
Abstract
Objective:
To determine the surgical outcomes of free tissue transfer surgery following head and neck tumor extirpation in a low-volume medical center.
Methods:
Retrospective chart review of patients who underwent free tissue transfer surgery for head and neck cancer at Moanalua Medical Center from 2015 to 2018.
Main Outcome of Measure:
Free flap failure rate and free flap-related complications.
Results:
From 2015 to 2018, there were 27 free tissue transfer surgery (mean 6.75 flap surgery/year). There were 2 events of partial flap necrosis, and no cases of total flap loss. One patient required leech therapy for venous congestion. One patient required additional free flap surgery. Two patients developed orocutaneous fistula that resolved with local wound care. One patient developed malocclusion following mandible reconstruction using fibular free flap. Overall free flap success rate was 96%.
Conclusion:
This study supports the ability of small-volume centers to produce positive outcomes with few complications in head and neck cancer free flap reconstructive surgery. While the data are limited to a single surgical team in one care center, it provides additional support for the idea that there are factors beyond the surgical volume that determine outcome.
Introduction
Head and neck tumor extirpation often require complex reconstructive strategy. Free tissue transfer or “free flap” surgery is one surgical technique utilized for reconstructing various head and neck defects. Free flap reconstruction has been widely used by physicians since the late 20th century, with favorable outcomes and high success rates.1,2 The free flap technique requires borrowing a tissue with artery and vein (eg, arm, thigh, or leg), transferring it to a recipient site (eg, tongue, neck, or larynx) and re-establishing the blood supply. Free flaps are a reliable method of reconstruction because they are pliable, not bulky, and allow for repair where tissue may be compromised or of insufficient size.1,2 Nonetheless, free flap reconstruction is not without limitations. For instance, it may not be an option for patients of advanced age with multiple comorbidities or certain tumor pathologies. 1 Operating time is usually 6 to 12 hours in duration, and it requires significant microvascular surgical experience. 2 Because of these technical and logistical difficulties, not all hospitals perform the free flap surgery.
It has been reported that high-volume centers yield better surgical outcomes than small-volume centers, especially when it comes to advanced procedures such as free flap surgery.1-12 However, surgical volume alone does not correlate with successful surgical outcome. It has been shown that surgeon experience, more than center volume, is directly related to successful surgical outcome. 8 Furthermore, growing body of evidence suggests that head and neck surgery with free flap reconstruction can be safely preformed in a low-volume center by assembling an appropriate surgical team.12,13
While there is currently no common accepted definition for “large” and “small” volume centers, the average number of free flaps performed in the United States per center is around 47.8 per year. 13 Over the last 4 years, our institution has performed approximately 6.75 free flap reconstruction surgeries per year for head and neck defects following various tumor extirpation. In this article, we report our experience in free flap success rates and complications in reconstructing various head and neck defects.
Methods
A retrospective review of all patients who underwent head and neck free tissue transfer reconstruction at the Kaiser-Moanalua Medical Center was conducted. The time period of review included 2015 through 2018. All procedures done in this time were performed by a team comprised of the same surgeons (2 head and neck surgeons and 1 plastic and reconstructive surgeon). All cases were done in 2-team approach with one head and neck surgeon (trained in head and neck/skull base surgery with more than 10 years of experience) performing the tumor extirpation. The plastic and reconstructive surgeon, and the second head and neck surgeon (both trained in microvascular surgery with >20 years of combined experience) performed the reconstruction. The 2-team approach promotes surgical efficiency (i.e., reduces operating time) and minimizes surgeon fatigue. All surgeons have extensive training with the surgical and medical management of free flap patients as well as various complications related to free flap surgery.
In the 4 years, 27 cases were identified. Patient records were retrieved, and data were collected regarding the surgical site, origin of free flap, and postoperative complications. The operations were performed by the same surgeons using the same protocol for the 4 years. For each flap, arterial anastomosis was performed with 9.0 nylon under operating microscope and venous anastomosis was performed with micro-Doppler coupler device. All patients were monitored in the intensive care unit at least overnight with hourly Doppler checks continuing for 72 hours. All patients received aspirin 81 mg by mouth or via enteral tube on postoperative day 1.
Results
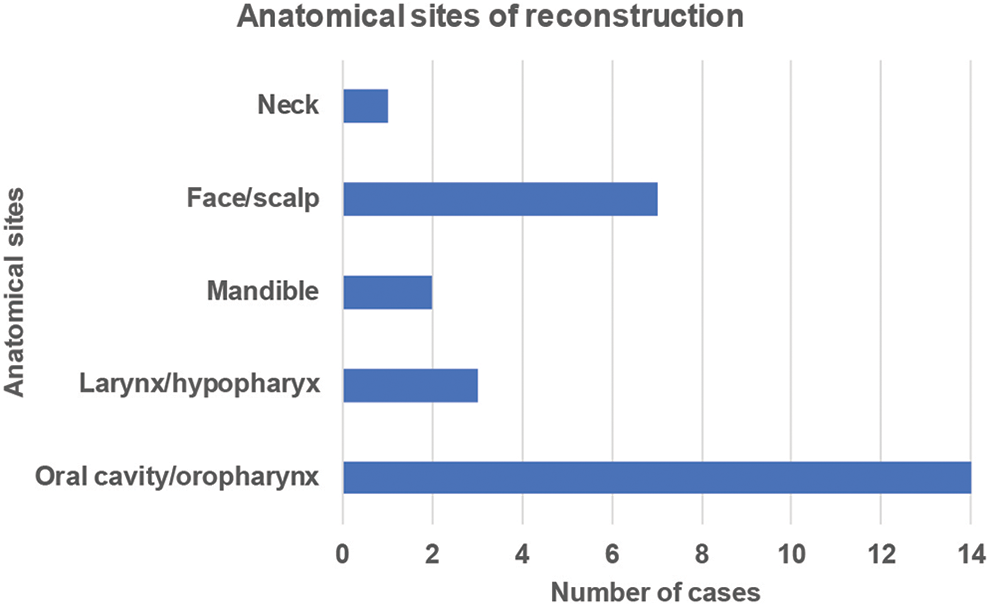
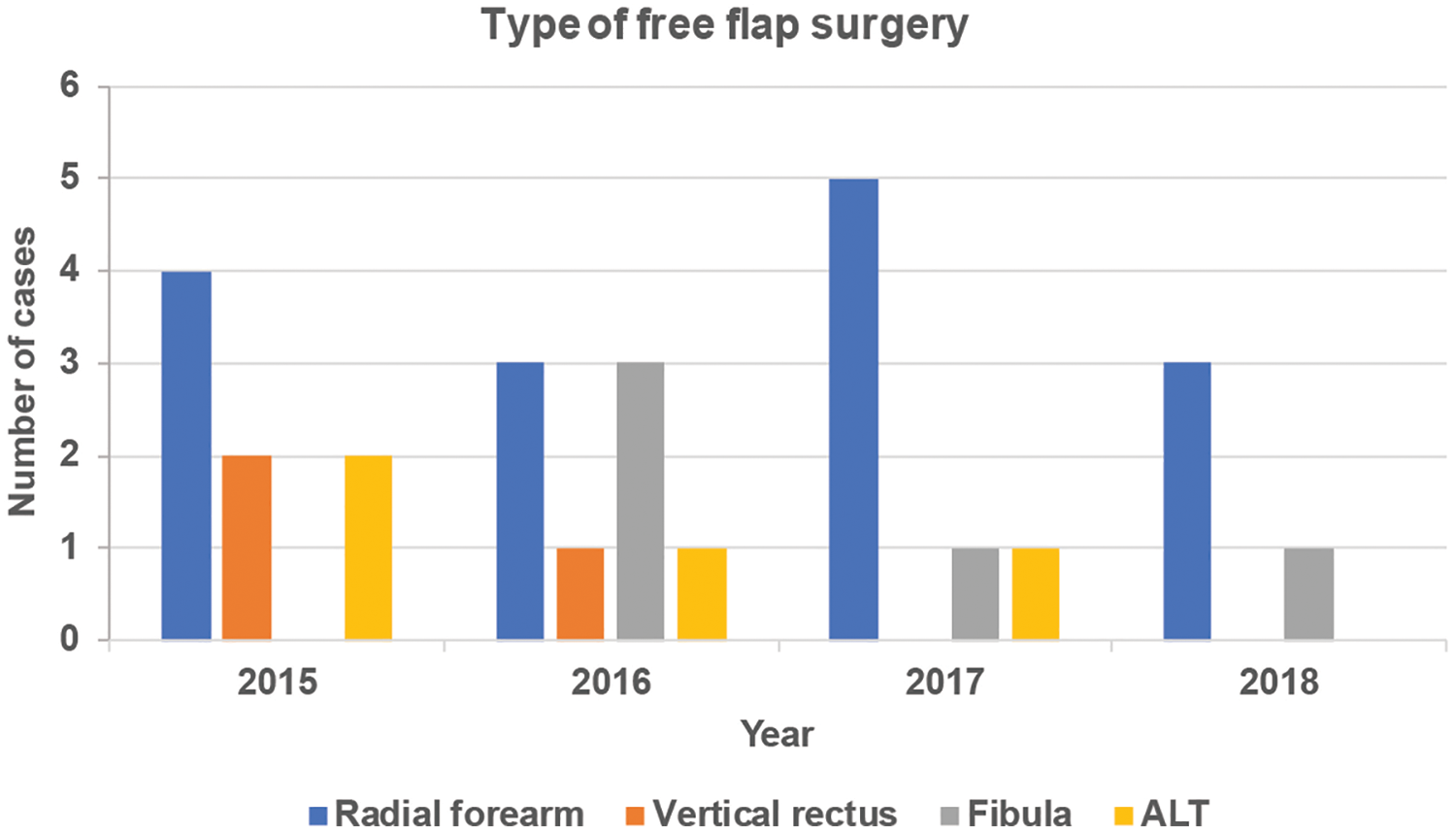
We performed 6.75 free flap operations annually. The radial forearm (n = 15) was the most utilized flap, followed by the fibula (n = 5), anterolateral thigh (n = 4), and lastly the vertical rectus (n = 3; Figure 1). Most common anatomical site for free flap reconstruction was oral cavity and oropharynx, followed by face/scalp, larynx/hypopharynx, and mandible and neck (Figure 2).
Types and number of free flap tissue surgery. Our center performed an average of 6.75 free flap operations per year over a 4-year period: 2015 (8), 2016 (8), 2017 (7), 2018 (4). The radial forearm (n = 15) was the most utilized flap, followed by the fibula (n = 5), anterolateral thigh (ALT; n = 4), and lastly the vertical rectus (n = 3).
Anatomical sites of reconstruction. The most common site of free flap reconstruction following head and neck tumor removal was the oral cavity/oropharynx—14 out of 27 cases. Others include face/scalp (7), larynx/hypopharynx (3), mandible (2), and neck (1).
Out of the 27 free flap transfers performed over 4 years, 21 were free of complications. As shown in Table 1, free flap-specific complications included 2 events of partial flap necrosis, of which one patient required additional free flap surgery following partial flap necrosis. A single-patient experienced venous congestion requiring leech therapy. This patient had prior surgery followed by radiation therapy for tongue base cancer. Two patients developed orocutaneous fistula that resolved with local wound care. One of these patients had previous radiation therapy. Finally, one patient developed malocclusion after fibular free flap reconstruction following mandibular ameloblastoma excision. He underwent subsequent prosthodontic therapy. There were zero instances of total flap loss. Overall free flap success rate was 96%.
Free Flap Specific Complications.
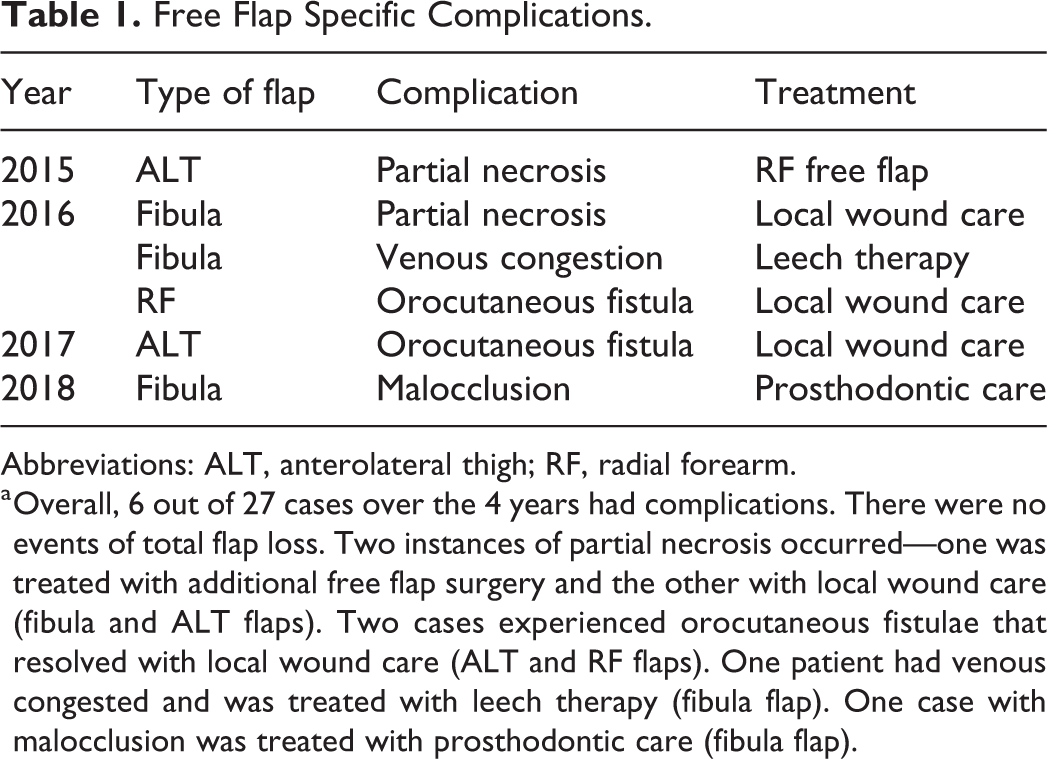
Abbreviations: ALT, anterolateral thigh; RF, radial forearm.
a Overall, 6 out of 27 cases over the 4 years had complications. There were no events of total flap loss. Two instances of partial necrosis occurred—one was treated with additional free flap surgery and the other with local wound care (fibula and ALT flaps). Two cases experienced orocutaneous fistulae that resolved with local wound care (ALT and RF flaps). One patient had venous congested and was treated with leech therapy (fibula flap). One case with malocclusion was treated with prosthodontic care (fibula flap).
Discussion
Our findings support the ability of small-volume centers to produce excellent results with few complications in head and neck cancer free flap reconstructive surgery. Our success rate of 96% is comparable to that of larger institutions. 8 This falls in line with other studies that have aimed to show that smaller programs with an appropriate surgical team and resources are able to safely and successfully perform this operation, providing flexibility and convenience for patients.12,13 In particular, our hospital serves the Hawaiian Islands that are considered to be one of the most geographically isolated locations to practice medicine. Given that most patients prefer to stay locally for treatment where family support plays a critical role in their healing, it is important to identify factors that improve surgical success.
While our data are limited to a single surgical team in one care center, it provides evidence for factors beyond the surgical volume in determining outcome in head and neck free flap surgery. It is widely accepted that better surgical outcomes are achieved by surgeons who perform a higher number of cases; however, some acknowledgment for exceptions to this general rule should be considered.3,8 Several studies have demonstrated the relationship between superior outcomes for surgeons with a high volume of operations across many specialties. These studies have looked at a wide variety of procedures and outcomes, using metrics such as length of hospital stay, postoperative complications, 30-day mortality, operation success, and health care costs.5,6,14 The factors that contribute to a successful operation are numerous and interrelated, such that high volume centers develop experience that translates to shorter hospital stays, fewer complications, and lower overall health care costs. 5 Other proposed benefits include increased technical skills of surgeons, proficiency of ancillary operating room staff, and improved postoperative management.
It is increasingly evident that surgeon experience rather than surgical volume plays an important role in surgical outcome. 8 Specifically, a recent study showed that surgeons with greater years of experience had fewer complications in free tissue transfers than those with less, and that this variable carried more weight than the surgeon’s volume of cases. 7 In addition, surgeons gain applicable experience from surrogate procedures that technically differ from a particular technique such as free flap transfer, but still provide valuable clinical decision-making experience. 8 For instance, this has been studied in the context of vascular procedures and esophagectomies, in which a surgeon’s overall volume (composite) was compared to operation-specific surgeon volume (index operation). 10 These studies have shown that composite volume of operations is the more important variable in determining surgical outcomes in open abdominal aortic aneurysm repairs and esophagectomies.8,10 Surgical procedures that were used as surrogates include a wide array of vascular operations and upper gastrointestinal operations.8,10 As the free flap transfer procedure includes elements of vascular anastomoses and head and neck reconstruction, it is feasible to apply these findings to our procedure of focus. In this sense, head and neck surgeons may transfer skill sets from other head and neck operations (i.e., complex tumor resection, neck dissections, or locoregional flaps, etc) to free flap cases with good outcomes, regardless of the number of free flap transfers they perform per year.
Finally, surgical team dynamics and ancillary staff availability (i.e., speech pathology, respiratory therapy, dietician, occupational therapy, and physical therapy) play crucial roles in success of free flap surgery and the eventual surgical outcome. In order to achieve optimal perioperative patient care, coordination of providers appointments and communication is critical. In our hospital, all our cases are discussed in biweekly Head and Neck Multidisciplinary Tumor Board meeting. Patients also meet with our head and neck cancer care coordinator to receive psychosocial support. During the operation, we utilize the same operating room nurses and surgical techniques (2 separate teams to ensure availability) for all our free flap cases. Moreover, we have trained our intensive care unit as well as surgical ward nurses with Doppler checks and monitoring of patients with free flap reconstruction. There exists a direct communication channel with the surgeons for any medical or surgical-related issues in these patients to quickly remedy potential complications. The assembly of the surgical team takes careful planning, but it is critical to building a successful free flap program.
Conclusion
This study supports the ability of small-volume centers to produce excellent outcomes with few complications in head and neck cancer free flap reconstructive surgery. While the data are limited to a single-surgical team in one care center, it provides additional support for the idea that there are factors beyond surgical volume that determine outcome. Future studies that examine the relationship between volume and outcome in free flap and other surgical procedures should acknowledge the multifaceted relationships that exist among surgical volume, surgeon experience, and hospital support system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.