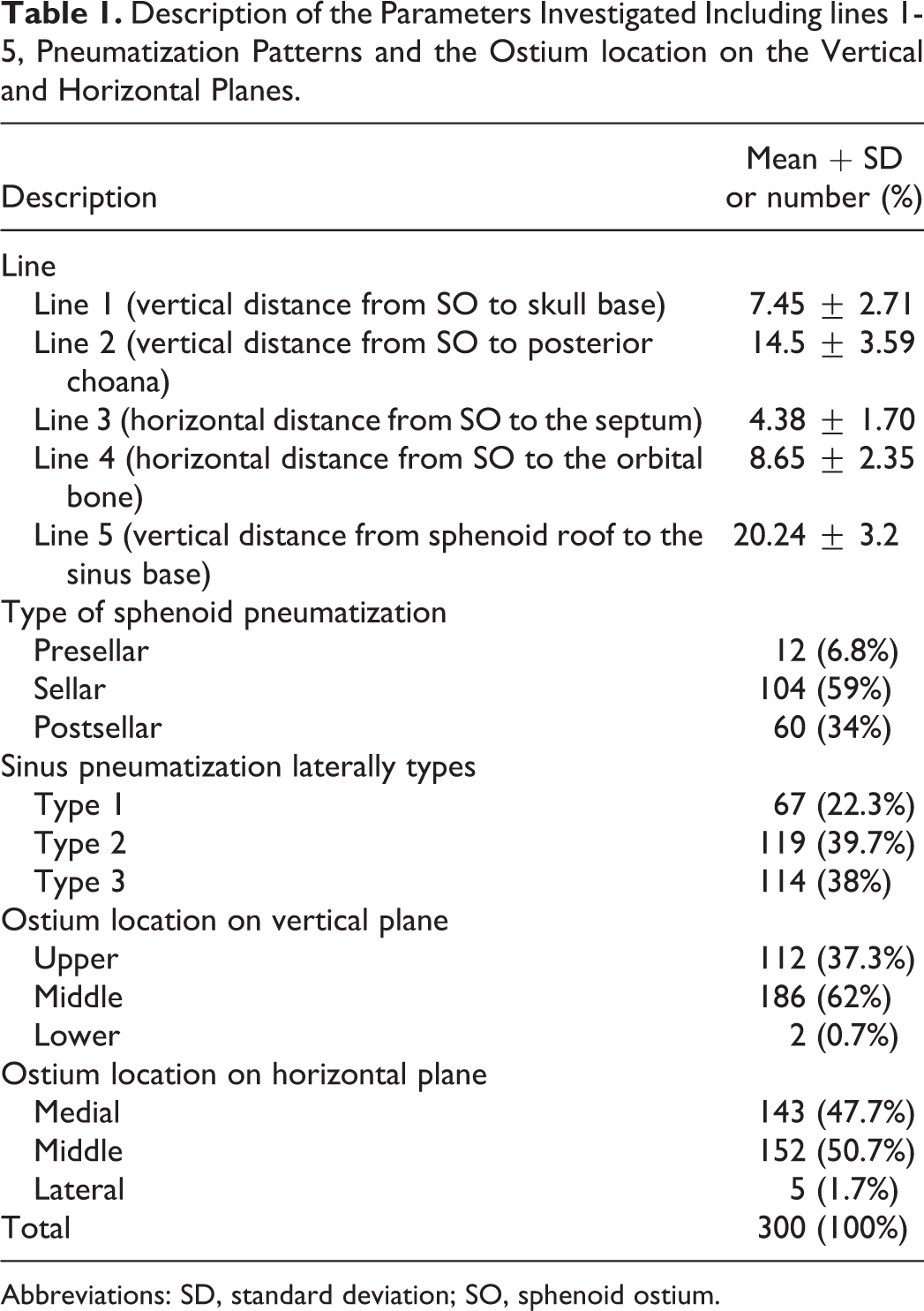
Abbreviations: SD, standard deviation; SO, sphenoid ostium.
Sphenoid Ostium and the Vertical Plane
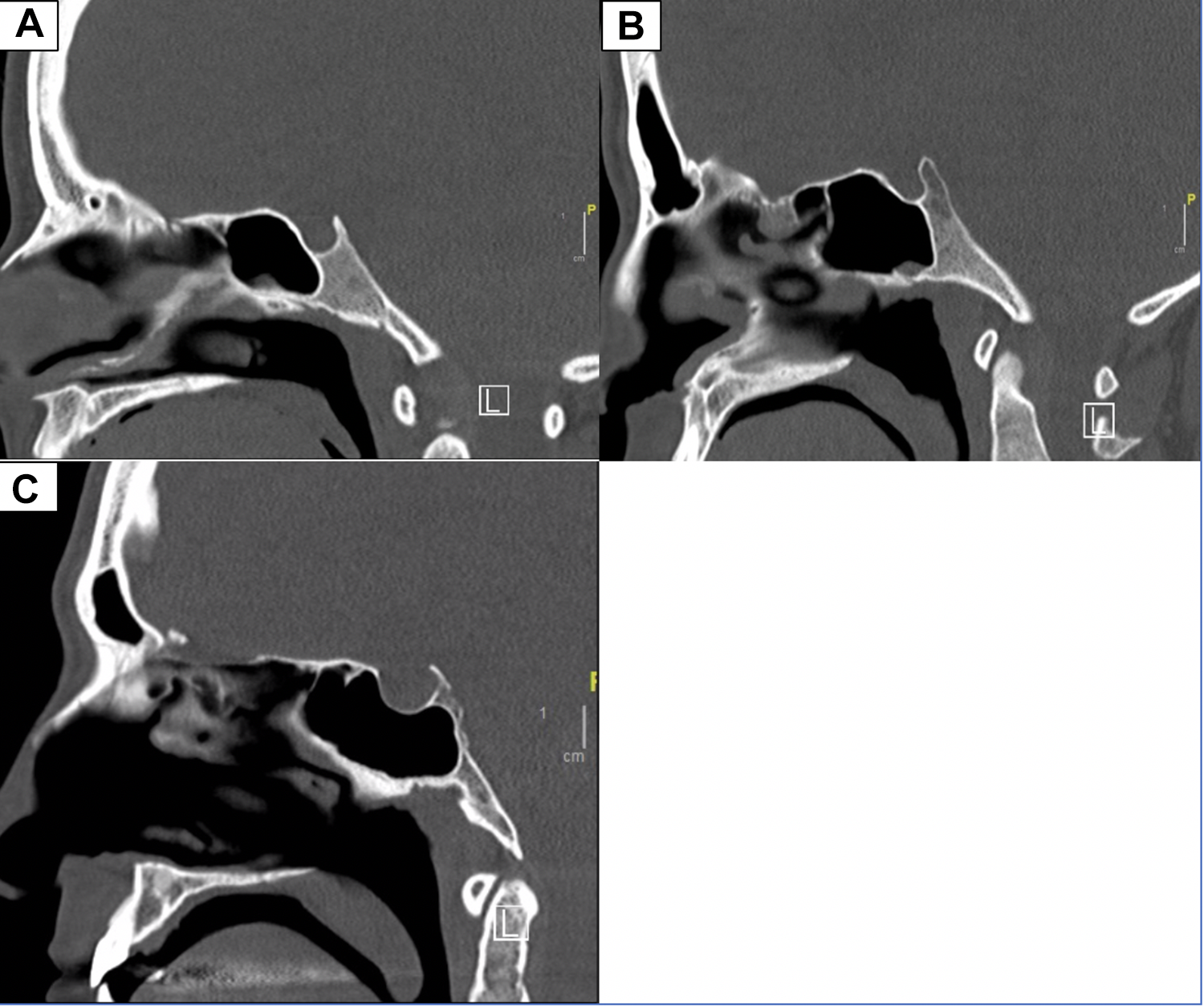
The type of sphenoid pneumatization on the sagittal plane was found to be presellar in 12 (6.8%) sides, sellar in 104 (59%) sides, and postsellar in 60 (34%) sides. The location of the sphenoid sinus ostium on the vertical plane was found to be in the upper third in 112 (37.3%) sides, in the middle third in 186 (62%) sides, and in the lower third in only 2 (0.7%) sides (Figure 4).
Examples of upper ostium location (A), mid-location (B), and lower ostium location (C) on the vertical plane.
Onodi cells were identified in 115 (38.3%) sides. Presence of Onodi cells had a significant effect on the distance from the ostium to the choana (line 2; P = .021), making it in higher location. The sphenoid sinus pneumatization on the sagittal plane had no effect on the vertical position of the ostium; however, the sphenoid height (line 5) showed a statistically significant correlation with lines 1 and 2 (P < .001). The SO is located in a higher position when sphenoid height is shorter. Table 2 demonstrates the affected variables on the vertical plane.
The Variables Affecting the Location of the Ostium on the Vertical Plane.

Sphenoid Ostium and the Horizontal Plane
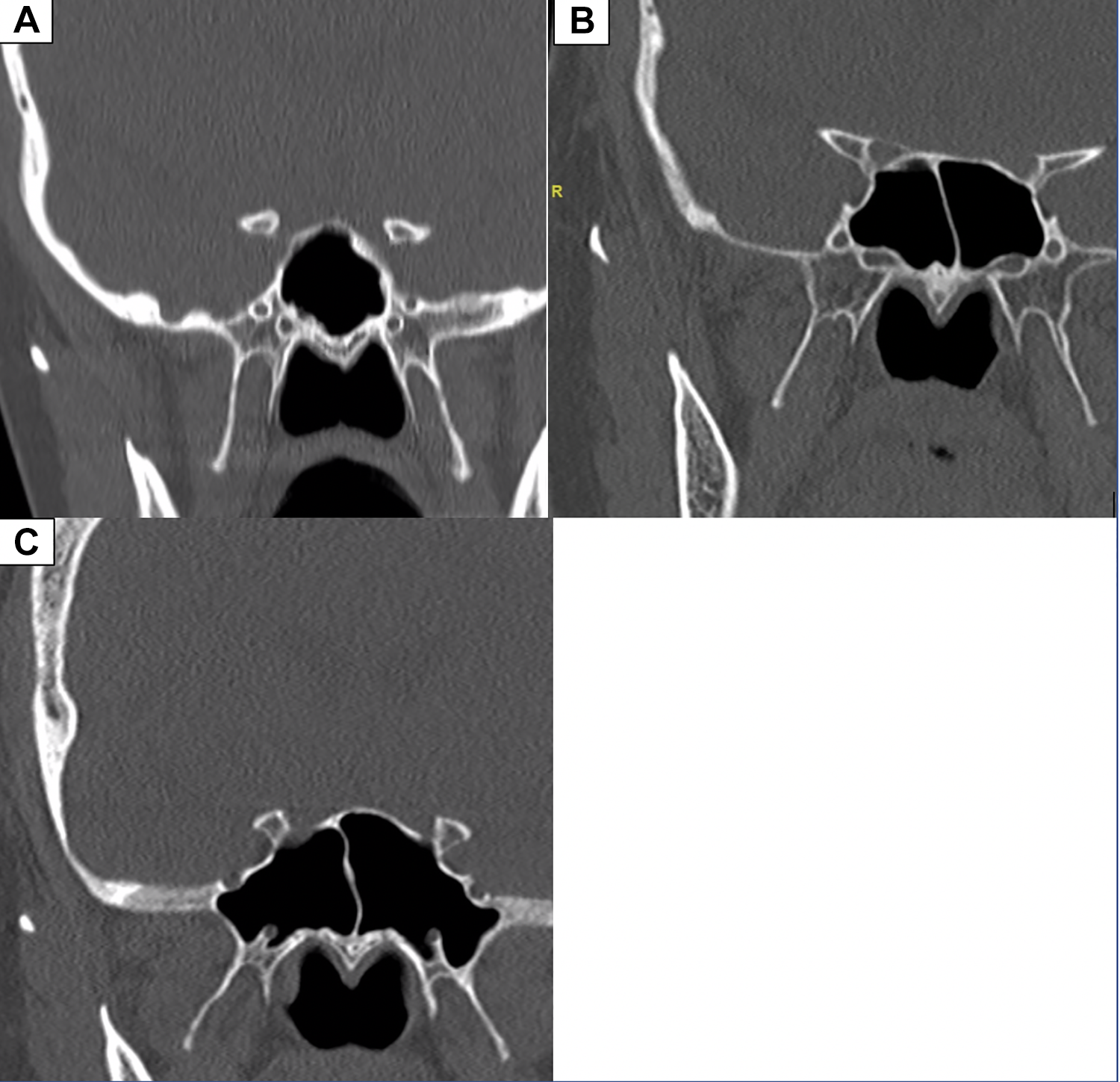
The type of pneumatization on the coronal plane was found to be type 1 (previdian) in 67 (22.3%) sides, type 2 (intercanal) in 119 (39.7%) sides, and type 3 (postrotundum) in 114 (38%) sides. The location of the ostium on the horizontal plane was found to be in the medial third in 143 (47.7%) sides, in the middle third in 152 (50.7%) sides, and in the lateral third in 5 (1.7%) sides (Figure 5). The rostrum was pneumatized 69% of the time with a mean (±SD) width of 5.8 ± 1.6 mm.
Examples of (A) medially located sphenoid ostium (note the lack of pneumatization of the rostrum), (B) mid-location of ostium on the horizontal plane, and (C) laterally located ostium on the left.
Both rostrum pneumatization and sphenoid sinus pneumatization shifted the horizontal ostium location laterally (P < .0001 and P = .018, respectively). Furthermore, nominal regression analysis showed that the horizontal ostium location was significantly affected by both the sphenoid pneumatization on the coronal plane and the rostrum pneumatization (P < .001). The variability, however, was low (Negelkerke R2 = .211). Table 3 demonstrates the affected variables on the horizontal plane.
The Variables Affecting the Location of the Ostium on the Horizontal Plane.
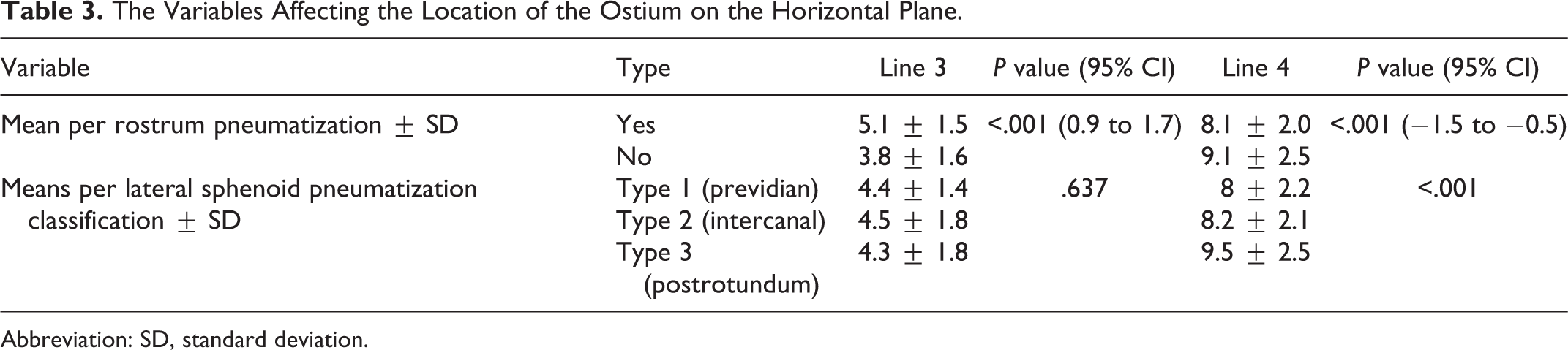
Abbreviation: SD, standard deviation.
Discussion
Sphenoid sinus pneumatization is believed to affect the SO location which is the safest point of entry to the sphenoid sinus. 3 The ostium is an important landmark for entering the sinus for various reasons, mainly for its proximity to many crucial structures, including the optic nerve, internal carotid artery, the sella, and cavernous sinus. 9 If the sinus ostium is missed during surgery, complications may arise such as a cerebrospinal leak superiorly, an arterial bleed inferiorly, or a septal perforation medially.
The effect of the sphenoid rostrum pneumatization on the location of the SO has not been previously investigated. In our analysis, rostrum pneumatization showed a statistically significant association with lateral location of SO. It was found that in a pneumatized rostrum, the SO was most commonly located at the mid-third of the horizontal plane, while in a nonpneumatized rostrum the ostium was most commonly located at the medial third. This finding has an important surgical application when the surgeons try to locate the SO. In cases of rostrum pneumatization, the surgeon should expect the SO to be deflected laterally and behind the superior turbinate but always medial to it. Additionally, our results explain the variations in the reported studies regarding SO location on the horizontal plane, including a cadaveric study conducted by Campero et al, which demonstrated a great variability in the distance from the internal border of the ostia to the midline. They found that in some skulls, the ostia were located far away from the midline, but, in others, both ostia were practically abutting. 17 Many other investigators have found laterally located SO in some specimens and variation in the mean distance of the SO from the midline (line 3).3,4,17-19 These differences may likely be due to the pneumatization of the sphenoid rostrum that has not been considered in their analyses as a causative factor. However, racial and regional variations should be considered as well.
This analysis found that the lateral pneumatization of sphenoid sinus significantly affect the horizontal location of SO as well as line 4. When reviewing the CT scan of the patient, the surgeon should pay attention to the lateral pneumatization of sphenoid sinus, as it may have an impact on the SO and deflect it laterally. As an example, Figure 6 scans are of the same patient and show a lateral ostium with type 3 pneumatization.
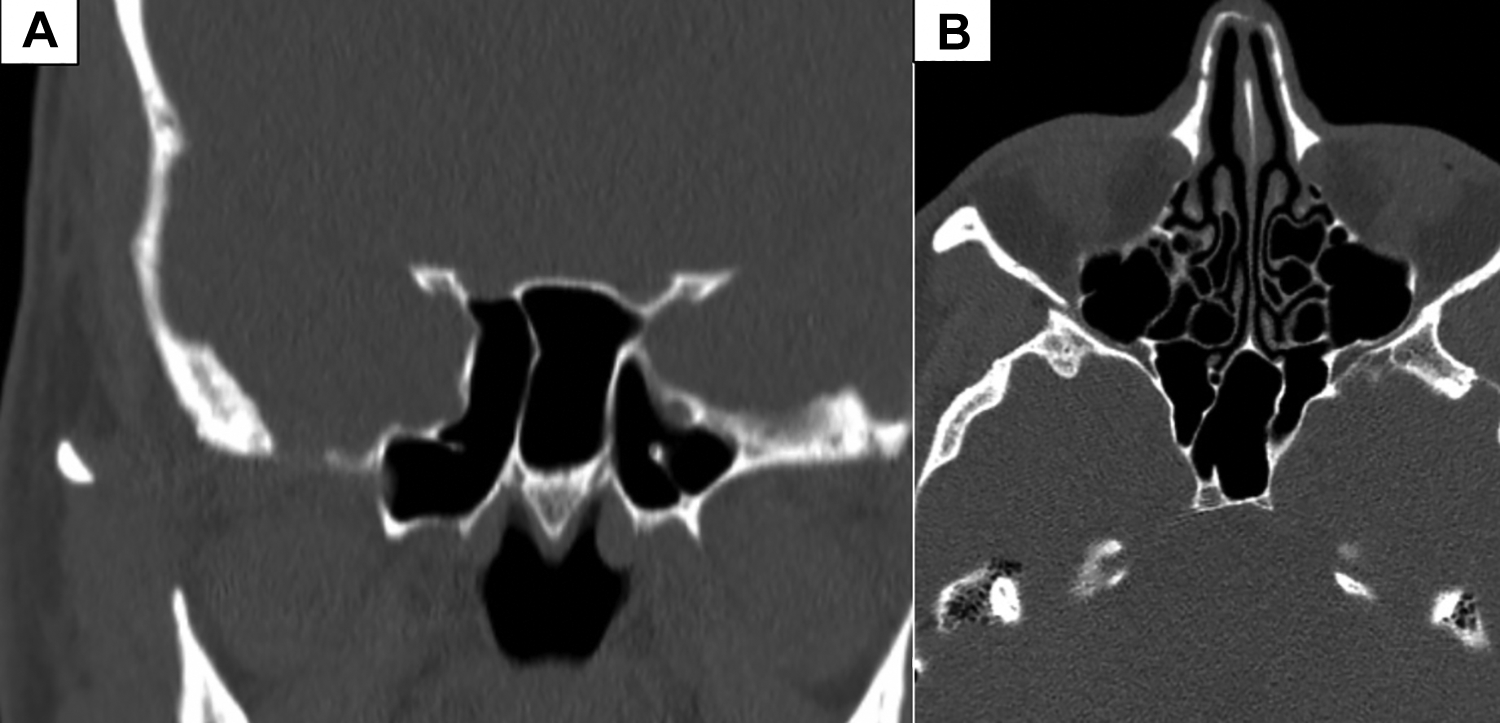
(A) Type 3 pneumatization on the lateral plane with a lateral location of the sphenoid ostium; (B) lateral ostium location in the same patient.
With regard to the vertical location of SO, we analyzed 3 factors that have a potential effect (Onodi cell, sphenoid vertical height [line 5] and sphenoid pneumatization on the sagittal plane). The distance between SO and the choana (line 2) is an important surgical measure in determining the entry point to the sphenoid. This analysis found that presence of Onodi cells lengthens this line, making the ostium in higher location with regard to choana. However, the distance of SO to the skull base was not affected by the presence of Onodi cells. Other authors found the distance from the SO to the roof of sphenoid sinus to be less in the presence of Onodi cells.11,20,21 This suggests that while the roof of the sphenoid may be pushed inferiorly by the Onodi cells, the distance of the ostium to the skull base was not affected.
Interestingly, pneumatization of the sphenoid sinus on the sagittal plane had no effect on the vertical location of the sphenoid sinus ostium nor on lines 1 and 2. These findings are in disagreement with Halawi et al who found that the ostium was closer to the planum in sinuses with sellar (P = .05) or presellar (P = .02) pneumatization when compared to those with postsellar pneumatization. 22 Their results could be related to sphenoid height rather than the type of pneumatization. Conchal type, for example, has the shortest sphenoid height compared to postsellar type, and this might explain their results. Our analysis supported this debate, as we found sphenoidal height (line 5) to be correlated with both lines 1 and 2 indicating that higher sphenoid height results in lower SO location. This is similar to the results obtained by Hidir et al who measured the height between the anterior edge of the choana and the cranial base and found the mean distance to be 21.3 ± 3.2 mm which is close to our calculation of the sphenoid height (20.24 ± 3.2 mm). Similarly, the ostium was found at the inferior one-third of the anterior wall of sphenoid sinus in the most inferior cases and at the superior three-fourth of the anterior wall of sphenoid sinus in the most superior case. 23
This analysis is the first to report the location of SO in both horizontal and vertical planes. We studied this location based on the potential variations of 5 factors (pneumatizations). It provides evidence that SO is deflected in opposite direction to a pneumatized bone. We found that horizontal location of SO is controlled by 2 factors, rostrum pneumatization and lateral extension of sphenoid sinus. This was further confirmed by nominal regression analysis and also found that the rostrum pneumatization combined with the lateral sphenoid pneumatization classifies the location of the ostium on the horizontal plane 67.3% of the time. Furthermore, the vertical location of SO is controlled by 2 factors, the sphenoid height and Onodi cells. When reviewing CT scan, one should be cautious to the pneumatizations of adjacent sphenoid structures that may push the SO to one direction or another.
This study has some limitations, the first being that all scans included here were normal, and therefore the information gathered cannot be generalized to include diseased sinuses. Also, an endoscopic examination could have provided a more clinically oriented insight.
The present data regarding the bony pneumatizations surrounding the sphenoid sinus are of significant importance in endoscopic sinus surgery and need to be thoroughly sought after in every case individually. Identifying the sphenoid sinus ostium is of a particular challenge, since it is closely related to many important structures. Closely studying the CT images for identification of the ostium, the surrounding bony structures and the type of sinus pneumatization could provide precise and useful information about the anatomy of the sphenoid sinus and ostium. Therefore, the measurements described in this study may be very valuable in avoiding serious complications while performing surgery.
Conclusion
On the horizontal plane, the sphenoid rostrum and the lateral extension of sphenoid pneumatization had a significant effect on the horizontal location of the ostium. On the vertical plane, the distance from the choana to the ostium was found to increase in cases where Onodi cells are present. The sphenoid height was also positively correlated with the distance from the SO to skull base and SO to choana, making it a predictor in the preoperative evaluation for endoscopic sinus surgeries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.