
Abstract
Background:
Chronic rhinosinusitis (CRS) is one of the most commonly reported chronic diseases. Refractory CRS represents a subgroup of patients who continue to be symptomatic even after adequate medical and surgical therapy. These patients started to form a significant portion of patients with CRS. Food elimination as a therapeutic method to control symptoms of different chronic diseases, such as eosinophilic esophagitis, asthma, and atopic dermatitis, has been described in the literature with variable success rates.
Objectives:
To evaluate the effectiveness of food elimination therapy as adjuvant treatment in refractory patients having CRS with positive food sensitization.
Design:
Prospective open-label study.
Setting:
Tertiary academic center.
Methods:
Consecutive adult patients with refractory nonobstructive CRS (patients who had persistent sinonasal symptoms despite endoscopic sinus surgery and patent sinuses ostia with adequate medical treatment) with positive food sensitization were included. Subjects were asked to eliminate the sensitized food from their diet. Clinical outcome was assessed using the Lund-Kennedy symptom and Lund-Kennedy endoscopic appearance scores.
Results:
Twenty-two patients were initially enrolled in the study. Six patients were excluded; 4 were lost to follow-up, and 2 did not eliminate the causal food for the required period. The average age of the patients was 36 years old. There were 10 female and 6 male patients. Nasal discharge and facial pressure were the most common presenting symptoms. Shellfish, egg, and meat mix were the most common eliminated foods. There was a significant difference in the patients’ Lund-Kennedy symptom and Lund-Kennedy endoscopic appearance scores at 6 and 12 weeks after food elimination therapy.
Conclusions:
Food elimination in refractory CRS is an effective adjuvant treatment and should be considered in the treatment algorithm of patients with persistent symptoms after successfully performed sinus surgery.
Introduction
Chronic rhinosinusitis (CRS) is a heterogeneous broad-spectrum disorder of different disease pathologies resulting in chronic inflammation of the paranasal sinuses. It is one of the most commonly reported chronic diseases affecting approximately 13% of the world population.1,2 The disease has been proven to have a more impact on the quality of life than chronic pulmonary and cardiac illnesses. 2
Functional Endoscopic Sinus Surgery (FESS) is considered the gold standard treatment for medically resistant CRS. 3 The operation is safe, minimally invasive, and effective; however, a subgroup of patients continue to be symptomatic even after adequate surgical therapy which is commonly referred as refractory CRS. 4 These patients started to form a significant portion of daily clinical practice at tertiary referral centers.
Persistent sinonasal symptoms after FESS can be due to obstructive and nonobstructive factors. Postoperative adhesion, middle turbinate lateralization, scar tissue, and persistent infected cell are common obstructive failure factors requiring revision surgery. The nonobstructive group has the same persistent nasal complaints, but they do not have any evidence of obstruction on endoscopic or radiological examination which limits the role of surgical management option. Biofilm formation, immunodeficiency, inhalational allergy, ciliary dysfunction, and neosteogenesis are factors that have commonly been cited as predisposing etiology in the nonobstructive refractory CRS. 4
The prevalence of food allergy in the general population of the United States is estimated to be from 1% to 3% in adults and 3% to 8% in infants. 5
Many authors found a correlation between food allergy and CRS. Pang et al 6 found 81% of patients with nasal polyps had positive intradermal food allergy test, while only 11% showed allergic reactions. Similarly, Dogru et al 7 and Collins et al 8 reported a high prevalence of food allergy among patients with nasal polyps (74% and 70%, respectively), which was significantly higher than the reported prevalence in healthy control groups.
An elimination diet as a therapeutic method to control symptoms of different chronic diseases such as eosinophilic esophagitis, asthma, and atopic dermatitis has been described in the literature with variable success rates.5,9-11 The aim of this pilot study is to evaluate the efficacy of food elimination therapy as adjuvant treatment in patients with nonobstructive refractory CRS having positive food allergen sensitization.
Patients and Methods
After obtaining institutional review board approval, the consecutive adult patients with refractory CRS who had positive food sensitization were included in this study. All patients underwent 1 or more endoscopic sinus surgery, signs and symptoms of persistent CRS with endoscopic and computed tomography (CT) evidence of patent sinus ostia, and failed to improve after being treated with broad-spectrum antibiotics, corticosteroid, and nasal irrigation.
All patients had a suggestive history of food allergy; the majority had runny nose and/or pruritis after certain food ingestion. Food sensitization has been tested by serum concentration of allergen-specific immunoglobulin E (IgE) to 34 food types measured by the Enzyme Allergo-Sorbent Test (Euroimmune kits; Medizinische Labordiagnostika). Patients who were allergic to more than 3 diets or had a test score of less than 2 were excluded.
All patients were informed to eliminate the positive tested food from their diet for 6 weeks and to continue on nasal irrigation and nasal steroid spray. Clinical response to treatment was monitored using the Lund-Kennedy (LK) symptoms score and the LK endoscopic appearance score. 12 This was done before initiation of food elimination therapy and at 2, 6, and 12 weeks after elimination.
The LK symptoms score evaluates nasal congestion and obstruction, headache, facial pain, alteration in the sense of smell, nasal discharge, and sneezing by grading each symptom on a scale of 0 (absent) to 10 (most severe) with a total score range from 0 to 60. The LK endoscopic appearance score evaluates 5 specific findings in the postoperative created ethmoid cavities: polyp, discharge, edema, scarring/adhesions, and crusting. Each element is scored from 0 to 2 for each side. Statistical analysis was performed using Student t test. A P value of less than .05 was considered significant.
Results
Twenty-two patients with nonobstructive refractory CRS were initially enrolled in the study. Four patients were lost to follow-up. Two patients did not eliminate the causal diet for the required period and were excluded. The mean age of the remaining 16 patients was 36 years (range; 16-63 years) with 10 female and 6 male patients. Three patients had nasal polyposis, 2 had asthma, and 1 had Samter’s triad.
Nasal discharge was the most common presenting symptom in 9 (56%) patients followed by facial pressure and/or headache in 5 (31%) patients. The average time between surgery and enrollment in the study was 13.2 months (SD ±7). The average number of eliminated diets per patient was 1.8 (SD ± 0.75). Shellfish, egg, and meat mix were the most common eliminated diets.
There was a progressive improvement in the LK symptom and LK endoscopic appearance scores throughout the follow-up time, which reached a statistically significant level after 6 weeks of diet elimination (P = .008 and P = .04, respectively) and maintained for 12 weeks (P = .002 and P = .008, respectively; Figure 1). Interestingly, 5 patients were found to have completely healthy ethmoid cavities with 0 LK endoscopic appearance score at the last follow-up time. When we assessed each component of the LK symptom score separately, we found an improvement in each domain value; however, the difference did not reach a significant level (Figure 2).
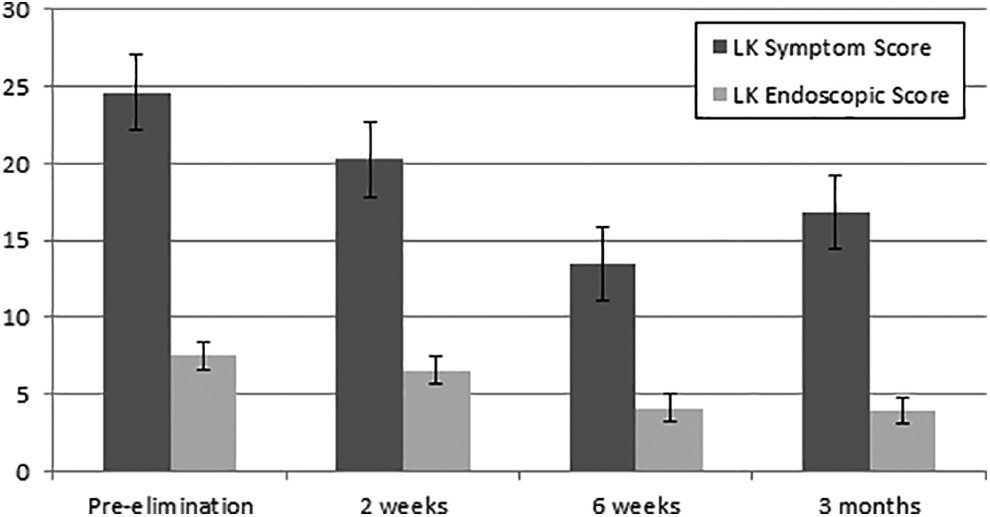
Bar chart illustrates changes in Lund-Kennedy symptom and endoscopic appearance scores at various study periods.
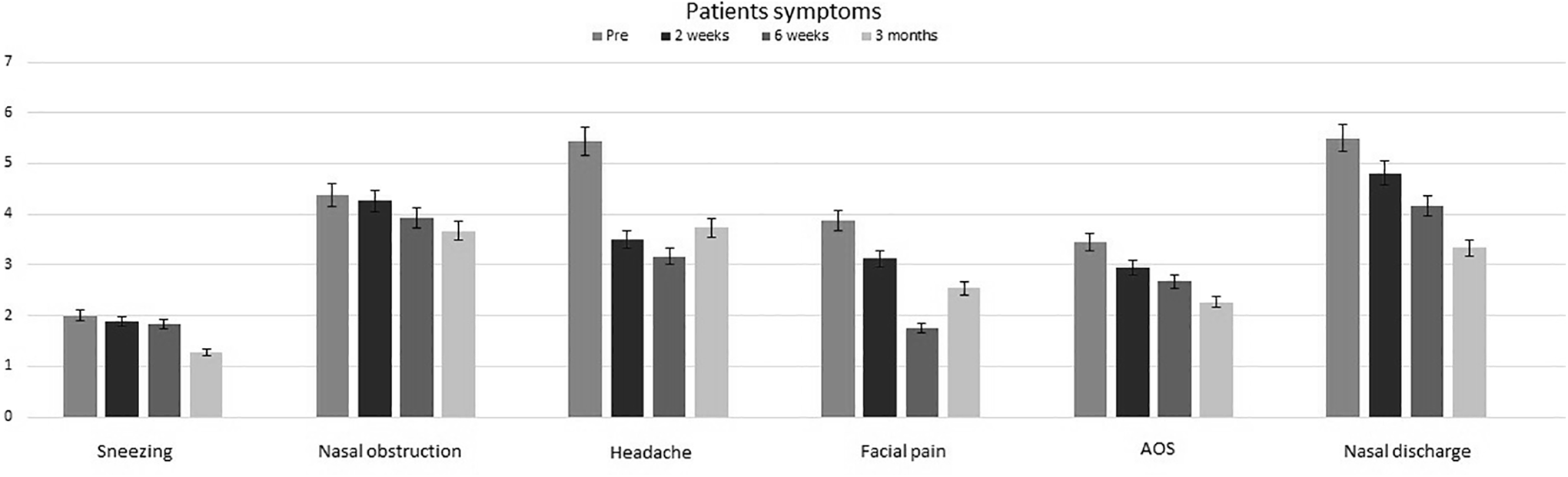
Bar chart displays the changes in individual Lund-Kennedy symptom score at various study periods.
Discussion
We found in this prospective pilot study that food elimination in positively sensitized patients can improve sinonasal symptoms and endoscopic signs in patients who continue to be symptomatic even after properly performed endoscopic sinus surgery. Patients with food-induced allergic disorders can present with different symptoms involving the respiratory tract, skin, gastrointestinal tract, and cardiovascular system. Immunoglobulin E-mediated food-induced allergic reactions are most often responsible for skin and respiratory tract symptoms, whereas isolated gastrointestinal disorders are often caused by non-IgE-mediated reactions. When approaching patients with possible food-induced allergic disorders, it is useful to be divided into IgE- and non-IgE-mediated syndromes. Although initial clinical evaluation is fundamentally identical for both disorders, the consequent assessment differs substantially. Proper diagnosis often requires screening tests for evidence of food-specific IgE and proof of reactivity through elimination diets and oral food challenges. Once accurately diagnosed, strict avoidance of the implicated diets is the only proven form of treatment. 13
Clinical history, physical examination, and diagnostic tests are required to diagnose food allergy. In some cases, an oral food challenge may also be required. 14 History should determine the possible causal foods, amount ingested, time and course of reaction, and any specific risk factors such as atopic dermatitis and a family history of atopy. 15 Allergen-specific serum IgE (sIgE) test and skin prick test (SPT) are sensitive to detect food sensitization but with limited specificity for predicting clinical allergy. Both tests are associated with a high rate of false positives due to cross-reactivity between homologous protein. 15
The SPT is a rapid, safe, and sensitive method for diagnosing suspected IgE-mediated food allergy. A positive SPT has a sensitivity of approximately 90%; however, its specificity is only around 50% which is not enough for food allergy diagnosis unless the patient has a suggestive history. 16 The negative predictive value (NPV) of SPT is greater than 95%, so a negative SPT generally confirms the absence of IgE-mediated reactions.14,17
A radioallergosorbent test and similar in vitro tests that measure quantitative food-specific IgE antibodies have been shown to be more predictive of symptomatic IgE-mediated food allergy. There is a direct relationship between the food-specific IgE level and the probability that an individual will react to that ingested food. 18
Immunoglobulin E is quantified using kilo units per liter based on the World Health Organization Reference Standard with 1 unit equaling 2.42 ng of IgE. 16 Using the cutoff of 0.35 kU/L, sIgE testing has high sensitivity but poor specificity to diagnose food allergy. For example, in peanut allergy cases, sIgE to peanut has a sensitivity of 75% to 100% and a specificity of 17% to 63%. Adopting 95% positive predictive value (PPV) cutoffs, the specificity of IgE testing increases, and by using the cutoff of 15 kU/L for peanut allergy, the specificity and sensitivity were 96.8% and 28.4%, respectively. 19 The 95% PPV cutoffs can be useful to confirm the diagnosis of food allergy, especially if there is a recent history of allergic reaction. On the contrary, the cutoff of 0.35 kU/L can be useful to exclude the diagnosis of food allergy as it has a high NPV. Levels of sIgE between positive and negative cutoffs without a clear clinical history do not confirm or exclude the diagnosis. 20
The oral food challenge is considered the gold standard for the diagnosis of food allergy with PPV and NPV accuracies exceeding 95%. However, this diagnostic method is infrequently used because it is impractical in the busy practice setting. It requires several hours to conduct and also properly equipped centers with specialized staff, as it carries the risk of inducing a severe anaphylactic reaction. 18
The prevalence of food allergy in the general population has been estimated to be around 4%, whereas studies from different parts of the world found it to be much higher in patients with CRS which might reflect a role of food allergy in pathogenesis of sinusitis.8,21,22 A correlation has been found between sinusitis with nasal polyposis and food allergy in case–control studies. Lill et al 21 found a significant high prevalence of milk allergy in CRS with nasal polyposis. Interestingly, patients undergoing surgery for nasal polyposis were more likely to have positive food sensitization compared to healthy controls. A more recent study confirmed the high prevalence of food allergy in refractory CRS but failed to find a significant difference in the sensitization profile based on the presence of nasal polyposis. 22 Contreras et al 23 conducted a literature review to determine whether atopy has a role in CRS. They suggested a possible role of food allergy in CRS pathophysiology although none of the 1755 reviewed articles had evaluated whether exposure to the positively tested foods showed worsening of symptoms, CT scan scores, postsurgical outcome, or whether eliminated diets led to resolution of inflammation.
Increased upper respiratory tract mucus production after excessive dairy milk consumption is known as the milk mucus effect. 24 Frosh and coworkers prospectively examined the effects of dairy versus nondairy diets on self-reported levels of nasopharyngeal mucus secretion. The study included only subjective measures of levels of nasopharyngeal secretions. They concluded that adults with nasopharyngeal hypersecretion might have a significant reduction in mucous secretion after a dairy diet elimination. The study was conducted over 8 days period with no long-term follow-up to support the diagnosis. Additionally, patients with allergy to milk and soya were excluded. 25
The possibility that dairy diet affects the viscosity or thickness of mucus is not clear. Perception of thick mucus after milk consumption could be explained by the fact that mixing saliva with emulsion such as milk can lead to droplet flocculation which affects the mouth feel and other sensory aspects that lead to mucus sensation. 26 Some investigators found no clear change in airway resistance to alter airflow parameters, they did suggest that milk lipids can alter gas exchange in patients with asthma. 27 However, others found no definitive link between milk consumption and the prevalence of asthma-related symptoms.28,29
Sugar allergy is a common but difficult to diagnose because of its presence in most foods. It is IgE-mediated allergy that leads to increased histamine levels in the body. Nasal symptoms are common in sugar allergy. The release of histamine causes inflammation of the sinuses that leads to excessive mucus production, headache, sneezing, congestion, and a runny nose.30,31
The role of food elimination in disease pathology control has been studied thoroughly in eosinophilic esophagitis. Eosinophilic esophagitis is a rapidly rising allergic disease induced by immune response dysfunction to food antigens. Its pathogenesis is complex, involving both IgE-mediated and cell-mediated allergic mechanisms. While IgE is not directly involved in the trafficking of eosinophils to the esophagus, IgE- and cell-mediated allergy play a role in the pathogenesis and presentation features. The disease is characterized by recurrent or chronic symptoms of esophageal dysfunction and eosinophilic inflammation confined to the esophagus that is refractory to high dose of acid suppressants. The majority of patients are atopic with coexistence of atopic dermatitis, allergic rhinitis, and/or asthma. The diagnosis is based on SPT or measurement of serum antigen-specific IgE. Foods elimination therapy has proven to be effective and became the mainstay of treatment in eosinophilic esophagitis. 9
Bath-Hextall et al 5 conducted a systematic review of randomized controlled trials to assess the effects of dietary exclusions in the treatment of established atopic eczema. Nine trials of 421 participants were included, most of which were poorly reported. They found a little good-quality evidence to support the use of exclusion diets in atopic eczema and recommended conducting better methodology designed studies to evaluate the benefits and harms of dietary exclusion in patients with atopic eczema.
Food allergies can precede the development of asthma and are considered a risk factor for exacerbations, use of systemic steroids, increased rates of hospitalization, and life-threatening asthma in young children. 10 Priftis et al 11 conducted a cross-control study to test the hypothesis that children allergic to common food allergens in infancy are at increased risk of wheezing illness and bronchial hyperresponsiveness during school age. They found that sensitization to food was a marker for increased risk of later asthma, but the presence of asthma symptoms and bronchial hyperreactivity were not associated with persistence of the food sensitization. Interestingly, there was no association between the severity of allergic reaction to foods and risk of developing asthma.
Although numerous scoring systems have been proposed to replace the LK scoring system, it remains one of the most frequently utilized and referenced in rhinology outcomes research, because of its simplicity, ease to remember, reproducibility, and intended design to describe endoscopic findings in patients who have already undergone endoscopic sinus surgery. Studies found significant correlations between numerical improvements in these scores and improvements in patient-reported health-related quality-of-life measures, namely, the Chronic Sinusitis Survey and Rhinosinusitis Disability Index.4,32
The limitations of this study are the relatively small number of patients, the absence of control group, and the short follow-up time. However, this work is the first in the literature reporting a possible role of food allergy in persistent symptoms of refractory nonobstructive CRS and showing that food elimination could be beneficial in these cases.
Conclusion
Patients with nonobstructive refractory CRS who tested positive for food allergy may benefit from food elimination, and the improvement in sinonasal symptoms and endoscopic signs can be maintained for a short period of time after the diet elimination. In patients with chronic inflammatory disorders of the upper aerodigestive tract, food allergy should be considered. Further case–control studies with large number of patients, better design and long clinical follow-up time are needed to fully evaluate the association between the 2 conditions.
Footnotes
Authors’ Note
This research was approved by our university IRB committee. Initial result of this study was presented as a poster at the 3 rd Congress of European ORL-HNS, Prague, June 7-11, 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from deanship of research, Jordan University of Science & Technology, Irbid Jordan.