
Abstract

Case Report
An 8-year-old boy presented to his pediatrician in southern New Jersey with fever, tender bilateral posterior cervical lymphadenopathy, sore throat, and extreme fatigue with refusal to walk for 3 days. He tested positive for streptococcus of the pharynx and was treated with amoxicillin. Six days later, he was changed to amoxicillin–clavulanate for failure to improve. Two days later, he presented to an emergency department for persistent fever, worsening cervical posterior lymphadenopathy, and a diffuse macular rash of the face, trunk, chest, and palms. At this visit, his mother recalled a tick bite on his scalp prior to the onset of symptoms that had resulted in a small eschar. Laboratory testing was performed, which showed a white blood cell count of 11.2 with mildly elevated absolute lymphocyte and absolute monocyte counts and mildly elevated liver function testing results. Monospot and Lyme testing results were negative. The antibiotic was changed to clindamycin, which also failed to improve the symptoms. Magnetic resonance imaging (MRI) of the neck was performed and revealed bilateral suppurative lymphadenopathy with internal septations (Figure 1A and B). An incision and drainage with excisional biopsy was performed with pathology demonstrating extensive histiocytosis and granulomatous inflammation (Figure 2). Tissue cultures grew tiny, faintly staining Gram-negative coccobacillus consistent with Francisella tularensis (Figure 3). The patient was seen in the office 4 to 6 weeks postoperatively with no recurrence or complaints.
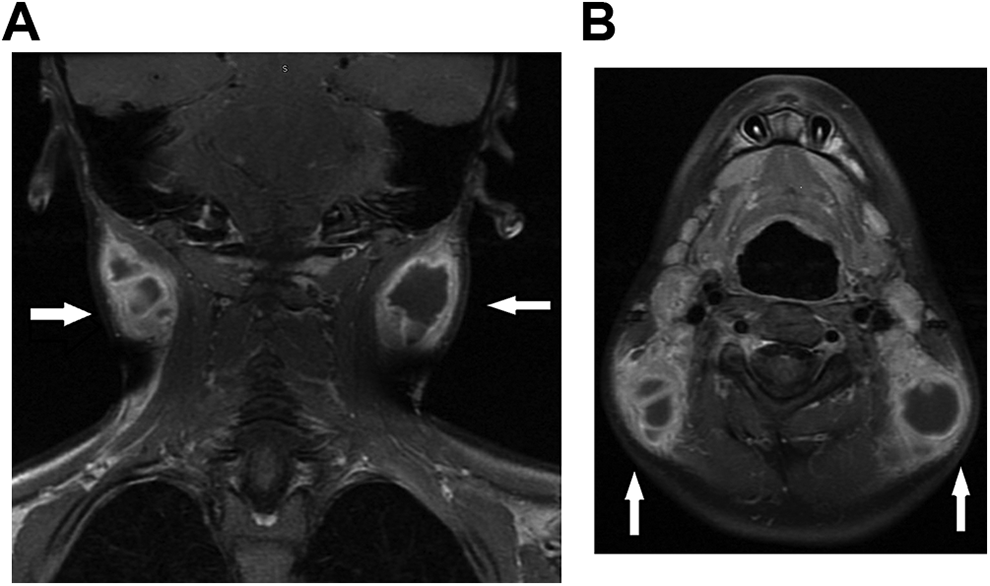
A, Coronal magnetic resonance imaging (MRI) depicting bilateral cervical lymphadenopathy, B. Axial MRI depicting bilateral cervical lymphadenopathy.
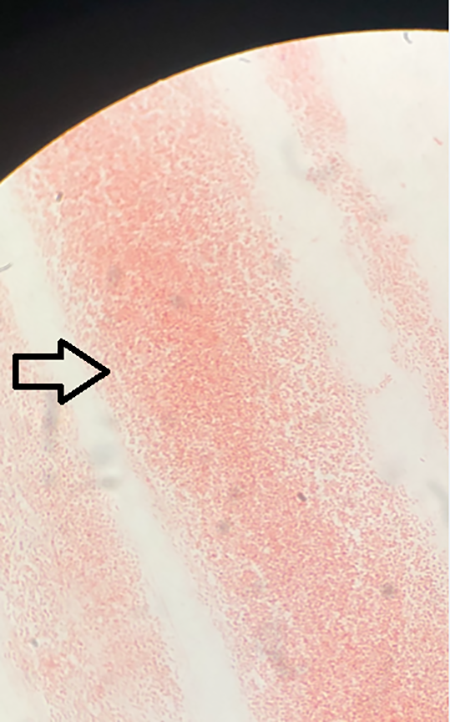
Pathology slide demonstrating extensive histiocytosis and granulomatous inflammation.
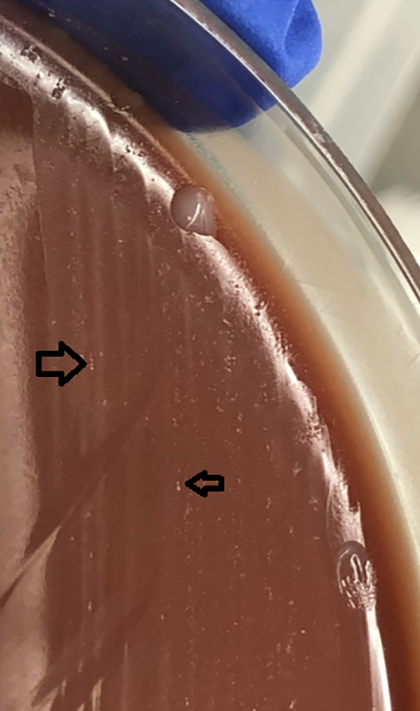
Tissue culture plate growing tiny, faintly staining Gram-negative coccobacillus consistent with Francisella tularensis.
Discussion
Tularemia is a zoonotic disease caused by the highly virulent bacteria F tularensis. Although not transmissible from human to human, even a small inoculum may result in disease. Ulceroglandular tularemia is the most common form, accounting for approximately 80% of tularemia cases. 1 In this form, a skin ulcer appears where the bacteria enters the body, and the patient will usually present with a flu-like illness followed by lymphadenopathy. Cervical or occipital adenopathy is more common in children than adults who present with inguinal lymphadenopathy. 2 Because symptoms of ulceroglandular tularemia are nonspecific, other causes of lymphadenitis including Staphylococcus, Streptococcus, Bartonella henselae, nontuberculous mycobacteria, Epstein-Barr virus, cytomegalovirus, and other infectious causes should be considered. 3 Other forms of tularemia include glandular, oculoglandular, oropharyngeal, pneumonic, and typhoidal. 4
Francisella tularensis infections are acquired by inhalation; ingestion; contact with infected animals; or contact with lagomorphs, rodents, ticks, or other insect vectors. 5 Approximately 100 to 300 cases annually are reported in the United States, with most outbreaks occurring in Arkansas, Missouri, Kansas, Nebraska, and Oklahoma. Only 130 other cases of tularemia have been reported in the northeastern United States from 2007 to 2017. Deer flies, horse flies, American dog ticks, lone star ticks, and Dermacentor variabilis are the most commonly implicated ticks in the Northeast. 2
Results of serologic testing may be negative for the first 2 to 3 weeks of infection. 6 Therefore, diagnosis and effective clearance requires a detailed medical history and thorough physical examination. It is important to elicit a history of recent exposure to cats, rabbits, and rodents or presence in wooded areas and tick-infested regions. Constitutional symptoms including fever, chills, myalgias, gastrointestinal manifestations, decreased activity, and refusal to walk are commonly described in pediatric tularemia. An ulcerative lesion may be hidden in the scalp, a common site for tick bites.
Ultrasound may demonstrate suppurative lymphadenopathy, but computed tomography or MRI are often required to determine nodal characteristics and extent of disease. 7 Other pediatric cases have also reported multiloculated masses with enhancing septa in the posterior cervical nodal chains. 8 Presumptive tularemia is diagnosed using direct fluorescent antibody, immunohistochemistry, or polymerase chain reaction analysis. While definitive diagnosis is verified by cultures, organisms in culture are highly infectious and testing must be performed in Biosafety Level 2 laboratories. 4 Laboratory personnel should be notified if there is a clinical concern for tularemia, and confirmed cases must be reported to the Centers for Disease Control and Prevention. Streptomycin is currently the medical therapy of choice, 9 with surgical drainage reserved for abscess formation. If left untreated, tularemia may cause bacteremia and lead to mortality. Effective management, particularly in this population, is rooted in early diagnosis and targeted therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.