
Abstract
Objective:
To compare local anesthesia (LA) versus general anesthesia (GA) for balloon dilation of the Eustachian tube (BDET) using the Bielefeld Dilation System in a Chinese population with obstructive Eustachian tube dysfunction (OETD).
Methods:
A total of 49 patients with OETD undergoing BDET under either LA or GA were included in the present study. Intraoperative blood pressure, heart rate, and pain sensation were recorded. The surgical outcome was assessed by Eustachian Tube Dysfunction Questionnaire-7 (ETDQ-7) symptom scores and positive Valsalva maneuver at baseline, 1 day, 2-, 4-, 12-, 24-, and 52-week follow-up.
Results:
Balloon dilation of the Eustachian tube procedures were successfully completed in all patients without adverse effects. The visual analog scale score for maximal pain during the surgical procedure in the LA group was 6.1 ± 1.0. Intraoperative blood pressure and heart rate were higher in the LA group compared with the GA group. The duration and costs of surgery were significantly reduced in the LA group compared with the GA group. Normalization of ETDQ-7 scores at 12-week and 52-week follow-up was observed in 71.9% (23/32) and 63.3% (19/30) of patients in the LA group, respectively, which was comparable to that of the GA group. Although improvement in positive Valsalva maneuver was observed in both groups after BDET, more patients reported positive Valsalva maneuver in the GA group compared with the LA group at 12-week and 52-week follow-up. In total, 96.0% (24/25) of patients in the LA group and 95.8% (23/24) of patients in the GA group would choose LA if BDET was needed again.
Conclusion:
Balloon dilation of the Eustachian tube under LA is safe and feasible in a Chinese population. The surgical outcome of BDET is comparable between under LA and GA during 52-week follow-up. Further studies are needed to address management of intraoperative pain and determine longer follow-up outcome for BDET under LA.
Introduction
Eustachian tube dysfunction (ETD) is a syndrome with a collection of signs and symptoms including aural fullness, otalgia, muffle hearing, tinnitus, and hearing loss, which suggests dysfunction of the Eustachian tube. 1 Eustachian tube dysfunction can be broadly categorized into 2 major subtypes: obstructive dysfunction and patulous dysfunction. Obstructive ETD (OETD) is the most common subtype of ETD and has been estimated to have a global prevalence of around 1% in adults. 2,3 Although there are several medical and surgical treatments aimed to deal with OETD, the treatment results are often less satisfactory. 4 Recently, several studies provided evidence for balloon dilation of the Eustachian tube (BDET) as an effective treatment option, with symptoms improved in 55% to 98% of patients during up to 12-month follow-up. 5 -8 Currently, the majority of BDET procedures are performed under general anesthesia (GA). With the growing number of patients with OETD requiring BDET and considering the short duration of BDET procedure, performing BDET under local anesthesia (LA) would have significant advantages over GA, such as faster patient recovery and reduced treatment costs.
Catalano and colleagues first described the feasibility of BDET under LA. 9 Although all procedures under LA were successfully completed, the dilation time varied from 10 to 30 seconds and dilation pressure varied from 6 to 8 atmospheres of pressure (atm). Then, Luukkainen and colleagues showed that no adverse effects were detected in BDET under LA using a pressure of 10 to 12 atm and a dilatation time of 2 minutes. 10 Recently, Meyer and colleagues reported that 72% of the BDET procedures were performed under LA without complications in a randomized controlled trial, and the symptoms of patients with OETD were significant improved even at 12-month follow-up. 11 However, these studies were performed only in a Western population. Moreover, there were 2 dilation systems (the AERA Dilation system and the Xpress Dilation System) used in these reports, while the most used dilation system in China is the Bielefeld Dilation System. 12 Most importantly, the surgical outcome of BDET was not compared between under LA and GA yet.
In this study, we aimed to confirm the safety and feasibility of BDET procedure using the Bielefeld Dilation System under LA in a Chinese population with OETD and also compare surgical outcome between BDET under LA and GA during 52-week follow-up.
Patients and Methods
Patients
Patients diagnosed with OETD and treated with BDET either under LA (the LA group) or under GA (the GA group) in Sun Yat-sen Memorial hospital, Sun Yat-sen University between September 2015 and April 2019 were retrospectively analyzed. All enrolled patients had persistent symptoms for at least 3 months and refractory to medical treatment. Obstructive ETD was defined by patient-reported symptoms that meet the criteria of mean item score ≥2.1 of the Eustachian Tube Dysfunction Questionnaire-7 (ETDQ-7) after exclusion of patulous ETD. 13,14 Exclusion criteria involved temporomandibular joint disorders, endolymphatic hydrops, rhinosinusitis, allergies, reflux disease not controlled with medication, anatomic conditions or mass that blocking the nasal access to the Eustachian tube, narcotic allergy, and severe cardiopulmonary disease. The study was approved by the ethical review board of Sun Yat-sen Memorial Hospital, Sun Yat-sen University, and informed consent was obtained from all participants.
Assessments
All patients were assessed by otoscopy, nasal endoscopy, and tympanometry at baseline. Otoscopy was used to determine the tympanic membrane position (normal or retracted). Nasal endoscopy was used to determine tubal torus mucosal status (normal or inflammatory). The ETDQ-7 questionnaire and ability of positive Valsalva maneuver were evaluated at baseline and 1 day in the ward, while at 2-, 4-, 12-, 24-, and 52-week follow-up via the telephone. 13 Perioperative blood pressure (systolic and diastolic blood pressure) and heart rate were recorded in both groups. Intraoperative systolic and diastolic blood pressure and heart rate were recorded when the balloon was maintained at a pressure of 10 bars in the lumen of the Eustachian tube. The patients were asked to complete questionnaires evaluating their experience and willingness regarding BDET procedures when they returned to the ward after the surgery. The effectiveness of BDET was defined as ETDQ-7 scores normalization (mean item score <2.1) and positive Valsalva maneuver ability.
Surgical Procedures
For BDET procedure under LA, nasal topical nerve block anesthesia was done as follows: put 3 to 5 small absorbent cotton pads with 1% lidocaine and 0.01% adrenaline into nasal cavity for 10 minutes. For Eustachian tube LA, 0.5 mL of lidocaine cream was applied to the Eustachian tube lumen via a balloon dilatation catheter and a 10-mL syringe under endoscopy for 10 minutes (Figure 1). For BDET procedure under GA, only 0.01% adrenaline was used topically as nasal decongestant. The induction to general endotracheal anesthesia was conducted by administration of fentanyl 2 mg/kg, propofol 2 mg/kg, and cisatracurium 2 mg/kg. Anesthesia was maintained with sevoflurane 1 MAC and remifentanil 0.1 to 0.2 μg/kg·min. The surgical technique for BDET has been described in detail in previous reports. 15,16 All BDET procedures were performed with the Bielefeld Dilation System (Spiggle & Theis GmbH). The balloon catheter was inserted into the Eustachian tube with endoscopic assistance (0°/30° view angle). The balloon (20 mm in length and 3.28 mm in diameter) was inflated with sterile water to a pressure of 10 bars and maintained for 2 minutes before deflating and removal. In the LA group, the duration of surgery included the time of anesthesia and the time of surgical procedure (BDET). In the GA group, the duration of surgery referred to the time of anesthesia (the time of surgical procedure was already included).
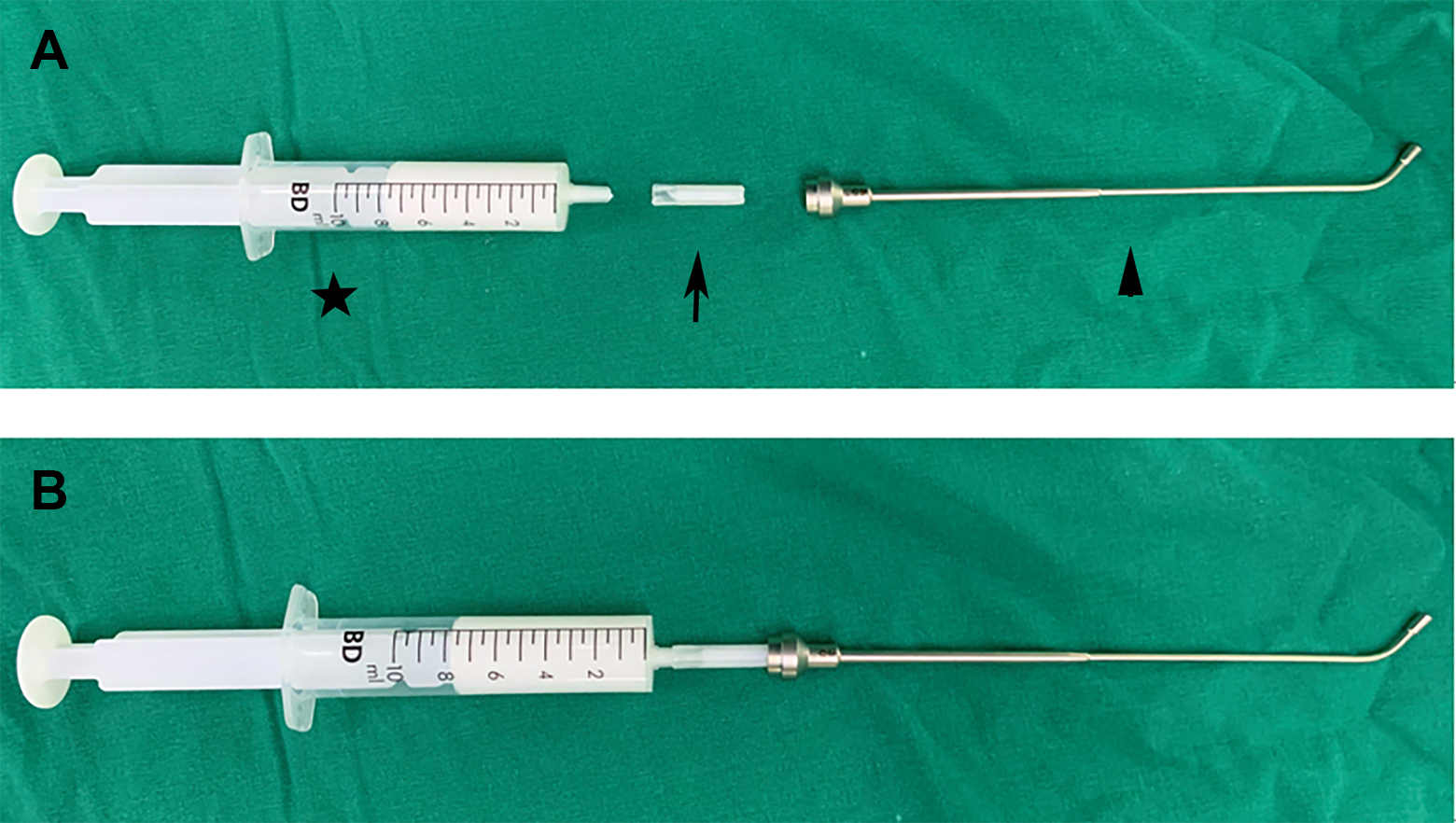
A, The instrument for Eustachian tube local anesthesia was consist of a 10-mL syringe (star), a 2-cm piece which was cut from a syringe tip cap (arrow) and the balloon dilatation catheter shaft (Spiggle & Theis GmbH; arrowhead). B, Instrument setup ready for Eustachian tube local anesthesia. The syringe is filled with lidocaine cream.
Statistical Analysis
The results were analyzed using SPSS 25.0. One-sided Student t test was used to compare symptom improvement between the LA group and the GA group with value of P < .025 considered statistically significant. Two-sided Student t tests and Wilcoxon rank-sum tests were used to compare other continuous measures; ×2 and Fisher exact tests were used to compare categorical measures. A P value of less than .05 was considered to be statistically significant.
Results
In total, 25 patients (32 ears) and 24 patients (32 ears) underwent BDET under LA and GA, respectively. Two patients (2 ears) in each group did not complete the 52-week follow-up evaluation because of not reaching the follow-up time point. Patient demographics and baseline characteristics are given in Table 1. There were no differences in demographics features, medical histories, and baseline characteristics except allergic rhinitis and chronic rhinitis between the LA and the GA groups. The procedural information is shown in Table 2. All BDET procedures in both groups were successfully carried out (64 successful dilations/64 attempts). The median duration of surgery was 39.4 minutes in the LA group, which was shorter than that in the GA group (95.0 minutes, P < .001). Similarly, the costs of surgery are significantly reduced in the LA group (1514.7 ± 451.6 RMB) compared with the GA group (3573.5 ± 56.5 RMB, P = .01).
Demographics and Baseline Characteristics.a
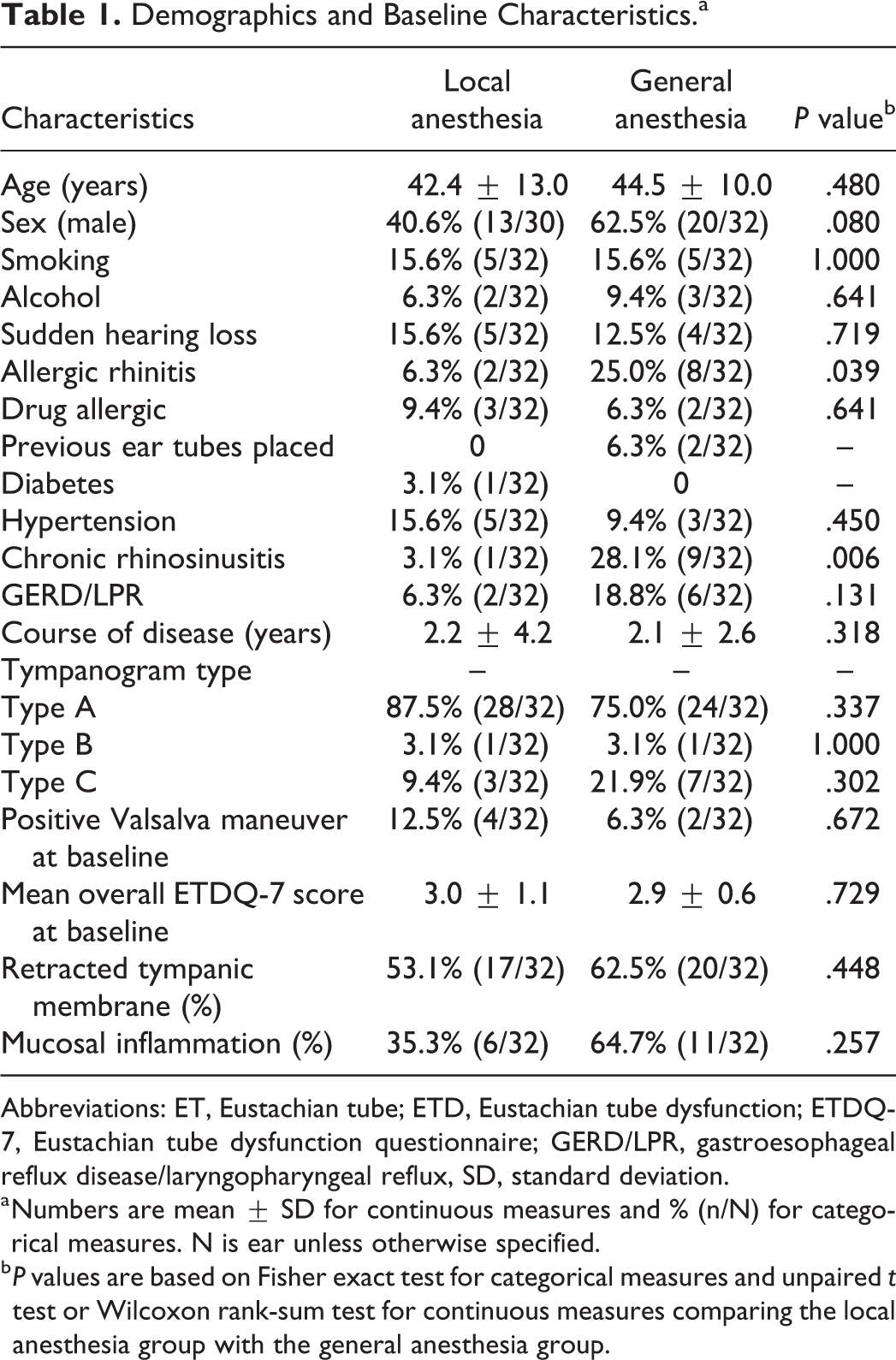
Abbreviations: ET, Eustachian tube; ETD, Eustachian tube dysfunction; ETDQ-7, Eustachian tube dysfunction questionnaire; GERD/LPR, gastroesophageal reflux disease/laryngopharyngeal reflux, SD, standard deviation.
a Numbers are mean ± SD for continuous measures and % (n/N) for categorical measures. N is ear unless otherwise specified.
b P values are based on Fisher exact test for categorical measures and unpaired t test or Wilcoxon rank-sum test for continuous measures comparing the local anesthesia group with the general anesthesia group.
Procedure Information for Participants Undergoing Balloon Dilation.a
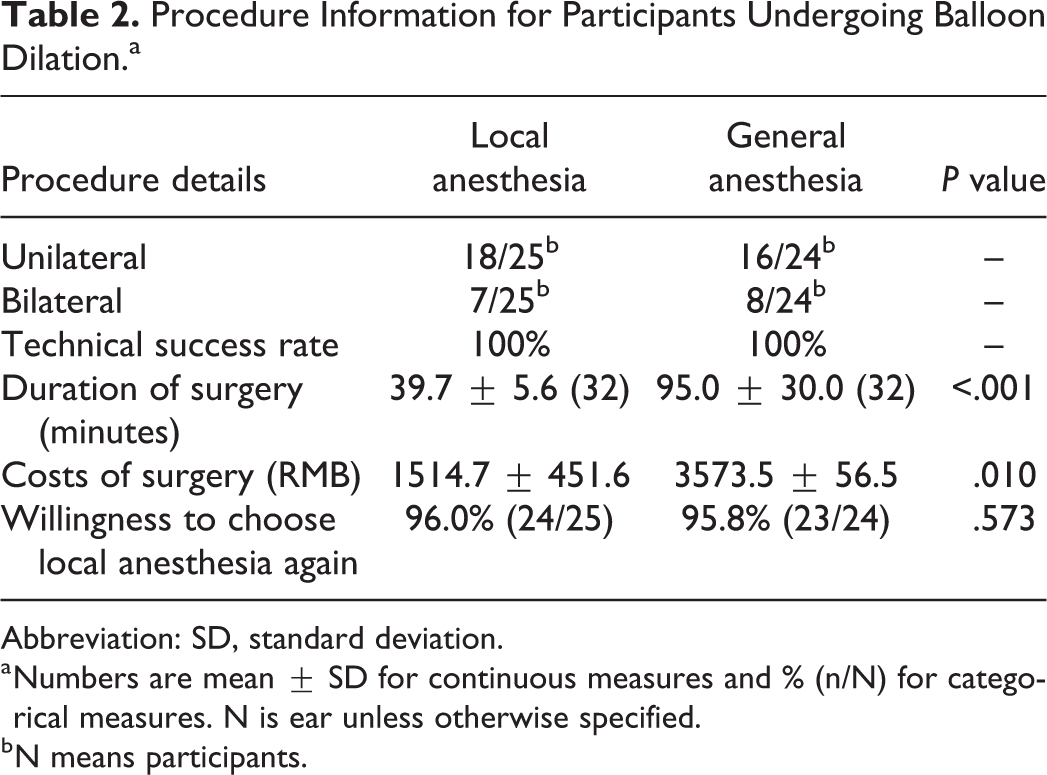
Abbreviation: SD, standard deviation.
a Numbers are mean ± SD for continuous measures and % (n/N) for categorical measures. N is ear unless otherwise specified.
b N means participants.
Intraoperative blood pressure and heart rate were monitored in all patients (Table 3). There were no significantly different in systolic blood pressure between 2 groups preoperatively (P = .141). Mean systolic blood pressure rose to approximately 137 mm Hg during BDET in the LA group, which is higher than that in the GA group (102 mm Hg, P < .001). Then, systolic blood pressure rapidly returned to baseline within 1 hour postoperatively in both groups. The similar change in diastolic blood pressure was observed during BDET procedure. Mean heart rate was 84 and 76 bpm in the LA and the GA group, respectively (P = .213). During BDET, mean heart rate increased to 92 bpm in the LA group, which was higher than that in the GA group (P = .01). Similarly, heart rate declined to baseline within 1 hour postoperatively in both groups.
Perioperative Blood Pressure and Heart Rate Between the 2 Groups.
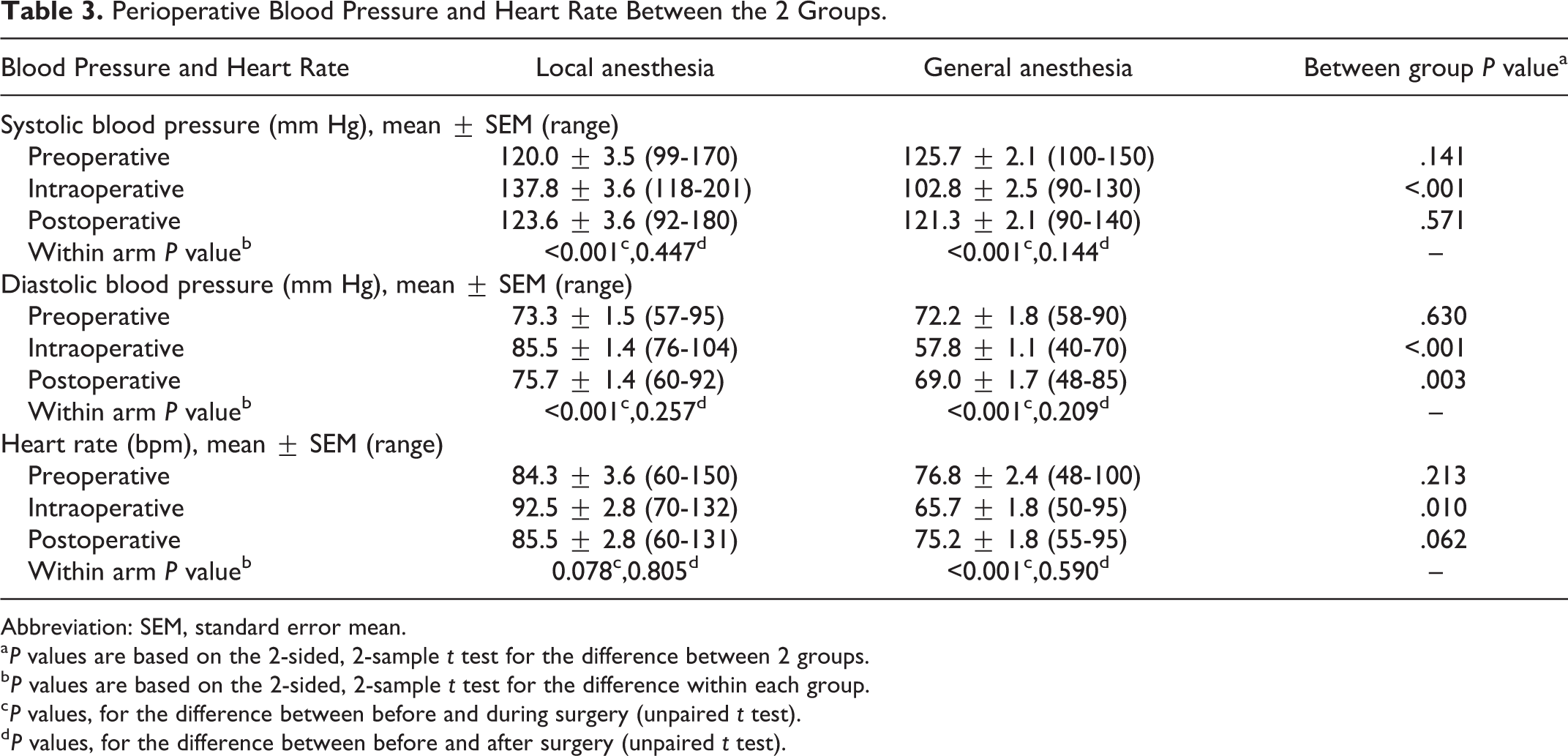
Abbreviation: SEM, standard error mean.
a P values are based on the 2-sided, 2-sample t test for the difference between 2 groups.
b P values are based on the 2-sided, 2-sample t test for the difference within each group.
c P values, for the difference between before and during surgery (unpaired t test).
d P values, for the difference between before and after surgery (unpaired t test).
After BDET procedures, the patients in the LA group were asked to evaluate the amount of pain they experienced during the procedure using the visual analog scale (VAS) of 0 to 10 (0, no pain; 10, worst possible pain). The VAS score for maximal pain was 5.4 ± 1.7 when inserting the balloon catheter into the lumen of the Eustachian tube and increased to 6.1 ± 1.0 when the balloon was being inflated with sterile water. The VAS score then slightly dropped to 4.9 ± 2.2 during maintenance of a pressure of 10 bar and returned to baseline (0.4 ± 0.8) 1 hour postoperatively (Table 4). Postoperative discomfort of patients in both groups is shown in Table 5. Sore throat was presented in 25% (6/24) of patients in the GA group, while no patients in the LA group complained of sore throat (P = .026). Fewer patients complained of fatigue, nasal obstruction, and runny nose in the LA group than the GA group, though there was no significant different. With regard to the willingness to choose the mode of anesthesia if BDET procedure was needed again, 96% (24/25) of patients in the LA group and 92% (23/25) of patients in the GA group would choose LA.
Pain During and After the Operation Under Local Anesthesia.a
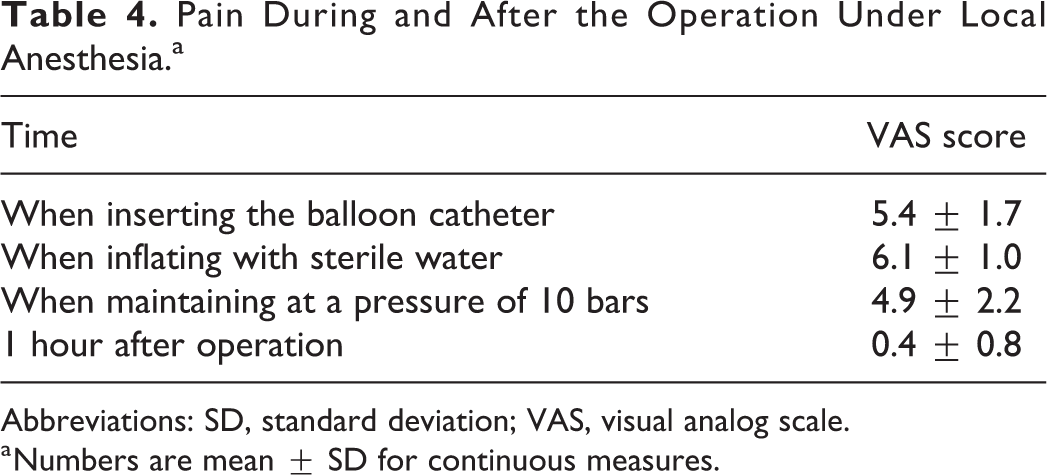
Abbreviations: SD, standard deviation; VAS, visual analog scale.
a Numbers are mean ± SD for continuous measures.
Discomfort After Surgery Between the 2 Groups.a
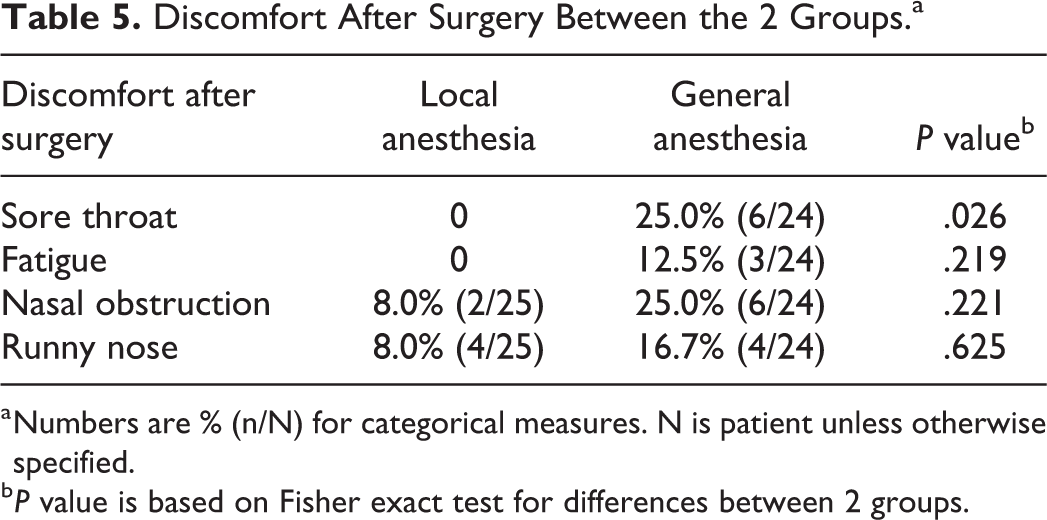
a Numbers are % (n/N) for categorical measures. N is patient unless otherwise specified.
b P value is based on Fisher exact test for differences between 2 groups.
The improvements in ETDQ-7 symptom score throughout follow-up are shown in Figures 2 and 3. Mean score of ETDQ-7 was 3.0 ± 1.1 and 2.9 ± 0.6 in the LA and GA group at baseline, respectively. Reduced ETDQ-7 score was presented in the majority of patients 1 day after surgery in both groups. The proportion of patients with normalization of ETDQ-7 scores was comparable between 2 groups at each follow-up time point except 1 day and 4-week follow-up. It is noteworthy that normalization of ETDQ-7 scores at 12-week follow-up was observed in 71.9% (23/32) of patients in the LA group and 81.3% (26/32) of patients in the GA group, respectively (P = .784). At 52-week follow-up, slightly more patients (80.0% [24/30]), though not significantly different, in the GA group showed normalization of ETDQ-7 scores in comparison with that in the LA group (63.3% [19/30], P = .126).
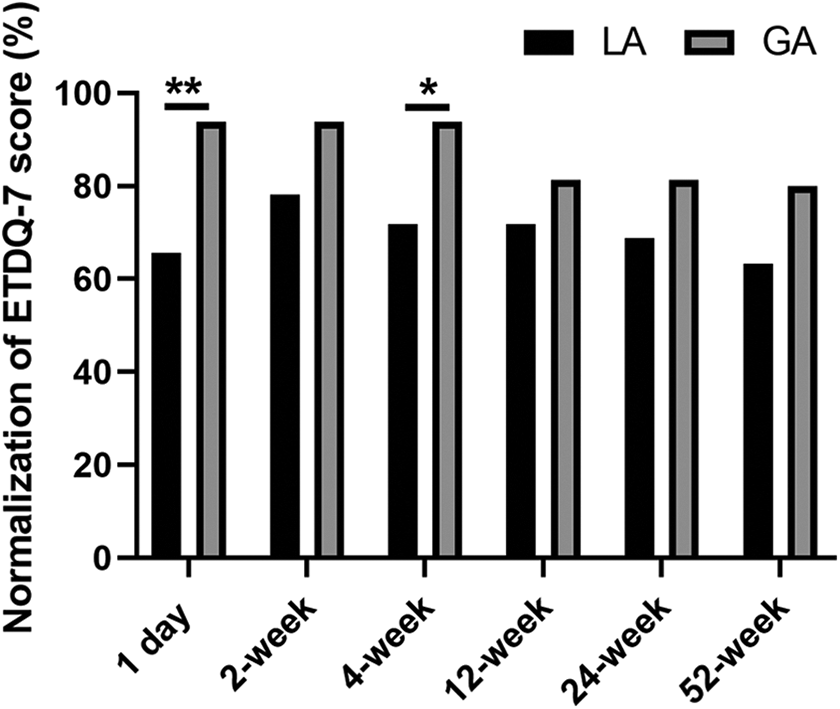
Normalization of mean EDTQ-7 score at 1 day, 2-, 4-, 12-, 24-, and 52-week follow-up in local anesthesia and general anesthesia groups. ETDQ-7 indicates 7-item Eustachian Tube Dysfunction Questionnaire. *P < .05, **P < .01. LA, local anesthesia; GA, general anesthesia.
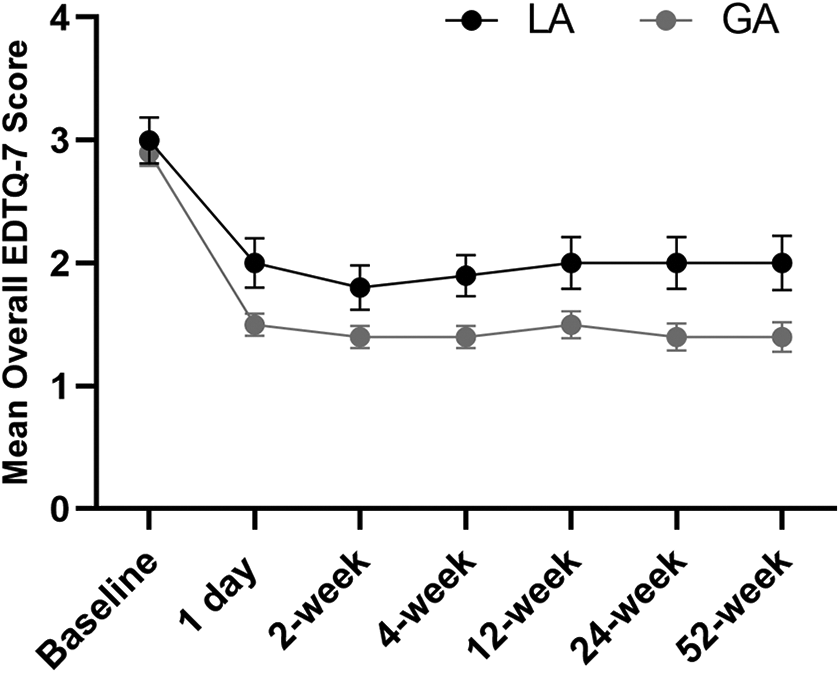
Mean overall ETDQ-7 scores at 1 day, 2-, 4-, 12-, 24-, and 52-week follow-up in local anesthesia and general anesthesia groups. ETDQ-7 indicates 7-item Eustachian Tube Dysfunction Questionnaire; GA, general anesthesia; LA, local anesthesia.
The ability of positive Valsalva maneuver was significantly improved after BDET in both groups throughout follow-up (Figure 4). To be noted, more patients reported a positive Valsalva maneuver in the GA group compared with the LA group at 12-week follow-up (93.8% [30/32] vs 65.6% [21/32], P = .011). At 52-week follow-up, the percentage of patients who could perform a positive Valsalva maneuver in the GA group increased to 100% (30/30), which was still higher than that in the LA group (80.0% [24/30], P = .024).
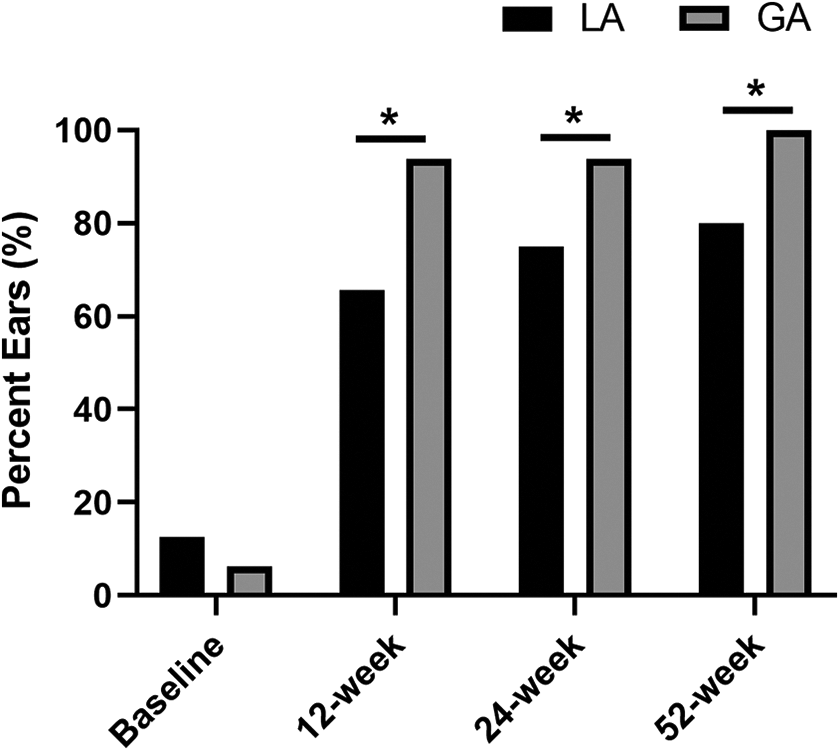
Change in positive Valsalva maneuver at baseline, 12-, 24-, and 52-week follow-up in local anesthesia and general anesthesia groups. *P < .05. GA, general anesthesia; LA, local anesthesia.
Discussion
Previous studies have indicated that BDET procedure could be performed safely with the AERA Dilation system and the Xpress Dilation System. 17,18 In the present study, we demonstrated for the first time that BDET under LA is also safe and feasible in a Chinese population with the Bielefeld Dilation System. Moreover, improvements in ETDQ-7 scores and positive Valsalva maneuver were sustained to 52-week follow-up and comparable between the LA group and the GA group, which are not described in previous studies.
The major concern of patients for BDET under LA is intraoperative pain. In the present study, 1% lidocaine and 0.01% adrenaline were used to nasal cavity, and lidocaine cream was applied to the Eustachian tube lumen for LA, which was similar to the methods described by Catalano and colleagues. 9 In Luukkainen and colleagues’ study, cocaine and adrenaline were used for nasal topical nerve block, while lidocaine–prilocaine cream for the Eustachian tube LA. 10 In addition, fentanyle, midazolam, and diazepam were also given for pain control during the surgery. Although the protocol for LA was a little different among these studies, the maximal pain experienced by the patients during BDET was similarly around 4 to 6, on a 1 to 10 VAS scale. Our results also revealed that patients experienced maximal pain when balloon was being inflated. Although experienced moderate pain during BDET procedure under LA, the majority of patients were satisfied with their pain control with the current LA protocol and would choose LA if the same procedure was needed again. Nevertheless, the efforts to improve LA method and further reduce intraoperative pain should be made in the future.
In the present study, blood pressure was monitored for the first time during BDET under LA. Our findings showed that both systolic blood pressure and diastolic blood pressure were dramatically increased during the surgery in the LA group perhaps due to pain and vagal reaction. The highest systolic blood pressure even reached above 200 mm Hg in one patient. Although such higher blood pressure only maintained for a short time (normally less than 5 minutes) and no adverse effects were detected in all patients postoperatively, we do not recommend performing BDET in patients with hypertension or at high risk for cardiovascular disease. We also strongly suggest that BDET under LA should be performed with electrocardiogram monitoring and intravenous line in place in case cerebrovascular accident occurs. In addition, increased heart rate was observed during BDET procedure under LA, which was not affected by BDET in Luukkainen and colleagues’ report. Because the number of patients in both studies was limited, the effect of BDET under LA on heart rate would be addressed with a large sample size in the further study.
Accumulating evidence has demonstrated the promising effects of BDET on OETD and symptom improvements could be maintained throughout 12-month follow-up. 7,11 In the present study, equally improvement in ETDQ-7 scores was observed throughout up to 52-week follow-up in the LA group and the GA group, which indicates that the effectiveness of BDET is not influenced by the mode of anesthesia. To be noted, the percentage of patients with normalization of ETDQ-7 scores appeared slightly lower in the LA group compared with the GA group at 12- and 52-week follow-up, although the difference did not reach statistical significance. Moreover, more patients reported the ability to perform a positive Valsalva maneuver in the GA group compared with the LA group at 12 week and 52 week. We speculated that cisatracurium as the muscle relaxant might affect the response of the surrounding muscles of the Eustachian tube to a pressure load induced by balloon dilation, which causes different outcomes between 2 groups. 19 Performing an animal experiment would test this hypothesis in the future.
The present study has some limitations. First, only one patient with a type B tympanogram in each group was included in the present study. Currently, it is customary to perform BDET in combination with tympanostomy tube placement for treatment with otitis media with effusion (OME) in China. Therefore, it is not possible to evaluate the effect of BDET alone in patients with a ventilation tube in the tympanic membrane. That is the reason why the majority of patients with OETD enrolled in the present study had a type A or type C tympanogram. Future research is needed to determine the effect of BDET under LA for patients with OME.
Furthermore, tympanogram was not recorded in most patients during follow-up in the present study. Our hospital is one of the biggest medical facilities in China, and the patients included in the present study were from various regions of China. Considering travel and time costs, most patients refused to return our hospital for follow-up, especially for those who have satisfactory outcomes. These patients were not willing to have additional examination because they were already free of symptoms. Exploring the effect of BDET under LA on tympanogram type transition needs further study.
Lastly, the relatively small numbers of patients in the LA group also limited the value of the present study. Therefore, we need to determine the effect of BDET under LA with a large sample size and a prospective randomized control trial in the future study.
Conclusion
Balloon dilation of the Eustachian tube under LA with the Bielefeld Dilation System is a safe and feasible procedure in a Chinese population. Surgical outcome is comparable between the LA group and the GA group during 52-week follow-up. The majority of patients would choose LA if the same procedure was needed again. Although performing BDET under LA remarkably reduced duration and costs of treatment compared with those under GA, more studies are required to investigate the management of intraoperative pain and longer follow-up outcome for BDET under LA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.