
Abstract

A 67-year-old lady presented with 6-month history of progressive, painless submental swelling (Figure 1). Clinical examination revealed a nontender, soft swelling, which was not mobile upon swallowing or tongue protrusion. Transillumination test was positive. The floor of mouth examination was unremarkable, and the mass was not ballotable with bimanual palpation. Computed tomography (CT) of the neck unveiled a well-circumscribed nonenhancing homogenous submental lesion. The presence of a “tail sign” supports the diagnosis of a plunging ranula (Figure 2). She subsequently underwent surgical excision along with the removal of the right sublingual gland (Figure 3). No recurrence was observed 6 months after the operation.
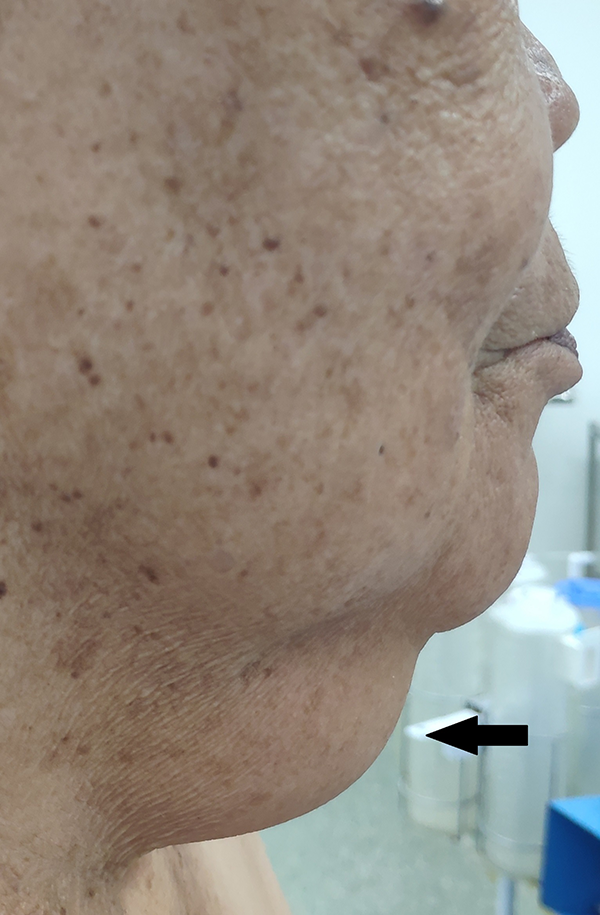
Clinical photography of a swelling over the submental region (arrow).
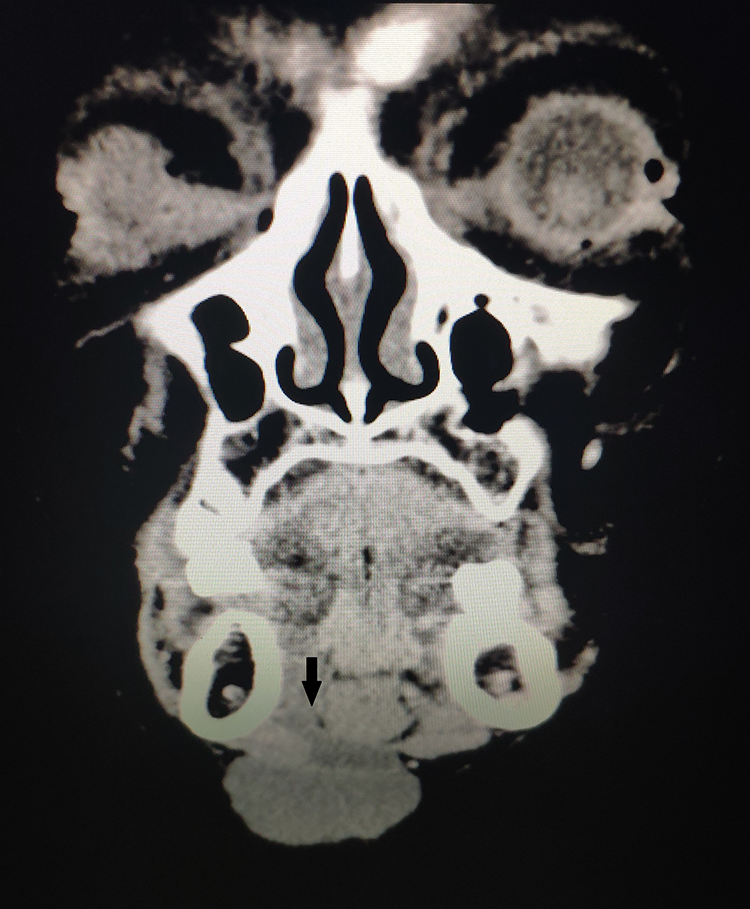
Contrasted computed tomography of the neck in coronal view: presence of “tail sign” (arrow).
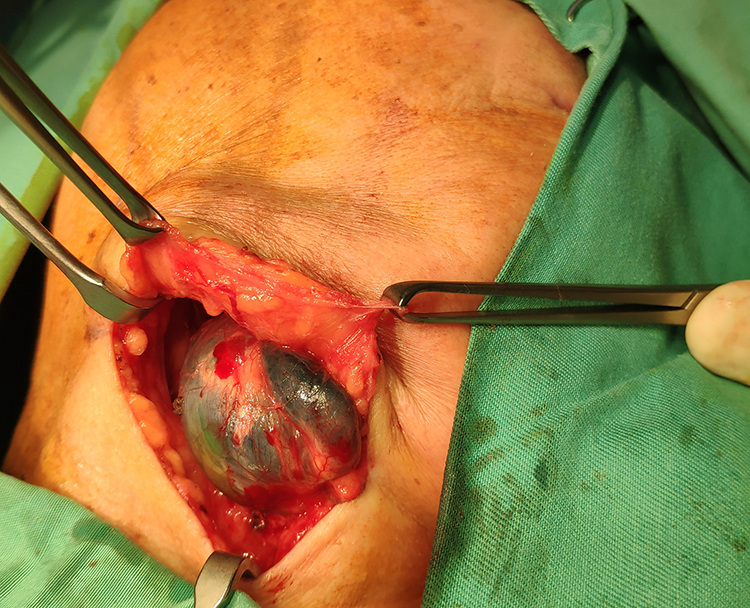
Inoperative finding.
A plunging ranula occurs when a mucous content pseudocyst situated in the floor of mouth herniates through the mylohyoid muscle. Any obstruction along the outflow tract may predispose to traumatic rupture of the excretory salivary duct, thereby resulting in extravasation of saliva and potentially ranula formation. 1 Ranula generally occurs between the second and third decade of life, with a slight male preference ratio of 2:1. 2 The diagnosis can be made clinically, with the aid of CT neck to access the extension. A “tail sign,” which indicates the communication between the collapsed sublingual and submandibular space over the posterior edge of the mylohyoid muscle, is pathognomonic of plunging ranula. 2 Surgical excision is preferred over sclerotherapy with low recurrence rate. 3