
Abstract
Objective:
Chronic suppurative otitis media (CSOM) is mostly caused by bacterial infection of the middle ear and antibiotics are generally used empirically, which may lead to the emergence of resistant bacterial strains. The objective of the study is to assess the bacteriological profile of and evaluate the antibiotic susceptibility of strains isolated in a tertiary care hospital in Shanghai, China.
Methods:
This study included 289 individuals with clinical diagnosis of CSOM. Middle ear purulent discharge was obtained with sterile swabs and cultured for bacterial pathogens. The susceptibility of the isolated microorganisms to antibiotics was assessed by a microdilution method.
Results:
Bacterial pathogens were found in 223 (77.2%) of the 289 cases. A total of 236 strains were isolated. Staphylococcus aureus was the commonest bacteria (44.9%) followed by Pseudomonas aeruginosa (16.9%) and coagulase-negative Staphylococcus (8.5%). There were 18.9% methicillin-resistant S aureus (MRSA) among the obtained S aureus organisms. Multidrug-resistant P aeruginosa was found in 4 patients, making up 10% of all detected P aeruginosa. Staphylococcus aureus showed highest susceptibility to vancomycin (100%), then gentamicin (98.1%) and rifampicin (97.2%) and was most resistant to penicillin (61.3%) and erythromycin (50%). All isolated P aeruginosa showed susceptibility to piperacillin, piperacillin/tazobactam, and meropenem. High degree of resistance in P aeruginosa was observed toward levofloxacin (42.5%), ciprofloxacin (40%), and ceftriaxone (30%).
Conclusion:
The high prevalence of MRSA and fluoroquinolone-resistant P aeruginosa indicated cephalosporins and fluoroquinolone as primary empirical antibiotic drugs in CSOM to be cautiously used. In order to reduce the incidence of resistant strains and promote effective usage of antibiotics, all aural discharges should be cultured to determine antibacterial susceptibility patterns before treatment.
Introduction
Chronic suppurative otitis media (CSOM) is characterized by repeated otorrhea via tympanic membrane perforation. Chronic suppurative otitis media often leads to conductive hearing loss and constitutes a risk factor for permanent sensorineural hearing loss because of inner ear injury as well as intracranial complications. 1 Globally, 21 000 individuals succumb yearly to CSOM complications. 2 The average global incidence rate of CSOM is estimated at 4.76/1000 individuals, totaling 31 million cases (all ages) per year; among the patients, 22.6% are below 5 years of age. 2 Chronic suppurative otitis media prevalence is high in nonindustrialized nations. The highest prevalence rates of pediatric CSOM are found in Alaska, Canada, and Greenland, American Indians, and Australian Aborigines, ranging between 7% and 46%. 1 Unfortunately, the exact morbidity of CSOM in China is not well documented.
Chronic suppurative otitis media is mostly caused by bacterial infection of the middle ear. Many studies from different countries have reported common pathogens causing CSOM. Some studies considered Pseudomonas aeruginosa (P aeruginosa) the commonest pathogen, while other studies showed that Staphylococcus aureus (S aureus) is the most predominant pathogen. 3 The discrepancies among the various studies might result from the patient populations and geographical areas assessed. Chronic suppurative otitis media is primarily treated with combined ear cleaning and topical antimicrobial drops. Systemic antibiotic drugs are advised when primary treatment fails or in case of intracranial complication occurrence in CSOM. Antibiotics are generally used empirically, which may lead to the emergence of resistant bacterial strains. Multiple studies have assessed antibiotic susceptibility and resistance patterns of bacterial pathogens.4-6 However, few studies have focused on CSOM etiology and bacterial resistance in China.
Since CSOM pathogenesis and etiology remain poorly understood, 3 assessing the rates of various pathogens in different regions is critical. Moreover, identifying the bacterial spectrum and susceptibility to antimicrobials is essential for efficient empirical treatment, and would help better understand CSOM. Therefore, this work aimed to document CSOM’s bacteriological profile and evaluate antibiotic susceptibility in CSOM patients.
Materials and Methods
The retrospective study was conducted in patients visiting the outpatient department of otorhinolaryngology in a tertiary care hospital from March 2016 to December 2018, who presented with ear discharge (one or both ears) and tympanic membrane perforation with or without cholesteatoma for at least 2 weeks. In all, 289 patients with a clinical diagnosis of CSOM were included. The patients had not received antibiotic agents (administered systemically or topically) within 1 week before enrollment.
A comprehensive medical history was obtained for each patient. The patient’s external auditory canal was cleansed using sterile ethanol-soaked swabs. A curved sterile swab was stretched into the middle ear through the perforated eardrum, and the purulent discharge was collected. These specimens were then sent for bacterial examination.
The collected purulent swabs underwent culture on blood and MacConkey agar plates at 37 °C overnight. Pathogen identification was carried out by routine methods for bacterial organisms. Antibiotic susceptibility testing was undertaken by a microdilution method to determine the minimum inhibitory concentration, and result interpretation followed Clinical and Laboratory Standard Institute guidelines.
Results
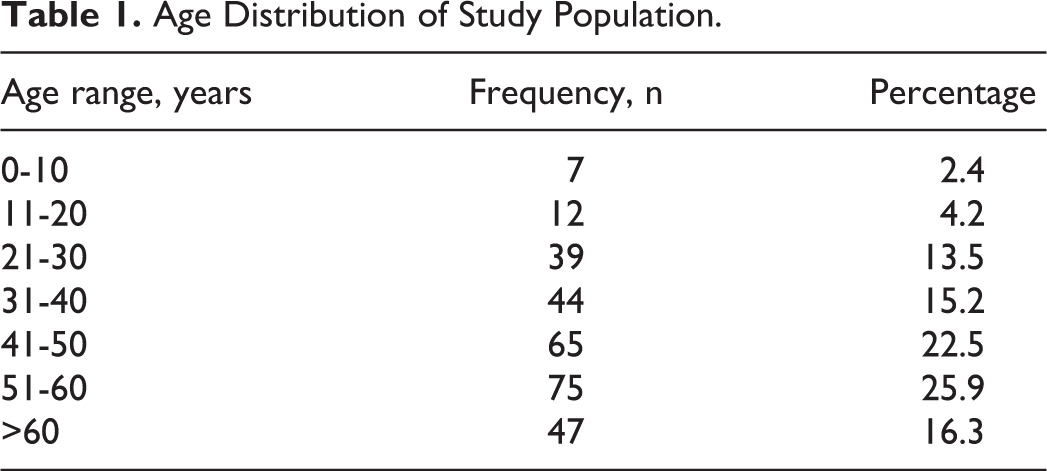
A total of 289 CSOM cases were included in the study. One hundred fifty-nine (55%) (n = 159) patients were males and 45% (n = 130) were females. The patients were 1 to 87 years old (mean of 45.1 years). The highest disease rate (25.9%) occurred between 51 and 60 years (Table 1). From a total of 289 ears, no bacteria could be cultured in 66 ears (22.8%), while 223 ears (77.2%) had positive cultures. Single microbial isolates were found in 211 cases (94.6%), and multiple bacteria were isolated in 12 cases (5.4%). Of these 223 patients with positive cultures, 188 (84%) were CSOM without cholesteatoma, and 35 (16%) were CSOM with cholesteatoma. A total of 236 strains were isolated from the 223 positive samples, including 142 strains of Gram-positive bacteria (60.2%) and 94 strains of Gram-negative bacteria (39.8%), indicating the predominance of the former group (Table 2). Of the 236 strains, 198 (84%) were derived from CSOM patients without cholesteatoma and 38 (16%) were from patients with cholesteatoma.
Age Distribution of Study Population.
Distribution of All Isolated Bacteria.
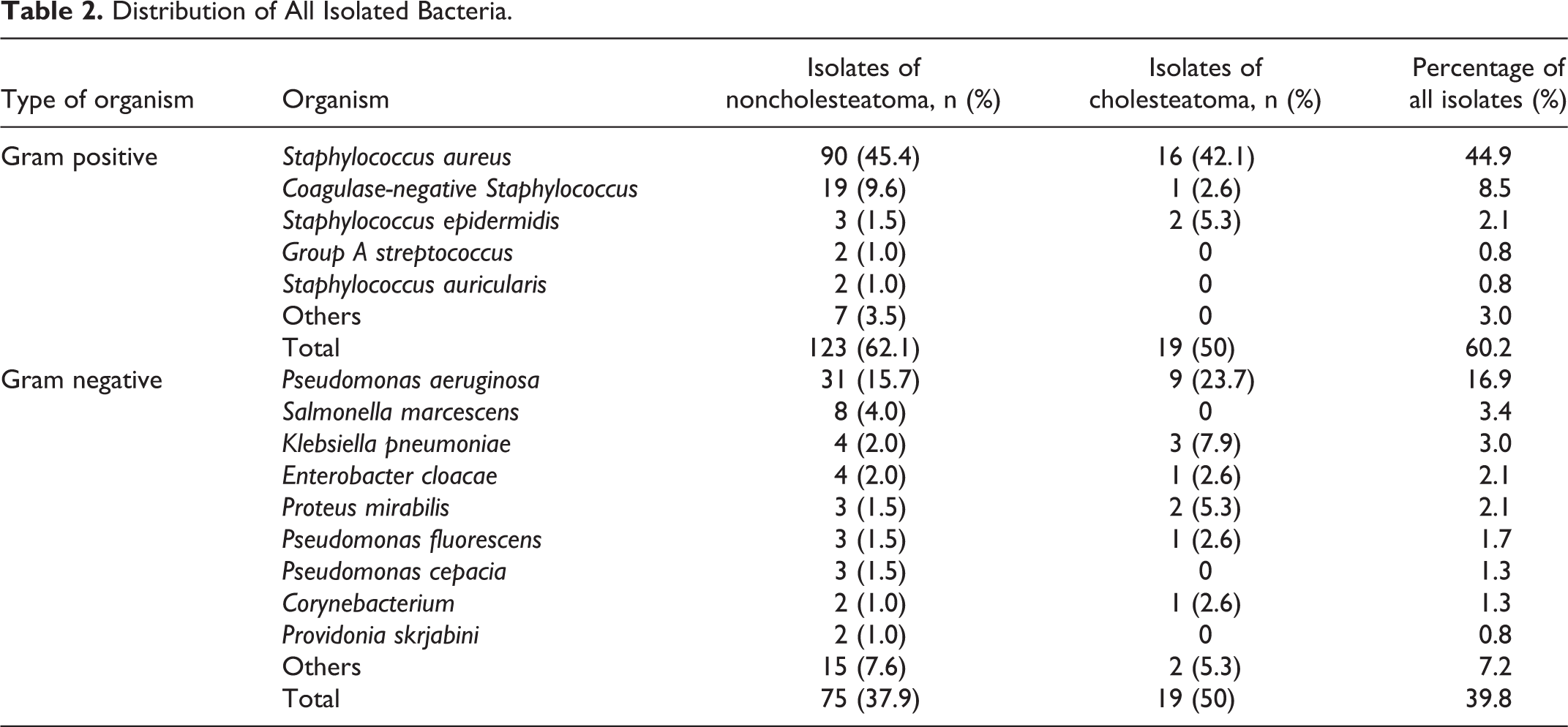
Staphylococcus aureus was the most represented microorganism identified in the cultured specimens. It was present in 106 patients and accounted for 44.9% of all cultured bacteria. Similar results were found when the patients were classified into those without cholesteatoma and with cholesteatoma. In the former, S aureus (90/198, 45.4%) was the most common bacteria. In the latter, S aureus (16/38, 42.1%) was also the most prevalent bacteria (Table 2). Mixed isolates revealed S aureus in coexistence with P aeruginosa (2.8%, n = 3), Salmonella marcescens (0.9%, n = 1), Klebsiella pneumoniae and Pseudomonas stephensi (0.9%, n = 1), and beta-hemolytic group A Streptococcus (0.9%, n = 1) in S aureus positive cultures. Pseudomonas aeruginosa was the second most common bacteria and isolated from 40 ear swab specimens, accounting for 16.9% of all isolates. Furthermore, 31 of P aeruginosa strains were isolated and accounted for 15.7% (31/198) of all isolates in CSOM patients without cholesteatoma. Nine of P aeruginosa strains were isolated and accounted for 23.7% (9/38) of all isolates in CSOM patients with cholesteatoma (Table 2). We isolated mixed flora of P aeruginosa with S aureus (7.5%, n = 3) and Enterobacter cloacae (2.5%, n = 1) in P aeruginosa positive cultures. Coagulase-negative Staphylococcus was isolated from 20 patients and accounted for 8.5% of all cultured bacteria, and no mixed flora with other bacteria was demonstrated. Klebsiella pneumoniae was isolated in only 7 patients, and no mixed flora with other bacteria was found. However, in CSOM patients with cholesteatoma, K pneumoniae was the third most common bacteria (7.9%, n = 3). In CSOM patients without cholesteatoma, Coagulase-negative Staphylococcus was the third most common bacteria (9.6%, n = 19).
Staphylococcus aureus, P aeruginosa, and Coagulase-negative Staphylococcus were the 3 main otopathogens responsible for CSOM. Table 3 shows S aureus’s antimicrobial susceptibility pattern. Methicillin-resistant S aureus (MRSA) was isolated from 20 ears and constituted 18.9% of all S aureus isolates. All isolated S aureus organisms were sensitive to vancomycin. Only 38.7% (n = 41) of S aureus isolates were sensitive to penicillin, which showed the lowest antibacterial activities. The antibiotics most active against bacteria were vancomycin (100% killing), gentamicin (98.1%), and rifampicin (97.2%). Table 4 shows the antimicrobial susceptibility pattern of P aeruginosa. Multiresistant P aeruginosa was found in 4 patients and accounted for 10% of all P aeruginosa isolates. All isolated P aeruginosa were sensitive to piperacillin, piperacillin/tazobactam, and meropenem. However, 4 P aeruginosa isolates were resistant to imipenem. The isolated P aeruginosa were very resistant to levofloxacin (42.5%), ciprofloxacin (40%), and ceftriaxone (30%). Table 5 shows the antimicrobial susceptibility pattern of coagulase-negative Staphylococcus. Vancomycin (100%), rifampicin (100%), and tetracycline (100%) were the most effective antibiotics, followed by chloramphenicol (90%). The majority of coagulase-negative Staphylococcus were resistant to penicillin (70%, 14/20) and erythromycin (55%, 11/20). Fluoroquinolones are the most common topical antibiotics; 58 patients (26%, 58/223) were resistant to treatment by ofloxacin or levofloxacin.
Staphylococcus aureus Strains Susceptible and Resistant to Each Antibiotic Class.a
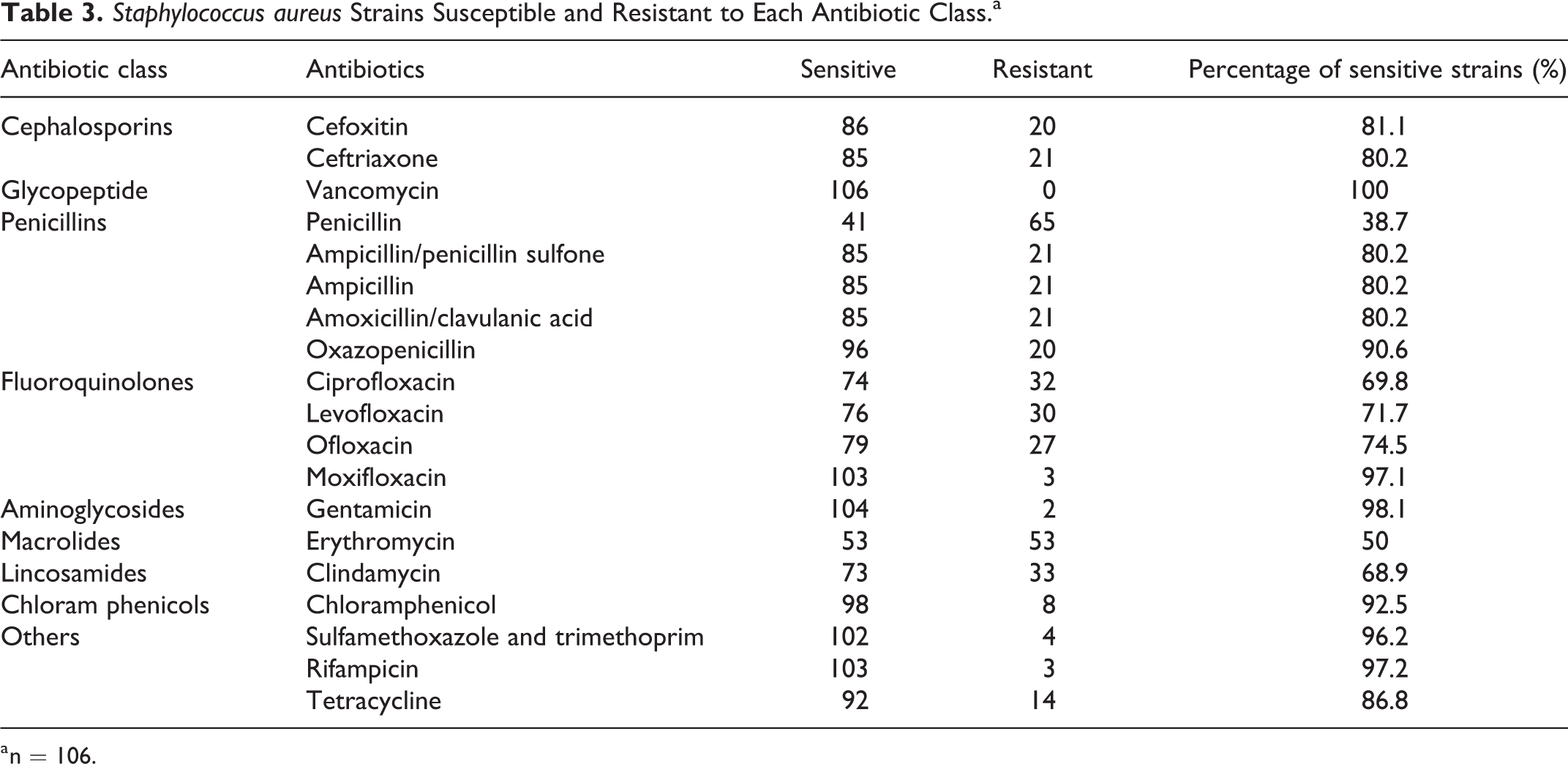
a n = 106.
Pseudomonas aeruginosa Strains Susceptible and Resistant to Each Antibiotic Class.a
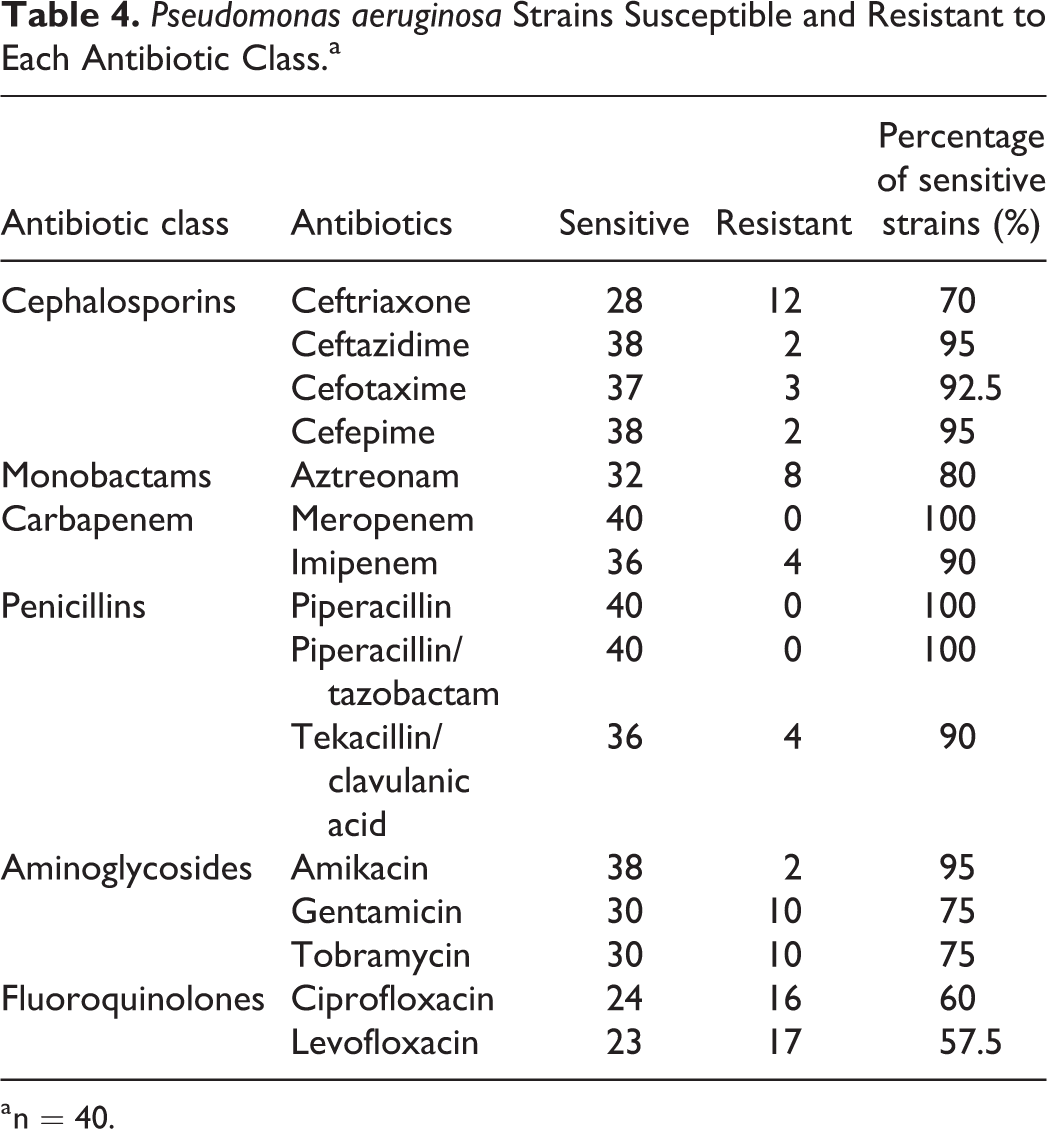
a n = 40.
Coagulase-Negative Staphylococcus Strains Susceptible and Resistant to Each Antibiotic Class.a
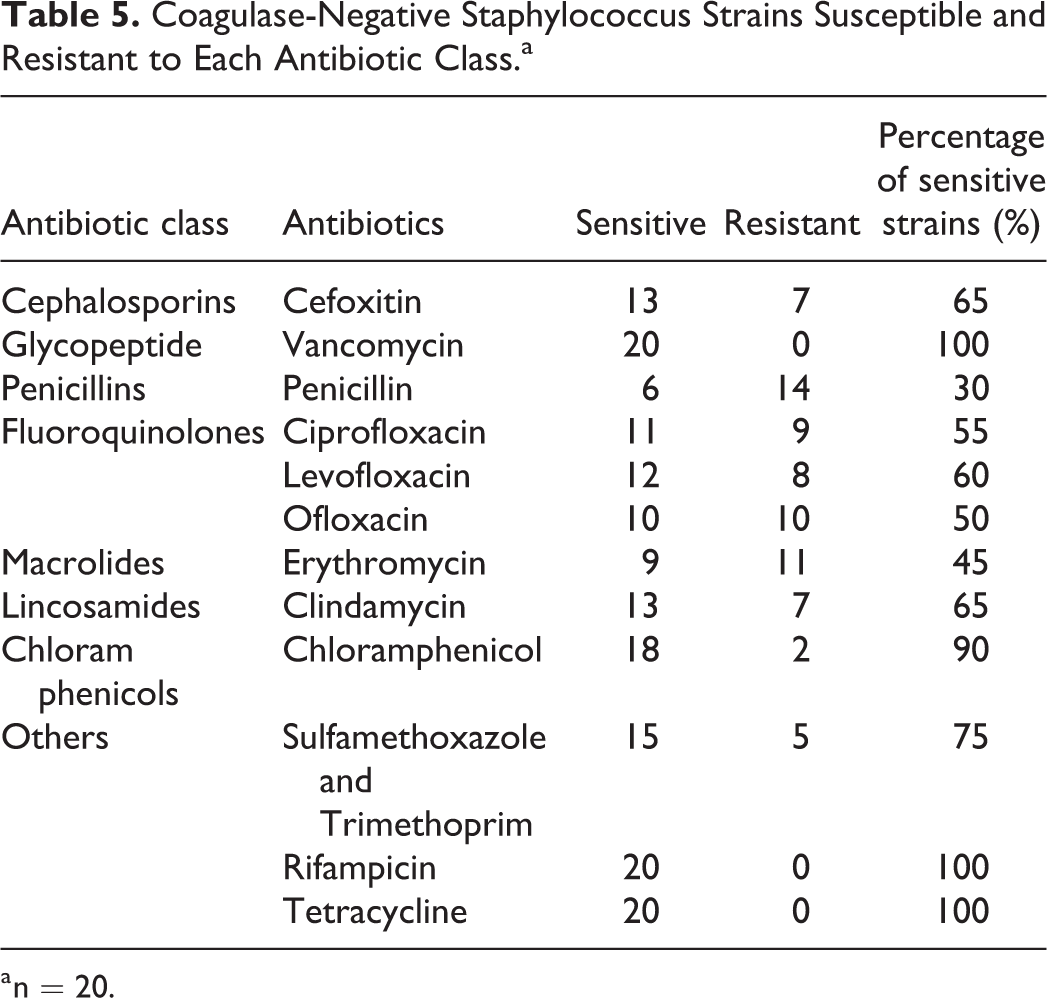
a n = 20.
Discussion
Chronic suppurative otitis media is also a particularly prevalent infection in China like most other developing countries. It is believed that CSOM is mostly the consequence of unresolved acute otitis media (AOM), although how the acute infection develops into a chronic disease remains largely unclear. No precise prevalence of CSOM has been reported in China. However, AOM incidence in China ranges from 57.2% to 69.4% in children aged 0 to 2 years. 7 Therefore, we hypothesized that CSOM prevalence is also high in China. Chronic suppurative otitis media is mostly diagnosed in children 5 years and below. 1 In this study, the highest rate of 25.9% was found in 51 to 60-year-old individuals. However, the percentage of CSOM in the 0- to 10-year age-group was only 2.5%. The reason may be that our hospital mainly treats adults, and most pediatric patients consult otolaryngologists in the children’s hospital. Here, CSOM was predominantly found in males (55%), corroborating a previous work. 8
To avoid otorrhea contamination by bacterial organisms from the external auditory canal, the later underwent sterilization before otorrhea sampling, and cotton swabs were employed to stretch into the middle ear for purulent collection as described in the experimental section. The normal external auditory canal bacterial flora mainly comprises Staphylococcus epidermidis, Staphylococcus auricularis, Staphylococcus capitis, and Corynebacterium. 9 As shown above, S aureus and P aeruginosa were detected most frequently, indicating that the samples were likely not contaminated by bacteria of the external auditory canal.
The majority of bacteriology studies of CSOM have been conducted in underdeveloped nations, 3 indicating high prevalence rates. We used blood and MacConkey agar plates to culture bacteria, which were also routine culture methods for middle ear samples. As shown above, positive cultures were found in 77.2% cases, a rate which was lower than in some studies. Three studies performed in Iran, 5 India, 10 and Pakistan 11 reported rates of 97.3%, 91%, and 91.4% for positive cultures, respectively. However, our results were in line with a study carried out in Korea, 12 which showed a rate of 75.5%. These discrepancies are likely due to differences in methodology, sample size, antibiotic treatment before bacteriologic testing, infection by slowly replicating pathogens, and/or local hygienic conditions. In our study, culture of anaerobic bacteria wasn’t performed. But the role of anaerobic bacteria in CSOM is often controversy. Only when extensive cholesteatoma or granulation tissue exits, anaerobic bacteria may be detected. There has been much discrepancy on the results of previous studies. Some studies isolated anaerobic bacteria in CSOM; however, other studies found negligible anaerobes. 13
Mixed bacterial infections of the middle ear are often reported. Two studies in India showed polymicrobial growth in 1.3% 10 and 5.2%, 14 respectively. In this study, single microbial isolates were found in 211 cases (94.6%), and multiple bacteria were isolated in 12 cases (5.4%).
Staphylococcus aureus, the predominant microorganism in the current study, was identified in 106 patients and accounted for 44.9% of all cultured bacteria. It was followed by P aeruginosa, which was isolated in 40 ear swab specimens and constituted 16.9% of all cultured bacteria. A similar result was observed between patients with cholesteatoma and noncholesteatoma. Staphylococcus aureus was the most common bacteria, followed by P aeruginosa in the 2 groups. These results were similar to those of previous studies,4,14 in which S aureus and P aeruginosa were, respectively, first and second most frequent organisms. However, other studies11,15 identified P aeruginosa as the predominant microorganism followed by S aureus. A study performed in Beijing, China, reported coagulase negative Staphylococcus (20.34%) as the most prevalent bacterial organism, surpassing P aeruginosa (16.95%) and S aureus (14.69%). 16 Recently, a study in Angola 17 revealed Proteus spp. as the most commonly cultured bacterial organism, which was followed by P aeruginosa and Enterococcus spp. Another study carried out in Malawi 18 also found Proteus mirabilis to be the most prevalent aerobic bacterial entity, with P aeruginosa, and S aureus as second and third, respectively. However, in this study, P mirabilis was only identified in 5 (5.1%) patients. These differences may be attributed to sample size and geographical variations.
Antibiotic susceptibility patterns are employed to select optimal antibiotics for treating CSOM. In China, most patients with CSOM show preference to oral antibacterial drugs, which are routinely prescribed, sometimes in combination with topical antibiotics. The most prescribed oral antibiotics for CSOM in China are cephalosporins and fluoroquinolone. As shown above, the rates of S aureus resistance to cefoxitin and ceftriaxone were 18.9% and 19.8%, respectively. Staphylococcus aureus isolates identified in this study were highly resistant to penicillin (61.3%) and erythromycin (50%). Meanwhile, S aureus isolates were highly susceptible to vancomycin (100%), gentamicin (98.1%), rifampicin (97.2%), moxifloxacin (97.1%), and sulfamethoxazole and trimethoprim (96.2%). In the current study, the susceptibility rates of S aureus to levofloxacin and ofloxacin were 76% and 79%, respectively. Empirical antibiotic drugs, for example, ciprofloxacin, are very efficient against multiple Gram-positive and Gram-negative bacterial organisms responsible for CSOM.19,20 However, in this work, the rates of S aureus and P aeruginosa susceptibility to ciprofloxacin were only 69.8% and 60%, respectively, which were consistent with a Nigerian study. 4 Chronic suppurative otitis media secondary to community-acquired MRSA infection was found to be increased from 0.7% to 11.4% from 1998 to 2006. 21 In this study, MRSA was isolated from 20 ears and constituted 18.9% of all S aureus. It is thought that CSOM develops after an unsuccessfully treated AOM infection. 1 A study assessing AOM in China reported 23.5% of the isolated S aureus to be MRSA. 22 A study in Korea reported an isolation rate of MRSA in all S aureus isolates of 22.8%. 12 However, an Indian study showed that MRSA infection in CSOM accounts for 34.3% (123/359) of all S aureus. 23 In this study, 12/20 of MRSA isolates showed resistance to ciprofloxacin, and all of them were cefoxitin, ceftriaxone, and penicillin resistant. The most effective antibiotics against MRSA were vancomycin (100%) and gentamicin (100%). However, gentamicin has ototoxicity and is seldom used for CSOM. The current data suggest cephalosporins and ciprofloxacin should be cautiously employed as first line of treatment in CSOM.
Pseudomonas aeruginosa associated CSOM is routinely treated with aminoglycosides, fluoroquinolones, and cephalosporins. Due to ototoxicity described for aminoglycosides, the most commonly used antibiotics in China are fluoroquinolones and cephalosporins. Meanwhile, P aeruginosa susceptibility to the latter drugs shows variability and unpredictability. The occurrence of multidrug-resistant (MDR) organisms further complicates antibiotic selection. In the current study, MDR P aeruginosa was isolated from 4 patients and constituted 10% of all P aeruginosa. All MDR P aeruginosa organisms isolated here showed resistance to aztreonam, gentamicin, tobramycin, ciprofloxacin, and levofloxacin. Meanwhile, the isolated P aeruginosa all showed susceptibility to piperacillin, piperacillin/tazobactam, and meropenem. However, 4 isolated P aeruginosa were resistant to imipenem. Imipenem-resistant isolates had high prevalence rates of resistance to ciprofloxacin (75%) and levofloxacin (75%). Pseudomonas aeruginosa isolates were highly resistant to levofloxacin (42.5%), ciprofloxacin (40%), and ceftriaxone (30%). These results suggest that fluoroquinolone as a first-line antibiotic in P aeruginosa infection should be reconsidered.
The only Food and Drug Administration (FDA)-approved nonototoxic ear drops contain ofloxacin or ciprofloxacin. The most common topical antibiotics in China are levofloxacin and ofloxacin drops. In this study, 58 cases with positive cultures (26%, 58/223) were resistant to ofloxacin or levofloxacin. A high prevalence of fluoroquinolone-resistant strains, especially resistant P aeruginosa, suggested that systemic fluoroquinolones should not be used as first-line treatment agents for CSOM. However, topical fluoroquinolones may be effective in patients with fluoroquinolone-resistant strains, because a topical otic solution of fluoroquinolone yields a high drug concentration in otorrhea. Although ototopical administration is effective in most cases with otorrhea, refractory and recurrent suppurative otitis media has been reported. In such cases, systemic antibiotics are also necessary. Therefore, before antibiotic administration locally or systemically, it is imperative to culture aural discharges from CSOM patients and obtain antimicrobial susceptibility patterns, to best guide antibiotic usage.
However, there were some limitations to the present study. Our culture method couldn’t identify all pathogens. The limited pediatric patients made it difficult to compare the difference with adult patients. In addition, the sample size was not large enough and there was a lack of a multicenter design.
Conclusion
Overall, these findings demonstrated that S aureus is the most frequent etiologic agent of CSOM, followed by P aeruginosa. Occurrence of MRSA and fluoroquinolone-resistant P aeruginosa strains indicated that cephalosporins and fluoroquinolone should be cautiously employed as common first-line antimicrobials in CSOM. In order to reduce the occurrence of resistant strains, all aural discharges should be cultured for identifying antibacterial susceptibility patterns.
Footnotes
Authors’ Note
Jianghong Xu and Qiang Du contributed equally to this work. The patients enrolled in the study gave their informed consent, and the study protocol was approved by the Institutional Review Board of Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.