
Abstract
Background:
The sphenoethmoidal cell and the sphenoid sinus (SS) show great similarity in endoscopy and imaging. Hence, it is important to accurately identify the sphenoethmoidal cell preoperatively to prevent injury of the nerve and artery during endoscopic surgery. The aim of the present study was to investigate a special type of sphenoethmoidal cell.
Methods:
A total of 365 inpatients whose paranasal sinus computed tomography (CT) was collected and reviewed from May 2018 to September 2019 were included. The anatomical imaging characteristics of the sphenoethmoidal cell were observed.
Results:
A special type of the sphenoethmoidal cell was found on 9 sides in 730 sides (1.3%), according to its extension to the SS. Unlike Onodi cell (49.6%) and Jinfeng cell (1.3%), this cell simultaneously extends toward the superolateral, lateral, and inferolateral regions of the SS and is simultaneously closely attached to the optic canal and the maxillary nerve. Presently, this cell is named as the whole lateral type of the sphenoethmoidal cell, and the SS is located at the medial or inferomedial of it.
Conclusions:
When evaluating the paranasal sinus CT preoperatively, attention must be paid to the possibility of the whole lateral type of sphenoethmoidal cell appearing, not just Onodi cell, extending into the SS.
Keywords
Introduction
There is great variation in the extension of the ethmoid sinus (ES),1-4 which may be because the ES is considered part of the skull base bones and different from other sinuses. 5 The ES can extend toward the sphenoid sinus (SS), 4 the frontal sinuses, 6 and the maxillary sinus,2,3 which have also contributed to the difficulty of endoscopic sinus surgery (ESS).
In fact, the most posterior wall of the ES is the anterior wall of the SS.7,8 The SS and the posterior ethmoidal (PE) cell extend toward each other to the binding region of the SS and ES, with the SS expanding forward and forming the anterior recess of the SS. 7 The most PE cell can also expand toward the SS, which is defined as the sphenoethmoidal cell. 8 The Onodi cell is a well-known type of sphenoethmoidal cell which was first described by the Adolf Ónodi in 1903. 9 Accurate recognition of the Onodi cell before operation will help prevent injury to the optic nerve and the internal carotid artery during ESS. 9 Onodi cells have been more recently divided into different types according to their pneumatization depth toward the SS and their relation to the optic nerve canal.8,10,11 In addition, the anatomical definition of Onodi cell has been more clearly defined. The Onodi cell is limited to the most PE cell, which extends posteriorly to lie superolateral to the SS and, thus, in close proximity to the optic nerve and the internal carotid artery.8,9,11,12
However, the most PE cell is a group of cells usually composed of 1 or 2 cells based on the pneumatization of the basal lamella of the superior turbinate. 13 All the most PE cells have the opportunity to enter the SS. Based on our previous observations, the PE not only extends superolaterally with respect to the SS (Onodi cell) but also extends inferolaterally to the SS and forms an inferolateral sphenoethmoidal cell (ISEC or Jinfeng cell). 4 Furthermore, when the 2 most PE cells expand into the SS on the same side, the Onodi cell and ISEC, respectively, are formed by extending toward the superolateral and inferolateral regions of the SS. 4 Therefore, the sphenoethmoidal cell contains not only the Onodi cell but also the ISEC. To further elucidate the anatomical variation in sphenoethmoidal cells, we investigated the extension of the PE toward the SS. Another type of sphenoethmoidal cell was also identified which was defined as the whole lateral type of sphenoethmoidal cells.
It is very important to identify the anatomical variant of the sphenoethmoidal cells before ESS because the sphenoethmoidal cells have a close relationship with the optic nerve, the internal carotid artery, the cavernous sinus, the maxillary nerve (V2), the pituitary gland, and so on. It is sometimes difficult to accurately identify the sphenoethmoidal cell because of its large variations. 9 We still need to be aware that there are other types of variation, in addition to Onodi cells, that may occur individually or simultaneously.
Materials and Methods
Study Design
A retrospective analysis of paranasal sinus CT scans obtained from adult inpatients treated in our hospital from May 2018 to September 2019 was performed. The paranasal sinus CT scans of a total of 335 patients (670 sides) were reviewed and analyzed. The medical records of the patients were also reviewed, and the enrollment and exclusion criteria were consistent with our previous studies. 4 The research materials of this article include the data in our previous report. 4
Computed Tomography Examination and Analysis
The computed tomography (CT) scanning range spanned from the superior margin of the FS to the inferior margin of the maxillary alveolar process. A GE Lightspeed 64-slice spiral CT (GE Medical Systems, New York) system was used with a bone imaging algorithm. The CT scan acquisition and multiplanar reconstructions use the same strategy as in previous studies. 4 GE Centricity Enterprise Web 3 software (GE Medical Systems, New York) was used for viewing and measuring. Continuous observation was performed by sliding the computer mouse. Collection of the CT scans was approved by the ethics committee of Capital Medical University affiliated with Beijing Chaoyang Hospital. The study also conformed to the guidelines of the Helsinki Declaration.
Radiographic Anatomical Analysis
The radiological anatomic definition of the sphenoethmoidal cells
Currently, the expansion of the PE into the SS is termed the sphenoethmoidal cell. The optic nerve tubercle is considered the demarcation between the sphenoid and the ES. 12 The first evaluation of CT images was completed by L.J., and then the PE extending toward the SS (sphenoethmoidal cell) was confirmed by 2 otolaryngologists (L.J. and W.N.).
The superolateral type of sphenoethmoidal cell (Onodi cell)
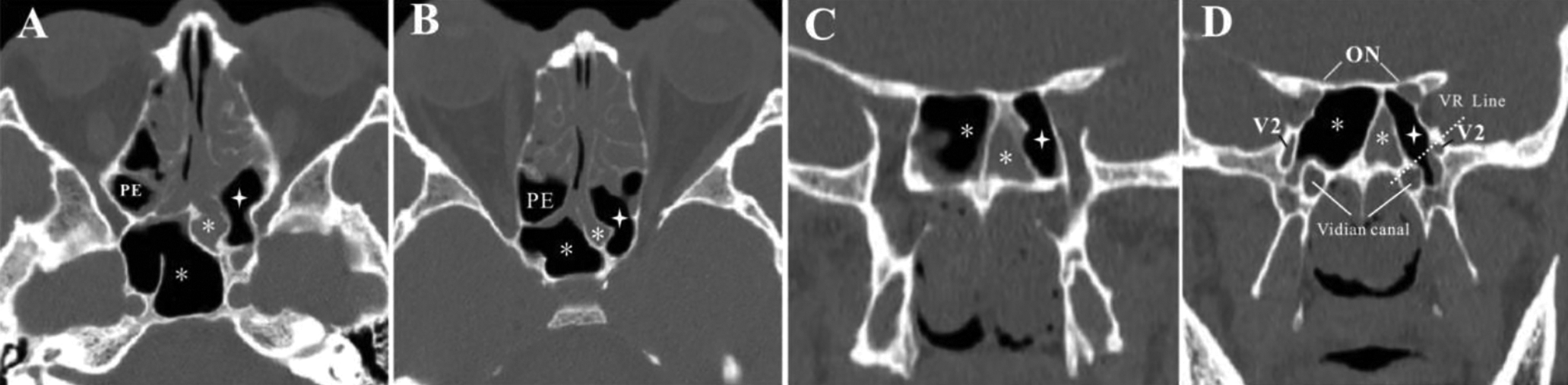
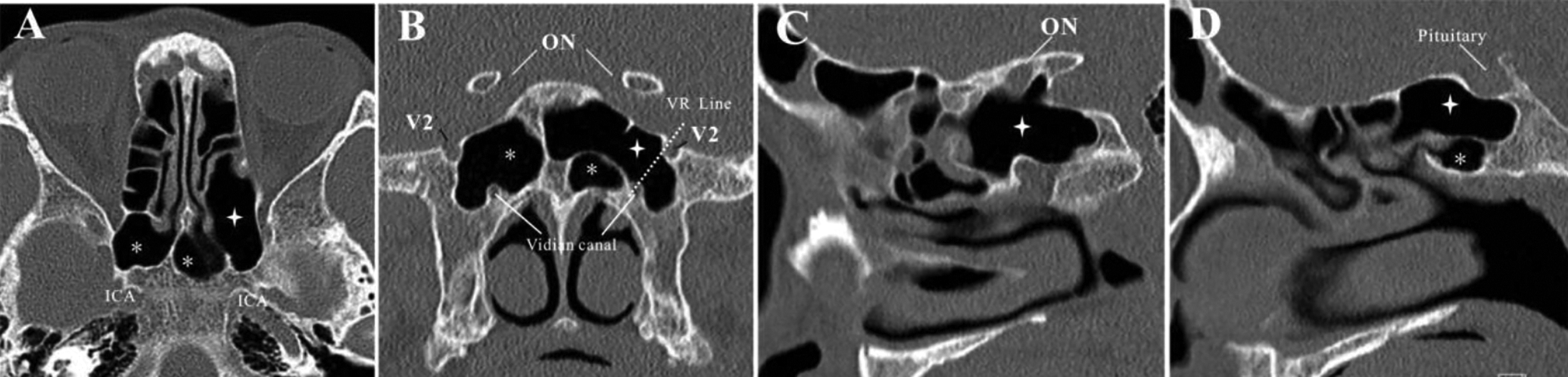
The Onodi cell is the most PE cell that pneumatizes superolateral, superior, or lateral to the SS and surrounds the optic canal (Figures 1–2),8,11,12 which was evaluated in all 3 planes (axial, coronal, and sagittal). 10 When the PE clings to the optic canal, it is confirmed to be an Onodi cell. The central Onodi cell is considered when the PE extends to the roof of the SS and clings to the optic canal of both sides (Figure 2).
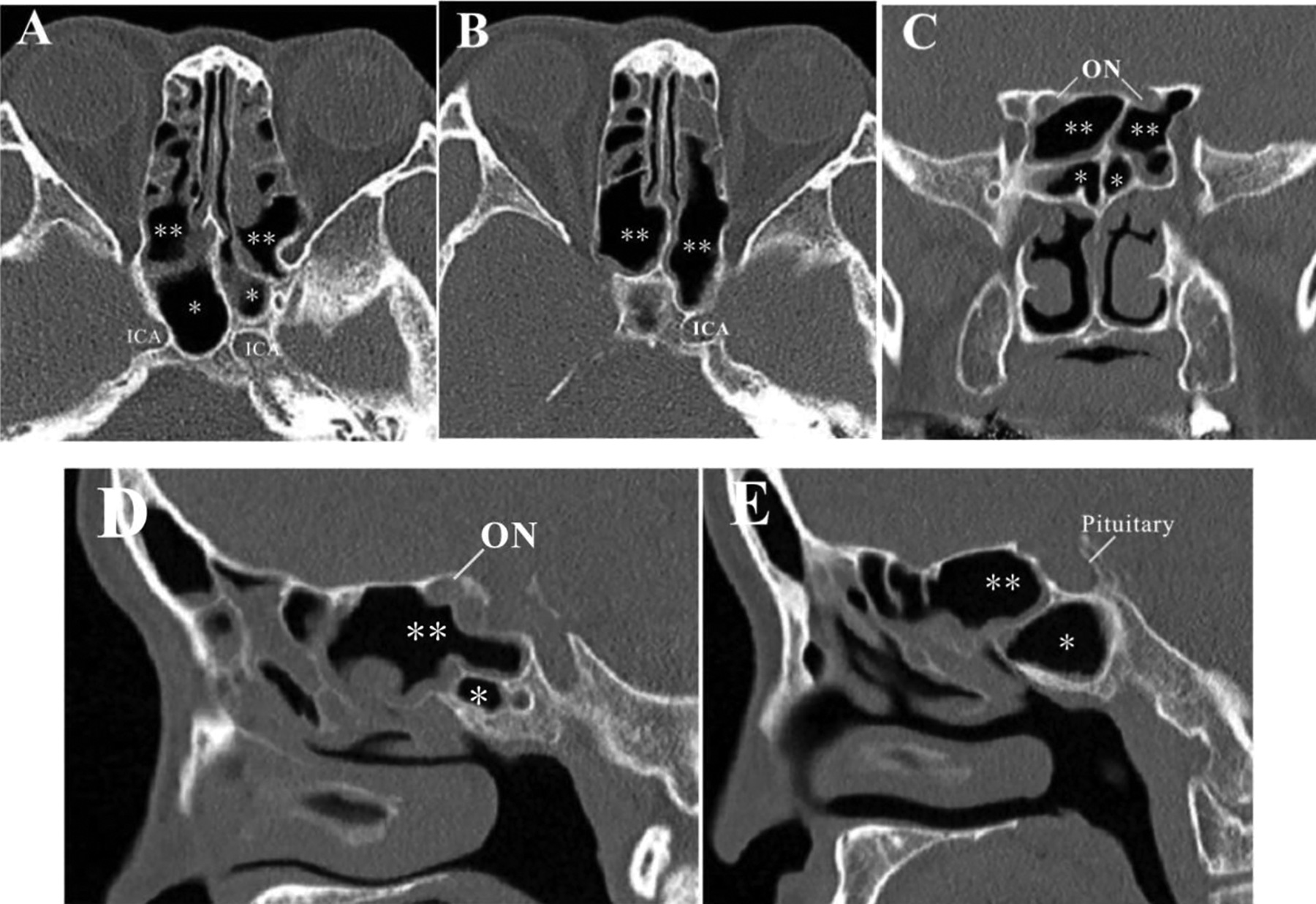
Axial, coronal and sagittal planes (from A to E) show that the superolateral type of sphenoethmoidal cells (Onodi cell **) on both sides was accompanied by the bilateral small sphenoid sinus (*). Figure C and D show that Onodi cell (**) located at the superior and lateral regions of the SS (*) and clings to the optic nerve (ON). Internal carotid artery (ICA).
Axial, coronal and sagittal planes (from A to C) show that excessive pneumatization of sphenoethmoidal cells (Onodi cell **) lies superior and midline to the SS (*). This Onodi cell is also described as the central Onodi cell (**), which clings to the optic cana of both sides (figure B). Figure B and C show that the bilateral SS (*) below the Onodi cell became smaller. Internal carotid artery (ICA). Optic nerve (ON). Maxillary nerve (V2).
The inferolateral type of sphenoethmoidal cell (ISEC or Jinfeng cell)
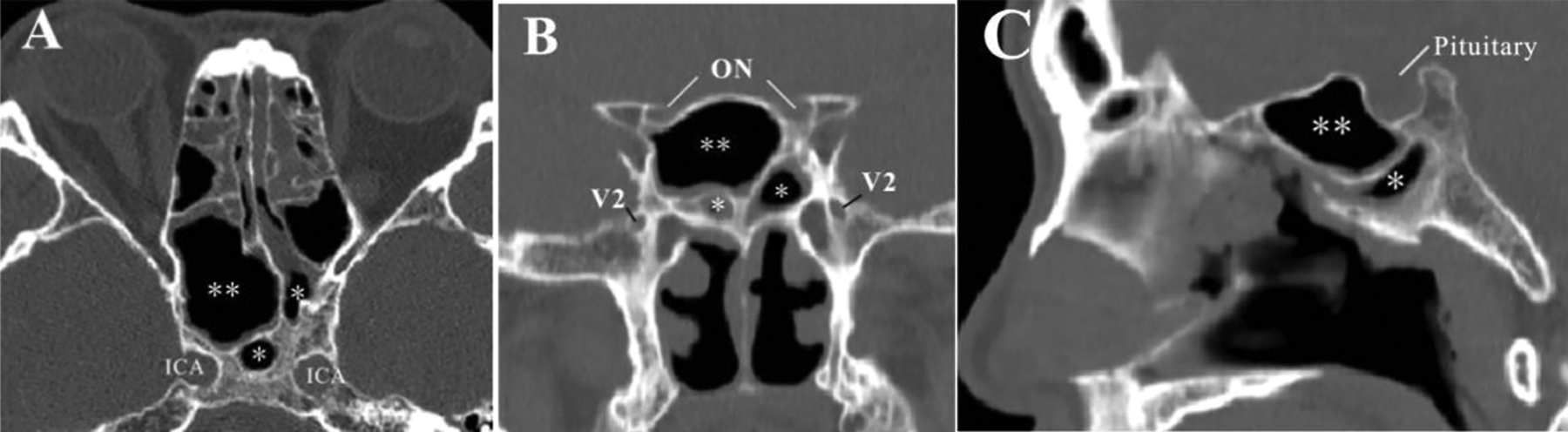
The ISEC was determined when PE pneumatization entering the lateral parts of the sphenoid bone, which drains directly into the most PE cell, was observed on the lateral side of the superior turbinate. The ISEC should also have a close relationship with the V2 (Figures 3 and 4). 4
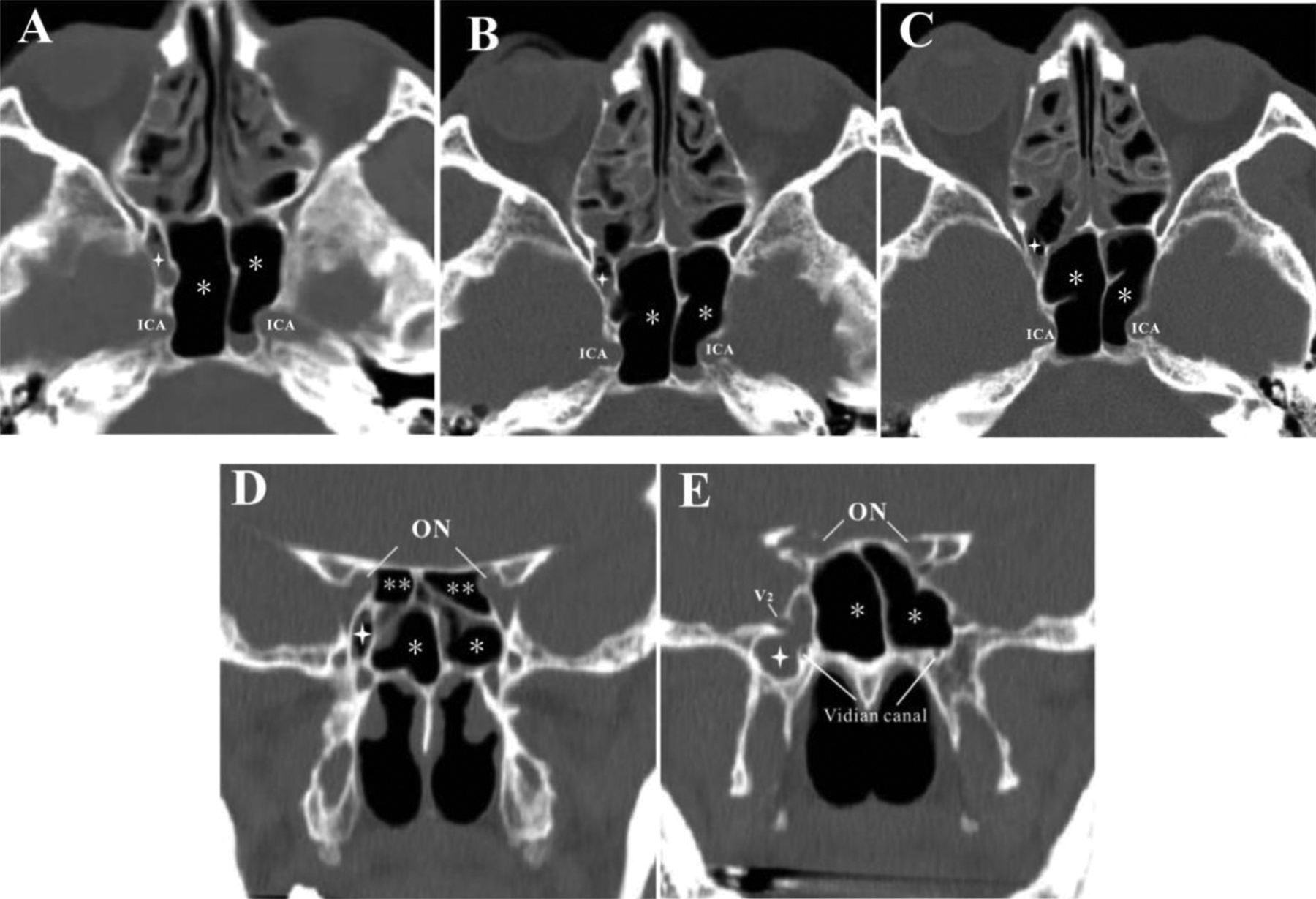
Axial and coronal planes (from A to E) show the inferolateral type of sphenoethmoidal cells (Jinfeng cell is indicated by the quadrangle star) appearing on the right side with chronic sinusitis (figure E). Jinfeng cell (indicated by the quadrangle star) located at the inferolateral of the SS (figure D and E) and drains directly into the most posterior ethmoid cell (figure C), which closely attached to the maxillary nerve (V2) and the vidian cana l (figure E). Onodi cell (**); SS (*). Internal carotid artery (ICA). Optic nerve (ON).
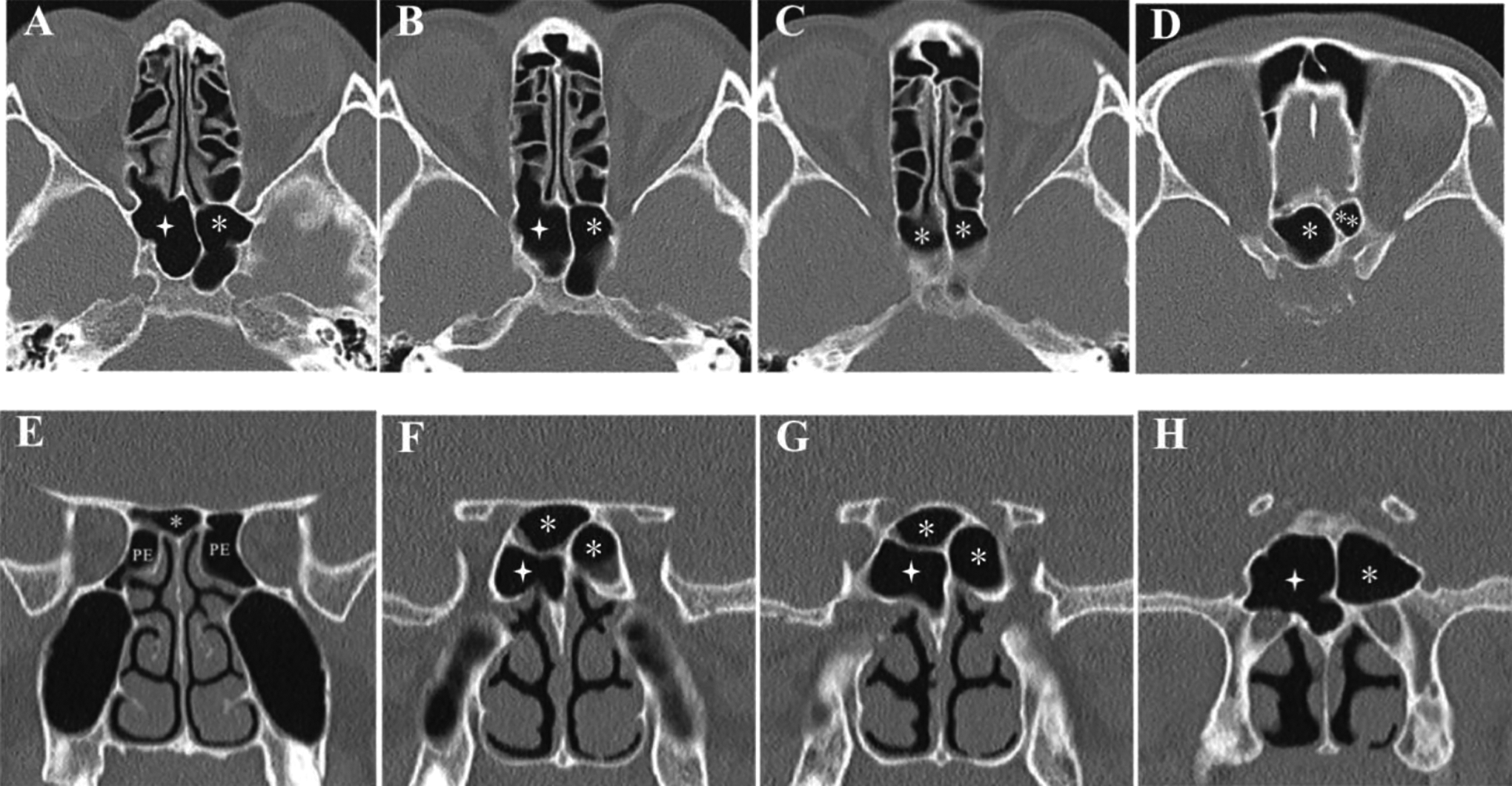
Axial CT scans of the bottom-up series (figure A-D) and a series of coronal CT scans from front to back (figure E-H) showing that the inferolateral type of sphenoethmoidal cells (Jinfeng cell is indicated by the quadrangle star) was the PE extends to the inferolateral of the SS (*), occupying most of the inferior and lateral parts of the right sphenoid body (figure F-H), while the right SS (*) is located above Jinfeng cell (quadrangle star). Onodi cell (**).
The whole lateral cell type of sphenoethmoidal cell
The whole lateral cell type of sphenoethmoidal cell is the most PE cell that simultaneously extends toward the superolateral, lateral, and inferolateral regions of the SS and is simultaneously closely attached to the optic canal and the maxillary nerve (Figures 5 and 7).
Statistical Analysis
Data regarding patient age are presented as the mean ± standard deviation. The descriptive statistics were determined using SPSS (version 23.0; SPSS, Inc, Chicago, Illinois). The incidence rates of the sphenoethmoidal cells in different types were calculated with preservation of 1 decimal place. The incidence difference among different types of sphenoethmoidal cells was calculated and evaluated by the χ2 test. Differences at the level of P < .05 were accepted to be statistically significant.
Results
The paranasal sinus CT images of 335 patients (670 sides) ranging in age from 18 to 73 years (mean, 42.96 ± 13.89 years) were reviewed and analyzed. Sphenoethmoidal cells were observed on 51.5% (345/670 sides) of the sides of 216 (64.4%; 216/335) patients. Furthermore, the sphenoethmoidal cells in 38.5% (129/335) of patients were bilateral, which was significantly higher than the percentage of unilateral sphenoethmoidal cells (26.0%; 87/335; P = .001). In patients with sphenoethmoidal cells appearing unilaterally, there was no difference between the left (42/87) and the right (45/87; P = .762).
The Whole Lateral Type of Sphenoethmoidal Cell
A special type of the sphenoethmoidal cell was found on 9 sides in 730 sides (1.3%), according to its extension to the SS, which is named as the whole lateral type of sphenoethmoidal cell. Unlike Onodi cell (49.6%) and Jinfeng cell (1.3%), the whole lateral type of sphenoethmoidal cell simultaneously extends toward the superolateral, lateral, and inferolateral regions of the SS and is simultaneously closely attached to the optic canal and the maxillary nerve (V2; Figures 5–7). The whole lateral type of sphenoethmoidal cell is well distinguished from Onodi cell and ISEC, according to its relation with the optic canal, the maxillary nerve, and the SS (Table 1). Onodi cell was the PE extending toward the lateral and superolateral region of the SS and surrounds or clings to the optic canal only on one side (Figure 1). The central Onodi cell was the PE extending into the infrasellar region, lying superior and midline to the SS and clinging to the optic canal on both sides (2.4%; 8/335), which is classified as Onodi cell (Figure 2). The ISEC was the PE extending toward the inferolateral region of the SS and may extend to the lateral part of the sphenoid bone, which clings to the V2 (Figures 3 and 4).
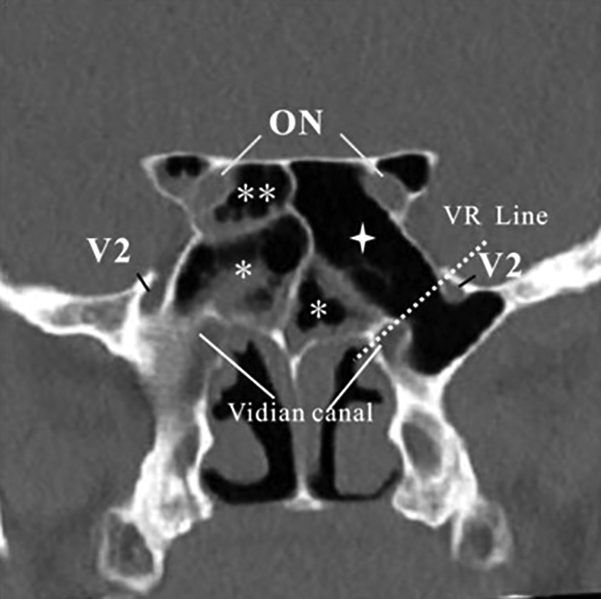
Axial (figure A and B) and coronal (figure C and D) planes showing the whole-lateral type of sphenoethmoidal cells (quadrangle star) appearing on the left side, which is also accompanied by chronic sphenoiditis on the left side (*). The SS(*) on the left became smaller (figure A-D). The whole-lateral type of sphenoethmoidal cells (quadrangle star) located at the lateral regions of the SS (*) and closely attached to the optic canal and the maxillary nerve (V2) simultaneously on left side (figure D). Optic nerve (ON). The VR line is the line connecting the vidian canal (V) and the foramen rotundum.
Axial (figure A), coronal (figure B) and sagittal (figure C and D) planes showing the whole-lateral type of sphenoethmoidal cells (quadrangle star) appearing on the left side and closely attached to the optic canal and the maxillary nerve (V2) simultaneously on left side (figure B and C). The SS (*) on the left side is squeezed and became smaller. Optic nerve (ON).
The superolateral type (Onodi cell**) and the whole lateral type (quadrangle star) of sphenoethmoidal cells appearing on the right side and the left side, respectively. Pneumatization of the anterior clinoid process appears on both sides.
Type of Sphenoethmoidal Cells and Its Incidence.
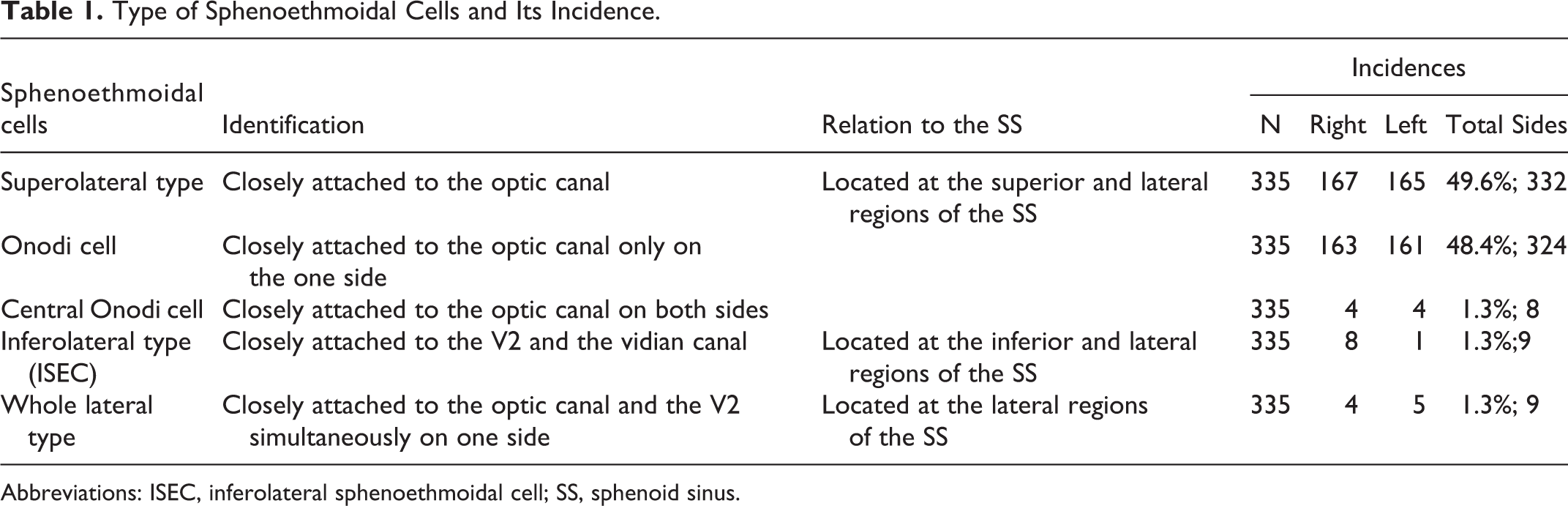
Abbreviations: ISEC, inferolateral sphenoethmoidal cell; SS, sphenoid sinus.
Three types of the sphenoethmoidal cells may occur individually (Figures 1, 2, 5 and 6). However, the Onodi cell and the ISEC can occur on the same side (Figure 3). The whole lateral type of sphenoethmoidal cells and Onodi cells can also occur in 1 patient (Figure 7). There were 5 patients with 2 sphenoethmoidal cells (Onodi and ISEC) that appeared simultaneously on the right side. Therefore, a total of 350 sphenoethmoidal cells were recorded. Among them, the superolateral type (Onodi cell and central Onodi cell) had the highest prevalence (49.6%; 332/670 cells), which was significantly higher than the inferolateral type (ISEC; 1.3%; 9/670 cells) and the whole lateral type (1.3%; 9/670 cells) (P < .05, respectively).
Relationship Between the Sphenoethmoidal Cells and the SS
The sphenoethmoidal cells are always located along the periphery of the body of the sphenoid bone and enter into it, even with excess pneumatization of the sphenoethmoidal cells (Figures 2 and 4). Regarding the position of the sphenoethmoidal cells relative to the SS, the sphenoethmoidal cells are located at the periphery of the SS. However, the position relationship varies according to the type of sphenoethmoidal cell. The SS is located inferior or inferomedial to the superolateral type (Figures 1 and 2), medial or superomedial to the inferolateral type (Figures 3 and 4), and medial or inferomedial to the whole lateral type (Figures 5 and 7).
Discussion
Identification of the anatomical variants of sphenoethmoidal cells is very important for ESS and endoscopic approaches of the sella and adjacent structures because of the proximity to important nerves and blood vessels.8,14 Therefore, the anatomical characteristics of sphenoethmoidal cells have been widely focused on and have been classified into different types according to the extension toward the sphenoid bone and its relationship with the optic nerve,8,10,11 which is helpful for avoiding neurovascular injury when the sphenoethmoidal cell and the SS are opened during ESS or when the sphenoethmoidal cell is amalgamated with the SS during endoscopic approaches of the sella and adjacent regions of the skull base. 14
However, the sphenoethmoidal cell itself can also have large variations, and it is sometimes not easy to accurately identify its rare variants, such as the ISEC (Jinfeng cell), 4 which is currently classified as an inferolateral type of sphenoethmoidal cell. When inflammation occurs alone in ISEC (Figure 3), if the ISEC is mistakenly thought to be the lateral recess of the SS during ESS, and only the SS is opened, the possibility of residual lesions will be increased. 4 Therefore, to accurately identify expansion of the PE into sphenoid bone based on paranasal sinus CT scans before operation, the sphenoethmoidal cells are divided into 3 types according to their extension characteristics (Table 1): the superolateral type (Onodi cell), the inferolateral type, and the whole-lateral type (Figures 1–7). Sphenoethmoidal cells can also extend into the infrasellar and lie superior and midline to the SS (Figure 2), which is termed a central Onodi cell 15 but is still currently classified as the superolateral type. However, we must emphasize that the opposite side of the central Onodi cell is not safe because the central Onodi cell clings to the optic canal of both sides.
All types of the sphenoethmoidal cells are formed by pneumatization of the most PE cell to the SS, which drains into the PE on the lateral side of the superior turbinate. Its drainage channel differs from that of the SS. Furthermore, there are also significant differences among different types of the sphenoethmoidal cells. Liu et al 4 have detailed the difference between ISEC and Onodi cell (Table 1). In addition, the simultaneous extension of PEs toward the superolateral and inferolateral regions of the SS on the same side forms the Onodi cell and the ISEC, respectively, which may be related to the number of most PE cells (Figure 3D). Kajiwara et al 13 reported that different types of pneumatization of the superior turbinate basal lamella may result in 1 or 2 of the most PE cells. However, even when Onodi and ISEC cells appear on the same side simultaneously, they also differ from the whole lateral type. Because the whole lateral type of the sphenoethmoidal cell is formed by the simultaneous extension of a single PE toward the superolateral, lateral, and inferolateral regions of the SS, there is no complete septum in it. The whole lateral type of sphenoethmoidal cells is an extreme variation, and this type can appear instead of the SS and be adjacent to important nerves, blood vessels, and the pituitary gland (Figures 5–7). Therefore, it is necessary to categorize the whole lateral type as an independent type.
Cohen et al 16 showed that the existence of Haller cells was significantly correlated with Kuhn and Onodi cells. Their results suggest that the extension of the ES is not only toward the SS but also toward the frontal sinuses 5 and the maxillary sinus. 3 In general, the extension of the PE toward the SS reflects that there exist significant pneumatization of the ES, implying that the internal motivating force of the ES pneumatization is higher than normal. However, there are significant differences in the prevalence of sphenoethmoidal cells among different types (Table 1). Onodi cell was the most common type (49.6%), which was significantly higher than that of the ISEC (1.3%) and the whole lateral type (1.3%; P < .05, respectively). The prevalent difference among the different types of sphenoethmoidal cells may be related to hindrance in the extension of the PE to the SS. The PE is often along the orbital apex and the optic canal into the superolateral part of the SS because the anterior wall of the SS is thinner and without obstacle. However, it is much more difficult for the PE to enter the inferolateral region of the SS, as it is difficult to bypass and cross the pterygopalatine fossa and pass through the root of the pterygoid process.
The sphenoid ostium has been considered to be one of the most constant and reliable landmarks for sphenoidotomy during ESS. 17 However, the appearance of sphenoethmoidal cells can make the SS smaller (Figures 1, 2, 4-7), which may lead to difficulty in finding the sphenoid ostium during ESS. Therefore, it may become difficult to open the sphenoidal sinus through sphenoid ostium approaches. 8 Because the PE always enters the SS along the periphery of the body of the sphenoid bone, this extending characteristic of the PE also reflects that sphenoethmoidal cells are always located at the periphery of the SS. The SS is then more medial and/or inferior than usual. 8 Under these circumstances, sphenoidotomy can be achieved by opening the sphenoethmoidal cells and then removing the bony septum between the SS and the sphenoethmoidal cells in an inward and downward direction according to the orientation of the septum.
Considering the similarity between a sphenoethmoidal (Onodi) cell and the SS endoscopically, Orlandi et al 18 described an anatomic relationship between the SS and the sphenoethmoidal (Onodi) cell. He demonstrated the surgeon’s ability to visualize the floors of the sphenoethmoidal (Onodi) cell but not the SS endoscopically, which is a reliable way to distinguish the sphenoethmoidal (Onodi) cell from the SS. However, based on the present observation, it is also difficult to endoscopically observe the floor of sphenoethmoidal cells of both the whole lateral type and ISEC, which are still not true SS. Therefore, the endoscopic method for distinguishing the SS from sphenoethmoidal cells, as described by Orlandi et al, 18 is only suitable for the Onodi cell. When evaluating the paranasal sinus CT before operation, attention must be paid to other possible PE types, not just Onodi cells, extending into the sphenoid bone.
Conclusion
Even if the incidence of the whole lateral types of sphenoethmoidal cell is very low, attention must be paid to it when evaluating the paranasal sinus CT preoperatively; otherwise, the whole lateral types of sphenoethmoidal cell may be mistaken for the SS, resulting in failed sphenoidotomy and putting the optic nerve and/or the internal carotid artery at risk during ESS or transsphenoidal approaches. In addition, the different types of sphenoethmoidal cells will lead to different position relationships between sphenoethmoidal cells and the SS. Therefore, the key to sphenoidotomy is to identify and confirm the orientation of the sphenoid ethmoidal septum before the operation. Sphenoidotomy can be achieved by removing the sphenoid ethmoidal septum downward and/or inward.
Footnotes
Authors’ Note
Jinfeng Liu discovered and identified this anatomical variation, analyzed the clinical significance of this variation, and wrote the article. Ningyu Wang and Jinfeng Liu reconfirmed this anatomical variation. Jingjing Yuan completed the data collection and analysis. Jinsheng Dai performed image editing. All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The CT scanning was approved by the Ethics Committee of Capital Medical University affiliated with Beijing Chaoyang Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Beijing Natural Science Foundation (7162066).