
Abstract
Nonepithelial tumors of the larynx are relatively rare neoplasms of the head and neck. The chondrosarcoma, which develops commonly from cricoid and thyroid cartilage, stands for 0.2% of the laryngeal malignant neoplasms. The rhabdomyoma is even more uncommon benign tumor developing from the laryngeal striated muscles. The clinical manifestation and the treatment options depend on the histopathological evaluation, tumor localization, and its size. In presented case, the simultaneous occurrence of benign and malignant tumors of mesenchymal origin in the patient’s larynx was provoking hoarseness, globus sensation, and dysphagia. To the best of authors’ knowledge, no other case of the concomitance of rhabdomyoma and chondrosarcoma of the larynx have been reported in the literature.
Introduction
Neoplasms derived from the mesenchymal tissue are very rare and unusual entities of the head and neck. What is more, a synchronous presence of benign and malignant tumors developed from the laryngeal connective and soft tissues is even more unique.
Adult type rhabdomyoma is a benign neoplasm of the head and neck region originating from the striated muscles of the third and fourth pharyngeal arches. The term was introduced by Zenker in 1864. Multifocal occurrence of this tumor is very rare and has been reported only in a few cases.1,2
Chondrosarcoma is the third most common malignant neoplasm of the larynx which comprises 0.2% of all laryngeal malignancies and was first described in 1816 by Francis Travers. The most common localization is the cricoid and thyroid cartilage, respectively 80% and 17% of the cases. 3
According to the authors’ knowledge, simultaneous development of those 2 rare, nonepithelial tumors of the larynx have not yet been described in the literature.
Case Report
A 61-year-old male presented with a 4-year history of hoarseness, globus sensation in the throat, and dysphagia. The clinical examination of the larynx revealed the presence of a solid mass of the left ventricular fold overlaid by normal mucous membrane (Figure 1). No cervical adenopathy was detected on examination. During phoniatric evaluation, vocal fold paresis was excluded.
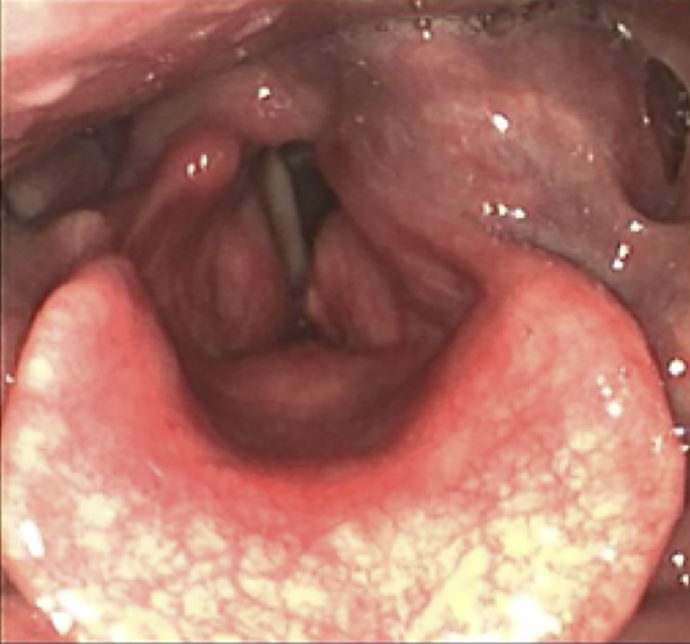
Endoscopic examination of the larynx. Tumor filling left piriform sinus derived from left ventricular fold.
In order to evaluate locoregional advancement of the tumor, preoperative computed tomography (CT) was conducted. The CT scans showed the presence of intralaryngeal mass filling the left piriform sinus which presented with several calcifications and heterogeneous contrast enhancement (Figure 2).
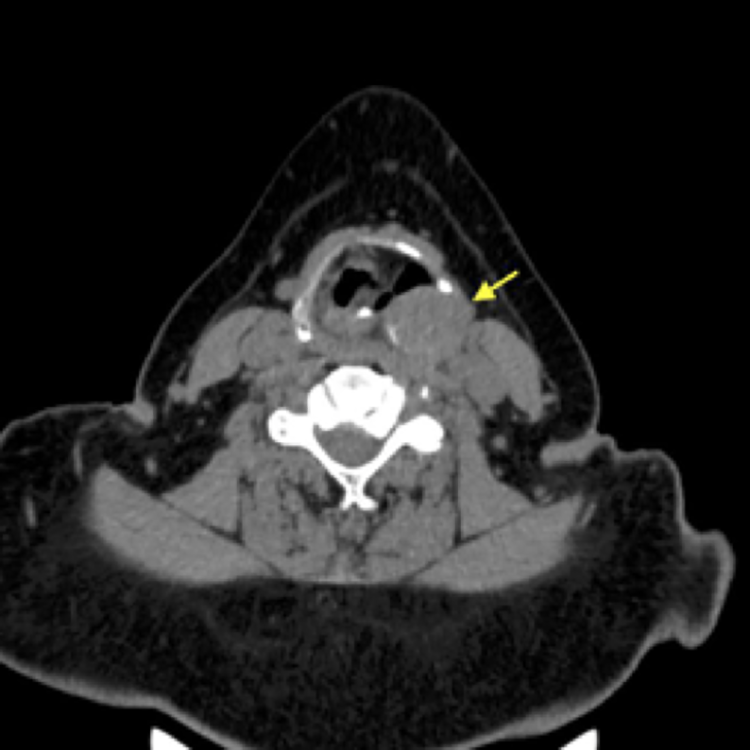
Preoperative computed tomography. Mass of left piriform sinus (yellow arrow). Visible calcifications within tumor.
The tumor as well as a part of the left ventricular fold and Morgani’s sinus were removed with a CO2 laser beam during transoral endoscopic surgery. Postoperative microscopic study confirmed the presence of a malignant neoplasm, G2 chondrosarcoma of the larynx, covered by normal mucous membrane. Due to the presence of neoplastic cells in the surgical margins and the impossibility of a radical removal of the tumor during an endoscopic procedure, the patient was qualified for a total laryngectomy with simultaneous implantation of a voice prosthesis.
During the second surgery, the larynx with the afflicted perilaryngeal tissue and the thyroid gland were removed and submitted for pathological evaluation which revealed the presence of 2 types of neoplasms derived from mesenchymal tissue: G2 chondrosarcoma invading the left piriform sinus and the left ventricular fold, accompanied by multiple adult type rhabdomyoma of the perilaryngeal tissue and the right ventricular and vocal fold (Figure 3) which were discovered coincidentally during specimen examination. Due to the lack of evidence of locoregional invasion of the chondrosarcoma and the radical tumor resection with preserved surgical margins of healthy tissue on pathological examination, the patient was disqualified from adjuvant radiotherapy and remained under supervision in the out-patient clinic.
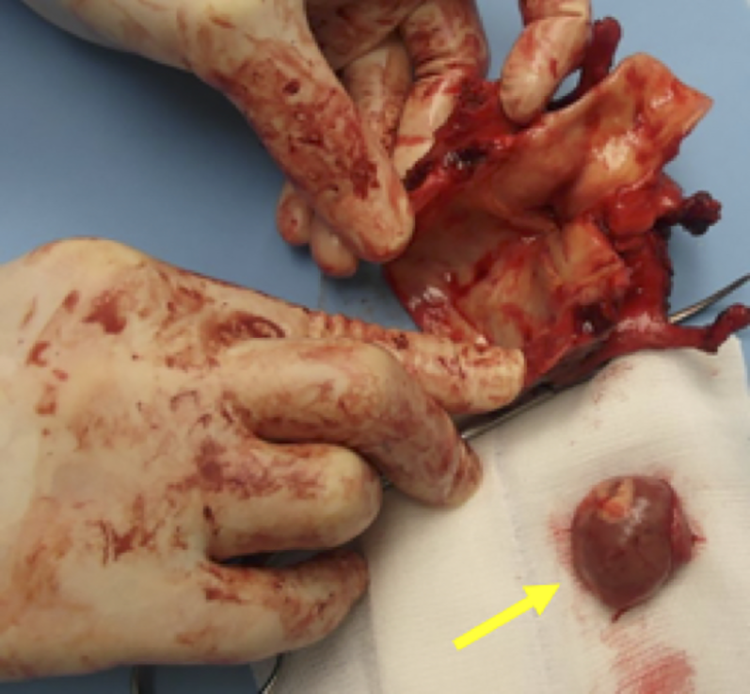
Postoperative specimen. Posterior look on the larynx cut through the cricoid cartilage. On the right, marked with yellow arrow, the tumor extracted from left piriform sinus.
Postoperative hypothyroidism was treated by a specialist in the field of endocrinology. Supplementation of thyroxine was introduced according to the corresponding levels of TSH, FT3, and FT4.
During the next 2 years, monthly follow-up control visits and oncological imaging (postoperative positron emission tomography-CT and magnetic resonance imaging [MRI] of the neck) were scheduled. The radiological and clinical findings show no evidence of recurrence nor local or distant metastases. Therefore, the patient remains under further clinical and radiological follow-up.
Discussion
Rhabdomyoma is a benign, slow-growing tumor that originates from striated muscles, most commonly localizing in the heart. The occurrence of extracardiac rhabdomyoma is most commonly observed in the head and neck region, often developing from the muscle tissue of the upper aerodigestive tract. Laryngeal rhabdomyoma is extremely rare, presenting mostly among male patients in the fourth decade of their lives. 4 The etiology of this neoplasm is not known, but its cervical localization may be associated with abnormalities of the bronchial musculature. 5 The tumors present as reddish-brown or gray, lobular, soft masses in postoperative examination. In microscopic study, sheets of large ovoid or polygonal cells with highly eosinophilic cytoplasm, large, peripherally placed nuclei, and small nucleoli are observed. Cytoplasm may be granular or vacuolated due to the accumulation of glycogen. 6 According to the literature, 3 types of rhabdomyoma can be distinguished: myxoid fetal, cellular fetal, and adult rhabdomyoma. In CT scans, laryngeal rhabdomyoma appears as a submucosally located, well-circumscribed tumor with no invasion of the surrounding tissues. It might mimic a malignant lesion if the mass blends into the adjacent isodence muscle, and the borders of the tumor may be hard to distinguish. The lumps should be differentiated with cysts, laryngocele, or other benign and malignant neoplasms. 4 Due to its benign character, the main method of treatment is a complete surgical excision with preservation of surrounding tissues. Nevertheless, recurrences leading to the obstruction of upper aerodigestive tract may occur even after many years and are associated with partial excision of the primary tumor mass.
Chondrosarcoma is a malignant but relatively low-grade neoplasm that comprises about 1% of laryngeal tumors and 0.1% of head and neck neoplasms. It occurs most frequently among patients between the ages of 50 and 80 years. 7 Clinical signs depend on the location and size of the tumor, thus the symptoms can be easily confused with chronic laryngitis or asthma. Due to an occasional appearance of metastases and regional lymph node involvement, treatment is based on surgical resection of the tumor during a function-preserving surgery, but no consensus has yet been reached regarding the optimal treatment. Total laryngectomy may be elected in cases of extended laryngeal cartilage destruction and large or recurrent tumors. Therefore, exact tumor localization and the possibility of preserving the postoperative function of the larynx, its size, and histological grading should always be considered in the decision-making process. Recurrence may happen in 16% to 18% of the cases and is usually associated with incomplete removal of the tumor during primary excision.3,8,9 Laryngeal chondrosarcoma may appear as a lobular, hypodense, submucosal mass developing from hyaline cartilage in CT scans. Magnetic resonance imaging examination reveals isointense masses corresponding with muscle in T1 and hypointense masses in T2. It may not be possible to distinguish between low-grade chondrosarcoma and chondroma based on CT or MRI results due to their resemblance. 10 Therefore, the final diagnosis always depends on direct laryngoscopy with deep, submucosal biopsy and postoperative microscopic study. In the majority of the cases, no distant metastases or regional lymph node involvement is observed which provides a rather good prognosis for the patient.
The role of radiotherapy among patients with laryngeal chondrosarcoma is limited due to the low radiosensitivity of the tumor cells. Adjuvant chemotherapy is not widely used because of the low risk of metastasis and lymphatic involvement. However, patients should remain under long-term postoperative observation.
Conclusion
Nonepithelial, mesenchymal-derived tumors are relatively rare neoplasms of the head and neck region and the upper aerodigestive tract. Treatment is based on tumor removal during a function-preserving surgery, preceded by biopsy with microscopic evaluation and imaging study. In some cases, radical approach of a total laryngectomy may be proposed. No adjuvant treatment is recommended among patients without evidence of lymph node involvement or presence of distant metastases. However, long-term follow-up should be scheduled for those patients. According to the authors’ knowledge, no previous case of a simultaneous occurrence of laryngeal chondrosarcoma and rhabdomyoma has been reported in literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.