
Abstract
Objective:
To investigate the association of high septal deviation with the olfactory fossa depth and Gera angle.
Methods:
Fifty-four computed tomography scans of patients with high septal deviation were evaluated. The olfactory fossa depth and Gera angle were measured. The values of the deviated and nondeviated sides were compared.
Results:
No association between high septal deviation and the olfactory fossa depth and Gera angle was found.
Conclusion:
High septal deviation does not affect the olfactory fossa depth and Gera angle. In other words, the olfactory fossa depth and Gera angle have no association with the high septal deviation.
Introduction
Computed tomography (CT) plays an important role in the assessment of nasal septal deviation (NSD) and paranasal sinus anatomy. Cerebrospinal fluid leak (CSFL) is one of the most common complications of endoscopic sinus surgery (ESS). 1 Some authors suggested that the risk of CSFL is directly proportional to the depth of olfactory fossa (OF).2,3 Some other authors reported that the angle between the lateral lamina (LLCP) and the horizontal plane (HPCP) of the cribriform plate which is called Gera angle creates more risk for CSFL. 4 There were no data in the English literature whether there is an association between the high septal deviation and the depth of OF and the Gera angle. The aim of this study was to investigate the relationship between the depth of OF, angle of Gera, the LLCP, and the high septal deviation.
Material and Method
Paranasal sinus CT scans which were acquired at KENT ENT Center were evaluated retrospectively. Only 54 patients with the diagnosis of high septal deviation were included in this retrospective study. Subjects under 18 years of age (since pneumatization of the paranasal sinuses continues till 18 years of age), previous incidents of sinonasal surgeries, sinonasal trauma, tumor mass lesions of the sinonasal region, and chronic inflammatory mucosal diseases (since they could have changed the anatomic structures) were excluded. All the evaluations were made by the author.
Radiologic Examinations
Computed tomography examinations were performed by using Genoray 3D Cone Beam CT unit (Papaya 3D Plus, Genoray Co). The imaging parameters were voxel size: 75 to 400 µm, tube voltage: 60 to 90 kV, tube current: 4 to 12 mA, line voltage: 220 V, 50/60 Hz, pixel pitch: 100 × 100 µm, focal spot 0.5 mm. Coronal and sagittal 1 mm sections were evaluated.
The septal deviations which reached to the dorsum at the level of the posterior margin of the frontal recess on the coronal and sagittal plane (Figure 1) were accepted as high septal deviation, and the measurements were made at this level. This point is easily identifiable and represents a fixed point for the measurements and that the reliability for measurements taken in this point was high, suggesting a good reproducibility. 4 The direction of the NSD was determined and the angle between the midline and septum was identified as the septal deviation angle (SDA). Patients were categorized into 3 groups according to the SDA grading system of Elahi et al 5 : 1 = mild (<9), 2 = moderate (9-15), and 3 = severe (>15).

The angle between the midline and septum was identified as the septal deviation angle (SDA) at the level of the posterior margin of the frontal recess on the coronal and sagittal plane.
The length of lamina lateralis as the vertical height of the OF and the depth of the cribriform plate were measured in the coronal plane on each side. The depth was defined as type 1 (1-3 mm depth), type 2 (4-7 mm depth), or type 3 (more than 7 mm depth), according to Keros classification system. 6 Degree of the angle formed by the LLCP and continuation of the horizontal plane passing through the cribriform plate was calculated (Figure 1). According to Gera system, 2 the angle was classified depending on its degree as class I (>80°), class II (45° to 80°), or class III (<45°). The depth of OF and Gera angle on the deviated and nondeviated side were compared in this study. The effect of the severity of NSD on the length of lamina lateralis and Gera angle was assessed.
Statistical Analysis
The results of the measurements obtained were analyzed using Mann-Whitney and Fisher tests in order to evaluate the presence of significant differences according to the side of the NSD.
Results
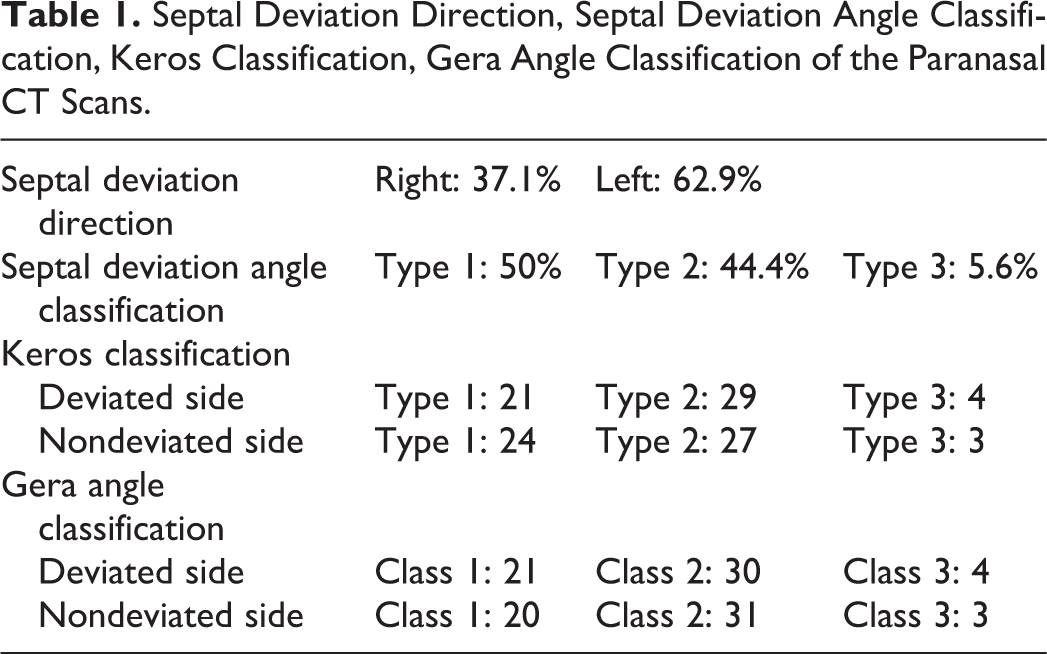
A total of 54 sinus CT scans were retrospectively analyzed. The mean age of the patients was 43.4 ± 4.9 years (range: 25-64). Male to female ratio was 1:2. The nasal septum was highly deviated to the right in 20 patients (37.1%) and to the left in 34 (62.9%) patients. Septal deviation angle classification was 27 type 1 (50.0%), 24 type 2 (44.4%), 3 type 3 (5.6%).
Depth of the Cribriform Plate
On the deviation side, the mean depth of the cribriform was 4.6 ± 1.5 mm (range, 2.5-7.1 mm) and 4.8 ± 1.7 mm (range, 2.7-7.8 mm) at the contralateral side. No significant difference in the depth between the 2 sides was found on Mann-Whitney test (P = .713). The most common anatomic variation at the deviation side was Keros type 2 (29/54 patients), followed by Keros type 1 (21/54 patients) and Keros type 3 (4/54 patients). At the contralateral side, the most common variation was Keros type 2 (27/54 patients), followed by Keros type 1 (24/54 patients) and Keros type 3 (3/54 patients). No significant differences in the distribution of Keros types between the 2 sides were found on Fisher test (P = .514).
Angle
The mean degree of the angle was 67.7° ± 11.4° (range, 28°-82°) in the deviation side and 69.1° ± 11.2° (range, 29°-84°) in the nondeviated side. These differences were not found significant on Mann-Whitney test (P = .756). The most common anatomic variation was angle class II (30/54 patients), followed by angle class I (21/54 patients) and angle class III (3/54 patients) on the deviated side and angle class II (29/54 patients), followed by angle class I (20/54 patients) and angle class III (3/54 patients) on the nondeviated side. No significant differences in the distribution of angle classification between deviated and nondeviated sides were found on Fisher test (P = .815) (Table. 1).
Septal Deviation Direction, Septal Deviation Angle Classification, Keros Classification, Gera Angle Classification of the Paranasal CT Scans.
Discussion
The septal deviation is an important factor in the ESS and especially if there is high septal deviation. High septal deviations may be associated with the abnormalities of anterior skull base anatomy and it may create difficulties during the surgery. Regarding the septal deviation, SDA grading system of Elahi et al 5 was used. Patients were categorized into 3 groups according to this SDA grading system: 1 = mild (<9), 2 = moderate (9-15), and 3 = severe (>15).
One of the most common complications of endoscopic sinus surgery is CSF leak. In the majority of cases, CSF fistula occurs during ethmoidectomy and it can be related to the anatomy of the anterior skull base. Ohnishi and Yanigasawa emphasized the importance of LLCP since it was the thinnest structure of the lateral lamella of the cribriform plate (LLCP) which makes it vulnerable to CSF leak and the commonest site for CSFL. 1 Several authors suggested that OF depth is the most important contributing factor in iatrogenic CSFL, whereas some others think the angle of the LLCP with the horizontal line is more important.2,3 The aim of this study was to analyze the association of the high septal deviation with the OF depth and the angle between the lateral lamella of the cribriform plate and the horizontal plane through the cribriform plate, which were the 2 most important contributing factors in iatrogenic CSF leak. Kainz and Stammberger, Skorek et al, Asal et al, and Sahan et al2,3,6,7 suggested that the risk of iatrogenic CSF leak is directly proportional to the OF depth. In our study, Keros classification system proposed in 1962 by Keros 8 was used. It categorizes the cribriform fossa into 3 types: type 1, 1-3 mm; type 2, 4-7 mm; and type 3, >7 mm. Keros type 3 patients are supposed to have the greatest risk of CSF leak. Gera et al 4 suggested that the angle formed between the lateral lamella and the horizontal plane through the cribriform plate was the most important factor. This classification system proposed by Gera was used in calculating the angle. This angle was classified into 3 classes: class 1 >80°, class 2 >45° to 80°, class 3 <45°, and class 3 with the highest risk of iatrogenic injury. Preti et al 9 reported that Gera classification system together with the Keros classification presented good sensitivity and specificity in predicting a possible LLCP injury during ESS.
High septal deviation may be the result of embryological development or due to trauma at early childhood. Therefore, high septal deviation may be associated with the anterior skull base anatomic abnormalities or it may cause some anatomic changes in the anterior skull base structures. Septal deviation angle was compared with OF depth according to Keros and Gera angle. No difference in the distribution of Keros classes or the depth of OF, Gera angle, and high septal deviation was found. However, this study has some limitations. The number of study group is limited and can be increased. The measurement of septal deviation can be made at other points of the skull base as well, which is not done in this study to have a uniformity. In conclusion, high septal deviation is not associated with the olfactory depth and the Gera angles.
Footnotes
Acknowledgments
The authors are grateful to Dr Taner Ozek, the radiology specialist of KENT ENT Medical Center, for his support and help in the evaluation of CT scans and measurements.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.