
Abstract
Objective:
The objective of this study was to determine the shape of cochlear basal turn through basic cochlear parameters measurement. The secondary aim was to overlay an image of the precurved electrode array on top of the three-dimensional (3D) image of the cochlea to determine which shape of the cochlear basal turn gives optimal electrode-to-modiolus proximity.
Materials and Methods:
Computed tomography (CT) preoperative image-data sets of 117 ears were made available for the measurements of cochlear parameters retrospectively. Three-dimensional slicer was used in the visualization and measurement of cochlear parameters from both 3D and 2D (2-dimensional) images of the inner ear. Cochlear parameters including basal turn diameter (A), width of the basal turn (B), and cochlear height (H) were measured from the appropriate planes. B/A ratio was made to investigate which ratios correspond to round and elliptical shape of the cochlear basal turn.
Results:
The cochlear size as measured by A value ranged between 7.4 mm and 10 mm. The B value and the cochlear height (H) showed a weak positive linear relation with A value. The ratio between the B and A values anything above or below 0.75 could be an indicator for a more round- or elliptical shaped cochlear basal turn, respectively. One sized/shaped commercially available precurved electrode array would not offer a tight electrode-to-modiolus in the cochlea that has an elliptical shaped basal turn as identified by the B/A ratio of <0.75.
Conclusion:
Accurate measurement of cochlear parameters adds value to the overall understanding of the cochlear geometry before a cochlear implantation procedure. The shape of cochlear basal turn could have clinical implications when comes to electrode-to-modiolus proximity.
Introduction
Cochlear implantation (CI) in recent times has reached a point that every fine geometrical detail of the inner ear has a role to play in the proper placement of the CI electrode array with a minimal degree of intracochlear trauma. Variations in the vertical trajectory of the cochlear duct from base to apex have been classified into rollercoaster, sloping, and intermediate as reported in detail by Avci et al. 1 The slope of the vertical trajectory of the cochlear duct has an influence on the course of electrode array and related damage to the basilar membrane or osseous spiral lamina where the slope decreases. 2 Rau et al 3 demonstrated through computer modeling how to optimize individually the insertion of one shaped preformed commercially available electrode array due to the overall variation in the size of the cochlea. Electrode-to-modiolus distance is one parameter that has been investigated in relation to Electrically Evoked Compound Action Potential, 4 current levels, 5 and battery consumption. 6 Scala Tympani is more spacious in the basal turn of the cochlea and as a result, the intracochlear position of the electrode could vary a lot influencing the auditory neural threshold level of the electrical stimulation. 7
The authors, to the best of their knowledge, are unaware of any prior studies that report specifically on the shape of the cochlear basal turn by measuring the cochlear parameters and its implications on the electrode-to-modiolus proximity with CI electrode array types. Therefore, the aim of this study was to determine the shape of the cochlear basal turn mainly by measuring the cochlear parameters A value basal turn diameter and B value which is perpendicular to the A value. The ratio between these 2 values could determine the shape of the cochlear basal turn. The secondary aim was to theoretically determine the ratio/shape of the cochlear basal turn that would give an optimal and suboptimal electrode-to-modiolus proximity with a precurved electrode array like the one that is commercially available. We hope that these findings could help the clinicians to an extent while choosing the best electrode type that fits to the cochlear needs of the patient.
Materials and Methods
Preoperative computed tomography (CT) images of temporal bones containing 117 ears within the Saudi population were made retrospectively available for the measurements of cochlear parameters. The CT images were loaded into a freeware 3-dimensional (3D) slicer (https://www.slicer.org/ version 4.8.0, Massachusetts) which is an advanced DICOM viewer. The inner ear in the oblique coronal plane (cochlear view as per Xu et al 8 ) was used in the measurement of A and B value from both sides of the ears. A value was measured by connecting the center of round window entrance passing through the mid-modiolus to the opposite side of the lateral wall as described by Escude et al. 9 The B value was measured by a line perpendicular to the A value and a line passing through the mid-modiolus. From the axial plane, the cochlear height H was measured from the floor of the basal turn to the roof of the apex along the mid-modiolar lines. Please refer to Figure 1 for the cochlear parameter measurement details.
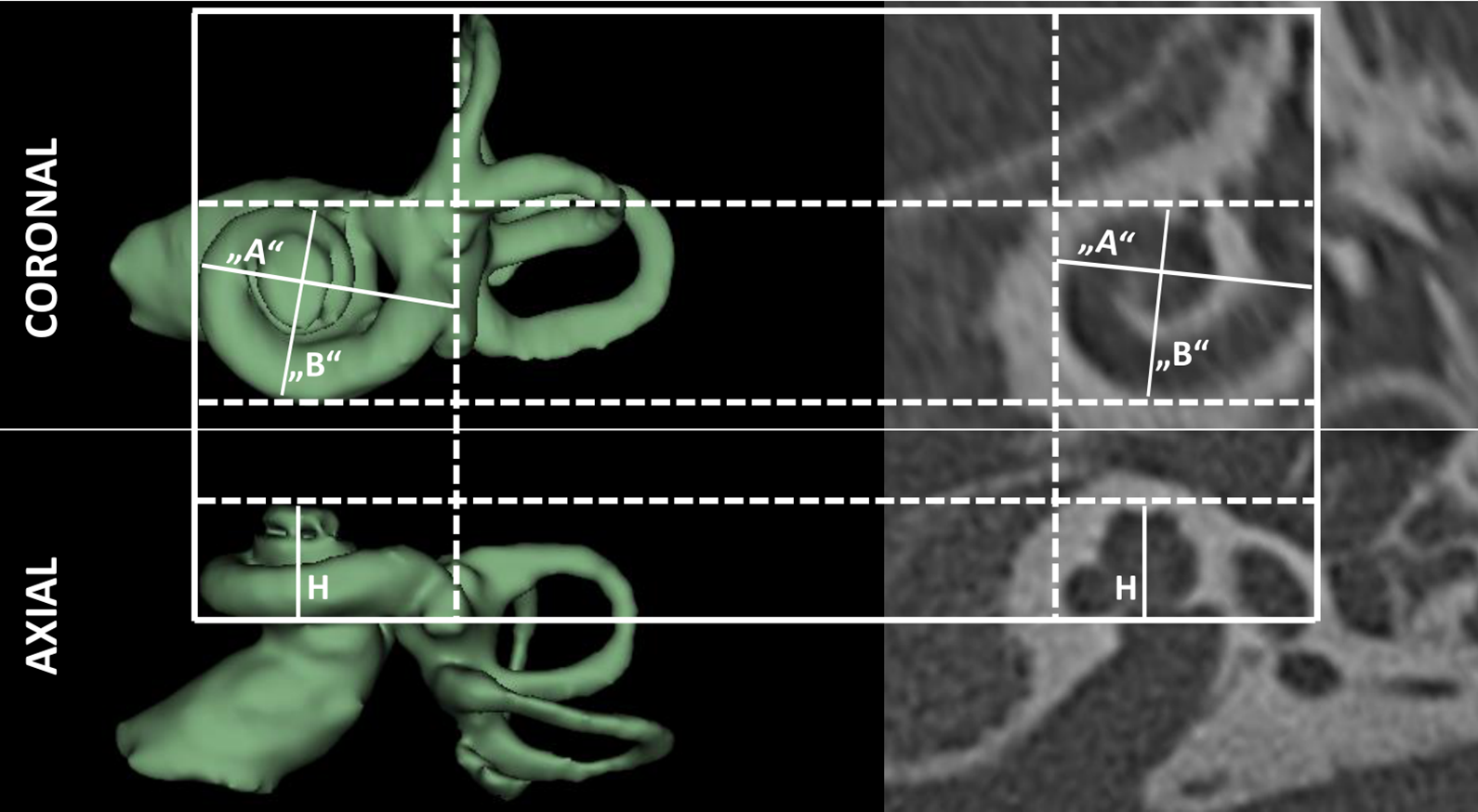
Normal anatomy inner ear in both coronal and axial view visualized using both 3D and 2D images in which cochlear parameters A, B and cochlear height (H) measurements are shown. 3D indicates three dimensional.
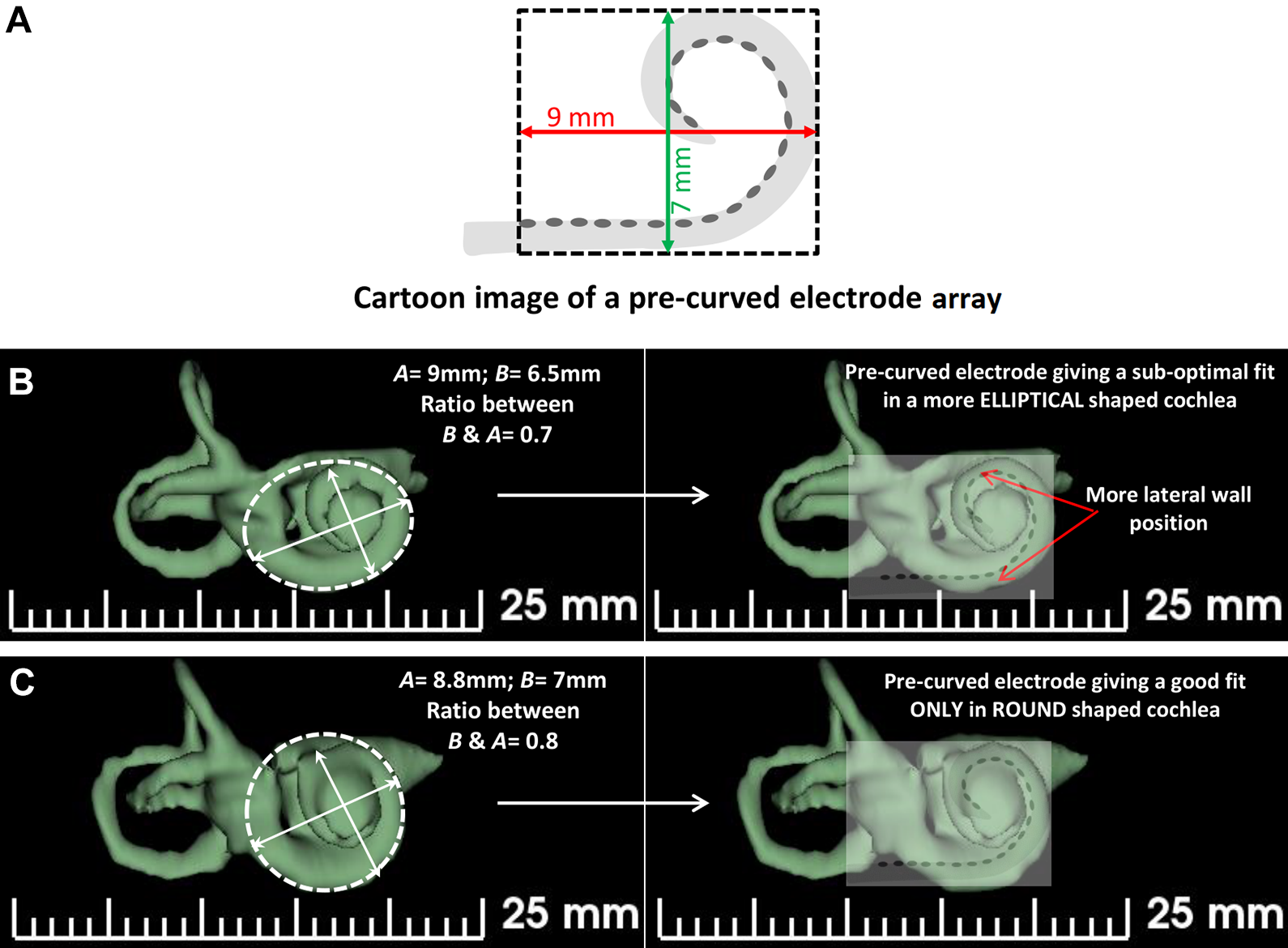
From the A value measure, cochlear duct length (CDL) along the organ of corti (OC) was estimated using the mathematical equation (CDLOC= [4.14 *A] − 4) derived by Alexiades et al 10 3D segmentation of the inner ear was made using the same 3D-slicer advanced DICOM viewer as described in Dhanasingh et al. 11,12 Geometrical shape of ellipse was drawn applying B and A values using Solid Works (www.solidworks.de; version 2017, Los Angeles) which is an advanced computer-aided design (CAD) software, followed by placing the resulting ellipse over the cochlear basal turn in its oblique coronal plane to determine the individual shape of the cochlear basal turn in all the 117 ears. Cartoon image of the precurved electrode was made by assuming their dimensions to be 9 mm in its long axis and 7 mm in its short axis as shown in Figure 2. This cartoon image of the electrode array was then laid over the 3D image of the cochlear basal turn to determine which cochlea would give an optimal and which one would give suboptimal electrode-to-modiolus proximity. B/A ratio was established to determine which ratio correspond to round-/elliptical-shaped cochlear basal turn. All the statistical analysis was done using Microsoft Excel 2010, Redmond, Washington.
Cartoon image of a precurved electrode array with its long axis length of 9 mm and short axis length of 7 mm (A). Three-dimensional images of an elliptical shaped cochlear basal turn with the cartoon image of the precurved electrode array on top of it. The B/A ratio is 0.7 and the prcurved electrode array shows lateral wall position in 2 locations intracochlear as pointed by red arrow marks (B). Three-dimensional image of a round shaped cochlear basal turn with B/A ratio of 0.8. A cartoon image of precurved electrode array over the cochlea showing a better electrode-to-modiolus proximity (C).
Results
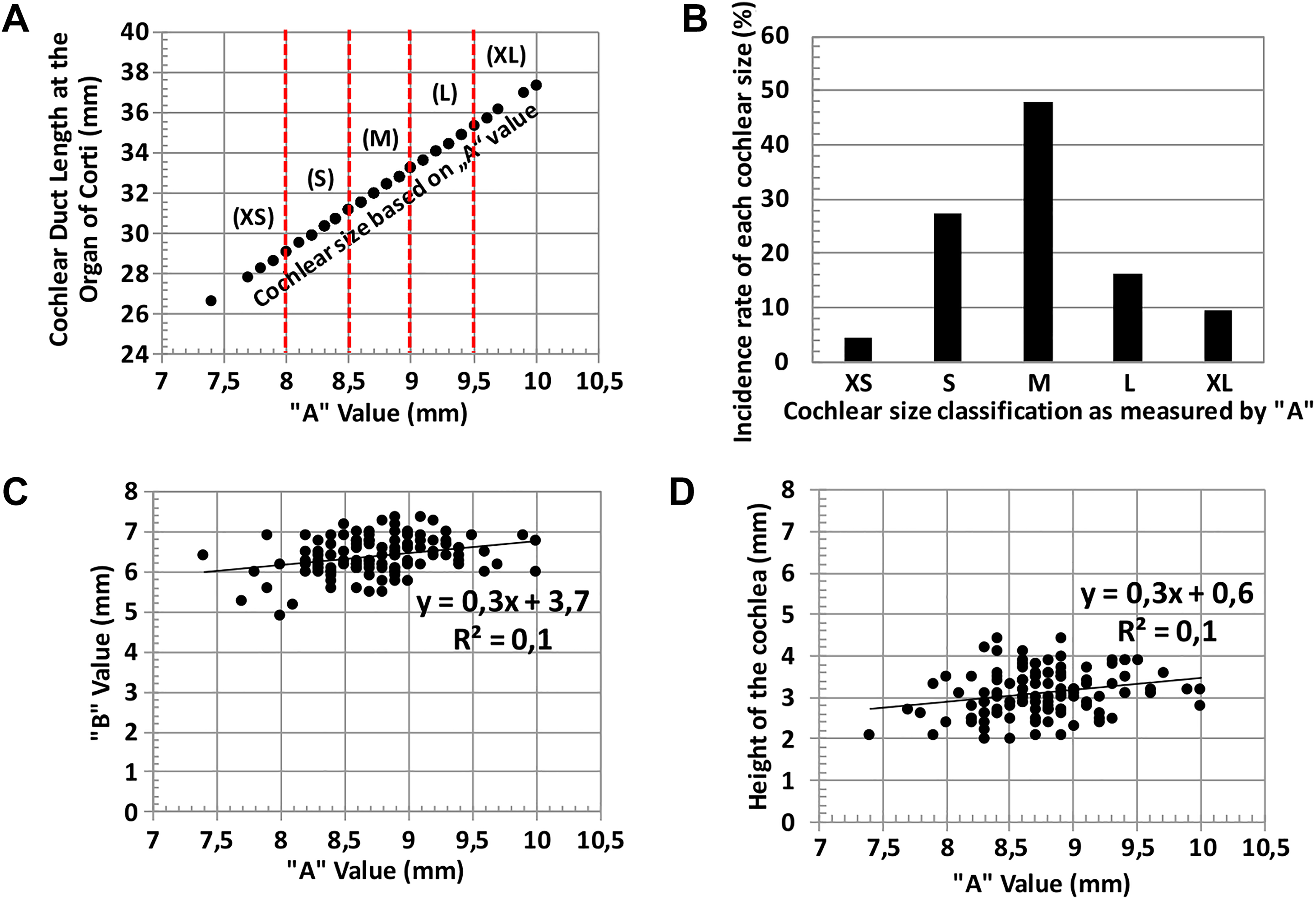
The cochlear parameters A, B, and the cochlear height (H) were measured from the CT images of 117 ears. The basal turn diameter A value ranged from a minimum of 7.4 mm to a maximum of 10 mm (Figure 3A). An attempt to classify the cochlear size based on the A value that differs by 0.5 mm was made. A value of anything less than 8 mm was named as extra small (XS) and it accounted for 4.3% of 117 ears taken in this study. A value anything between 8 and 8.5 mm was classified as small size cochlea (S) and it accounted for 27.3% of the total number of studied ears. Medium-sized (M) cochleae are considered with an A value between 8.6 and 9 mm and within this range, and there were 47.9% of the total number of ears. Large-sized (L) cochleae are the ones with A value between 9.1 mm and 9.5 mm and within this range, 16.2% of the studied ears were present. The extra-large (XL) sized cochleae was anything above 9.6 mm of the A values, and this was only 5.1% of the 117 ears considered in this study (Figure 3B).
Classification of cochlear size based on A value and the corresponding CDL OC using Alexiades equation. The vertical red dotted lines differentiate the cochlear size based on the A value (A). The incidence rate of each cochlear size is separately given in the form of histogram (B). A value plotted against the B value showing a weak positive relation (C). The A value plotted against the cochlear height H showed again a weak positive linear relation (D). CDL indicates cochlear duct length; OC, organ of corti.
The B value ranged from a minimum of 4.9 mm to a maximum of 7.6 mm. Between the A and the B value, a weak linear positive correlation with R 2 = 0.1 (Figure 3C) was observed. The height H of the cochlea again had a weak positive linear relation to the A value with R 2 = 0.1 and the value varied between 2 mm and 4.4 mm (Figure 3D). The corresponding CDL along the OC calculated using the Alexiades linear equation 10 ranged from a minimum of 26.6 mm to a maximum of 37.4 mm.
To determine which shaped cochlear basal turn would offer an optimal and suboptimal electrode-to-modiolus proximity with precurved electrode array considered in this study, a cartoon image of a precurved electrode array (Figure 2A) with long axis and short axis dimensions of 9 mm and 7 mm, respectively (authors take no responsibility if these dimensions match coincidentally with commercially available Contour Advance electrode array) was overlaid on the 3D images of all the 117 cochleae in its oblique coronal plane as shown in Figure 2B and C and eye-balled to see the physical fit. The result may be highly subjective but agreed with all the authors. For an elliptical-shaped cochlear basal turn with the B/A ratio of 0.7, the precurved electrode array which is similar in size and shape to the commercially available one is expected to give suboptimal electrode-to-modiolus proximity inside the cochlea with the electrode array being more lateral wall positioned as shown in Figure 2B. For a more round-shaped cochlear basal turn with the B/A ratio of 0.8, the precurved electrode array would give a tight electrode-to-modiolus proximity (Figure 2C). Geometrical shape ellipse was constructed using the CAD software applying the B and the A values of 117 cochleae to get an understanding of the exact shape of each of the cochleae (Figure 4B). The B/A ratio of 1 would be a perfect circle and anything <1 would be an out of shape circle. The B/A ratio of 0.75 was taken as the cutoff value by the authors based on Figure 2 trials and anything above and below the cutoff value would differentiate a more rounded-shaped cochlear basal turn from a more elliptical-shaped cochlear basal turn, respectively.
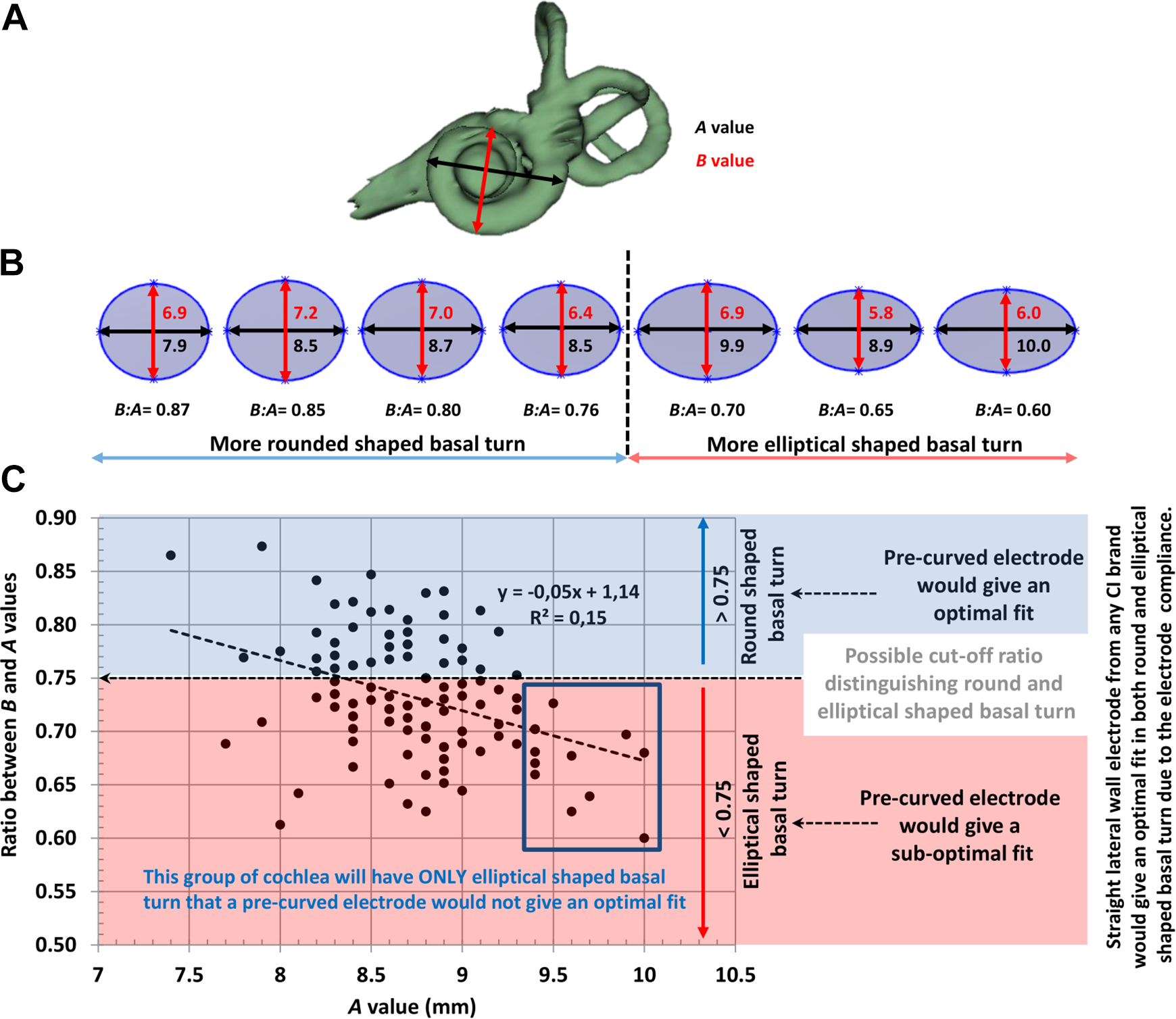
Oblique coronal view of cochlea with the A and the B value description (A). CAD models of various size/shape of ellipse for a wide range of B/A ratios (B). Plot between A and the B/A ratio showing a weak negative linear relation. Ratio of < 0.75 or > 0.75 would be considered an elliptical shaped and round shaped cochlear basal turn respectively (C). CAD indicates computer-aided design.
Plot between A value and the B/A ratio showed a weak negative linear relationship with an R 2 = 0.15 (Figure 4C). For the A values between 9.4 and 10 mm (Figure 4C red-boxed area), all the samples would have a more elliptical shaped cochlear basal turn in which the precurved electrode array would give only a suboptimal electrode-to-modiolus proximity.
Discussion
Recently, Zahara et al 13 and Grover et al 14 reported on the cochlear size variation by measuring both A value and B value within the Indian and Indonesian population, respectively. Alanazi and Alzhrani 15 reported on the cochlear size variation between Saudi and non-Saudi populations just by measuring the A value. Iyaniwura et al 16 reported on automated A value measurement tool in the accurate estimation of CDL and nothing about the B value was mentioned. Schurzig et al 17 reported a more accurate estimation of CDL by measuring both the A and the B values. The rationale for including B value as well in their report in CDL estimation is to accommodate to the variation seen in B values. However, they did not investigate the ratio between B and A values that would determine the shape of the basal turn of the cochlea as given in our study. Kuthubutheen et al 18 reported on the effect of cochlear size on the CI outcomes, in which they measured the A value in estimating the cochlear size. Takahashi et al 19 reported on cochlear volume as a predictive factor in residual hearing preservation in which they measured the A value was considered in the estimation of the CDL. Deep et al 20 reported, measuring A value is consistent from preoperative CT imaging and recommended utilizing it in the CDL estimation prior to CI surgery. Liu et al 21 reported interesting data on the measurements of cochlear parameters including A, B and the cochlear height (H) for several anatomical variation types of cochlea, but there was no report on the ratio between B and the A value as reported in this current study. Escude et al 9 derived a mathematical equation in estimating the CDL using A value and the insertion angle as the input. He as well reported on the B value and correlated it with A value with a better R 2 = 0.57 which is higher than the R 2 = 0.1 reported in this current study.
To the best of our knowledge, this is the first study that reports the ratio between B and A values in predicting the shape of the cochlear basal turn. It was the author’s self-classification that B/A ratio > 0.75 would refer to a more rounded shaped cochlear basal turn and the B/A ratio < 0.75 would correspond to more elliptical shaped cochlear basal turn. This conclusion was made from the observation of manually placing the cartoon image of precurved electrode array over the 3D image of the cochlea in its oblique coronal plane. Shape of cochlear basal turn has a direct clinical implication on the electrode-to-modiolus proximity inside the cochlea. Our theoretical findings revealed that a single sized/shaped precurved electrode array would give a more lateral wall position in a more elliptical shaped cochlear basal turn compared to round shaped cochlear basal turn. The other novel finding in our study is the classification of the cochlear size in-terms of XS, S, M, L, and XL based on the A value that differed by 0.5 mm which is clinically relevant in choosing the CI electrode array length and type irrespective of CI brands. “M” sized cochlea with a higher incidence rate of 47.9% is worth taking a closer look compared to the other cochlear sizes as this may be the rational for making the precurved electrode array in one size and shape. But this leaves the other sized cochleae to have a clear mismatch with one sized/shaped precurved electrode array. Between A value and other parameters including B and H, we did see a weak positive relationship with R 2 = 0.1, and this implies that the cochlea does grow in all directions, however, not proportionally. This makes it important to measure most of the cochlea parameters and not just limited with the A value when comes to cochlear size measurement followed by electrode array length/type selection.
One sized/shaped precurved modiolar hugging electrode might have difficulty in providing a tight modiolar hugging position consistently in every cochlea that varies hugely in its size, shape, and anatomy. Our conclusion is well supported by the clinical findings of Wang et al 22 that a precurved modiolar hugging electrode array, in particular, the Contour Advance electrode more often than not do not sit adjacent to the modiolar wall. The straight lateral wall electrode array type for an array length that goes beyond the basal turn, shape of the basal turn could influence the electrode array insertion behavior which was not studied prospectively yet. The major limitation of this study is that we did not clinically investigate the postoperative CT images implanted with precurved electrode type. This could well be a proposal for future studies where both preoperative CT images can help with an accurate determination of the shape of cochlear basal turn and postoperative CT images to find the electrode-to-modiolus proximity.
Conclusion
In conclusion, the classification of cochlear size in terms of XS, S, M, L, and XL based on A value is a new finding. The B/A ratio is a helpful measure in the identification of shape of cochlear basal turn. This could have a clinical implication on the electrode-to-modiolus proximity especially with one sized/shaped precurved electrode array type.
Footnotes
Acknowledgments
Radiology department of King Abdul Aziz University Hospital, King Saud University, is kindly acknowledged for their kind support throughout this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The second author is employed by MED-EL GmbH, Austria as the Head of Translational Science Communication, a role which is purely scientific with no marketing activities.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.