
Abstract
Foreign bodies in the ear are relatively common in emergency medicine. However, attempts at removal made outside the healthcare setting by untrained persons can result in complications of varying degrees. We conducted a 3-year retrospective review of 123 cases of aural foreign bodies at our hospital in Nigeria. Our patient population was made up of 80 males and 43 females, aged 2 to 67 years (mean: 13.2); almost three-fourths of these patients were aged 15 years or younger. Only 40 of them (32.5%) presented to an otolaryngologist within 12 hours of foreign-body insertion. A total of 30 patients (24.4%) had initially undergone removal attempts by a non-otolaryngologist prior to receiving trained ENT care, and 23 of them experienced a total of 41 complications: 17 cases of canal abrasion, laceration, and/or bleeding, 8 cases of otitis externa, 6 cases of tympanic membrane perforation, 5 cases of impaired hearing, 3 cases of chronic suppurative otitis media, and 2 cases of middle ear involvement. Of the 93 patients who were seen by an otolaryngologist initially, only 6 (6.5%) developed a complication: 4 cases of canal abrasion, laceration, and/or bleeding and 2 cases of otitis externa. The difference in overall complication rates between patients treated by otolaryngologists and non-otolaryngologists was statistically significant (p < 0.001). We conclude that attempts at removal by non-otolaryngologists can result in a high incidence of preventable complications.
Introduction
Insertion of a foreign body into the ear is a common occurrence worldwide, and it is seen most often, but not exclusively, in children. 1 –6 Mentally ill adults are also known to insert a foreign body in their ears. 7,8 A wide variety of objects are inserted into the ears; the specific types of object generally vary according to the patient’s age. 9 Commonly reported substances include stones, paper, beads, pencil erasers, cotton buds (e.g., Q-tips), insects, seeds, matchsticks, and many others. 6,10
The earliest presentation of an aural foreign body generally occurs around the age of 9 months, when children develop a pincer grip and become able to manipulate small objects. 8 When a caregiver suspects that a child has sustained an aural foreign-body impaction, the caregiver should not scold or threaten the child because the child may deny it to avoid punishment. Obviously, denial can result in a delay in discovery and increase the risk of complications. 5 In adults, impaction can result from a desire to clean or scratch the ear canal. 11
Most cases of a foreign body in the ear are not serious. The urgency of any particular situation depends primarily on the nature of the substance and its precise location. The keys to successful removal are adequate vision, appropriate equipment, a cooperative patient, and a skilled physician. 12
We conducted a study to review the clinical spectrum and profile of foreign bodies in the ear as seen in our medical facility in southwestern Nigeria. Our focus was on the complications associated with a delay in presentation and the consequences of attempted removal by untrained persons.
Patients and Methods
We retrospectively reviewed the records of all patients with a foreign body in the ear who had presented to the Federal Medical Centre in Ido Ekiti, Nigeria, from January 2005 through December 2007. Our hospital is a tertiary care institution located in a suburban setting in southwest Nigeria. Records were obtained from the emergency department, the ENT clinic, and the surgery department.
In addition to demographic data, we compiled information on the type of foreign body, the affected side, the interval between onset and presentation, the presenting signs and symptoms, treatment, any previous attempts at removal by a non-otolaryngologist, and complications.
We identified 136 cases in all. Of these, 13 were excluded because of incomplete data, leaving us with 123 evaluable cases. For analysis, patients were assigned to various age groups broken into 5-year increments up through age 30; all those older than 30 years were classified as a single, separate group.
Data were tabulated and statistically analyzed with the Statistical Package for the Social Sciences software (SPSS v. 15; Chicago). A p value of less than 0.05 was considered statistically significant.
Results
Demographic Data
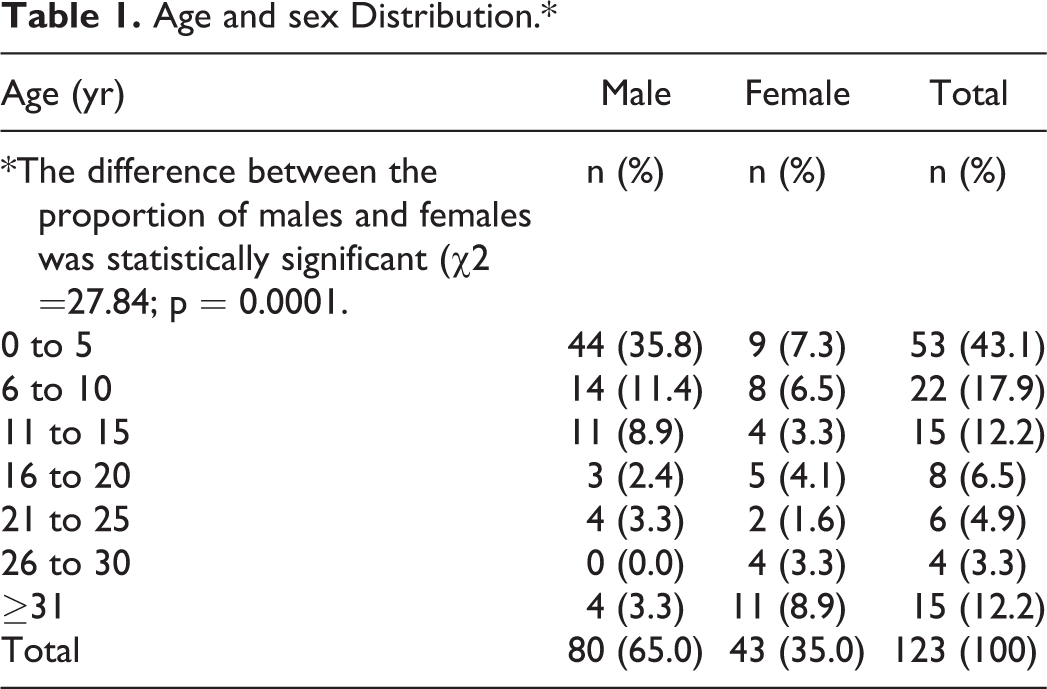
The study population was made up of 80 males and 43 females, aged 2 to 67 years (mean: 13.2). The male-to-female ratio was 1.9:1. A total of 90 patients (73.2%) were in the pediatric age group (≤15 yr), and 33 patients (26.8%) were considered adults (≥16 yr); the difference between the proportion of younger and older patients was statistically significant (p < 0.001). The incidence of an aural foreign body was directly proportional to age group; the younger the patient, the higher the incidence (Table 1).
Age and sex Distribution.*
Type of Foreign Body and Affected Side
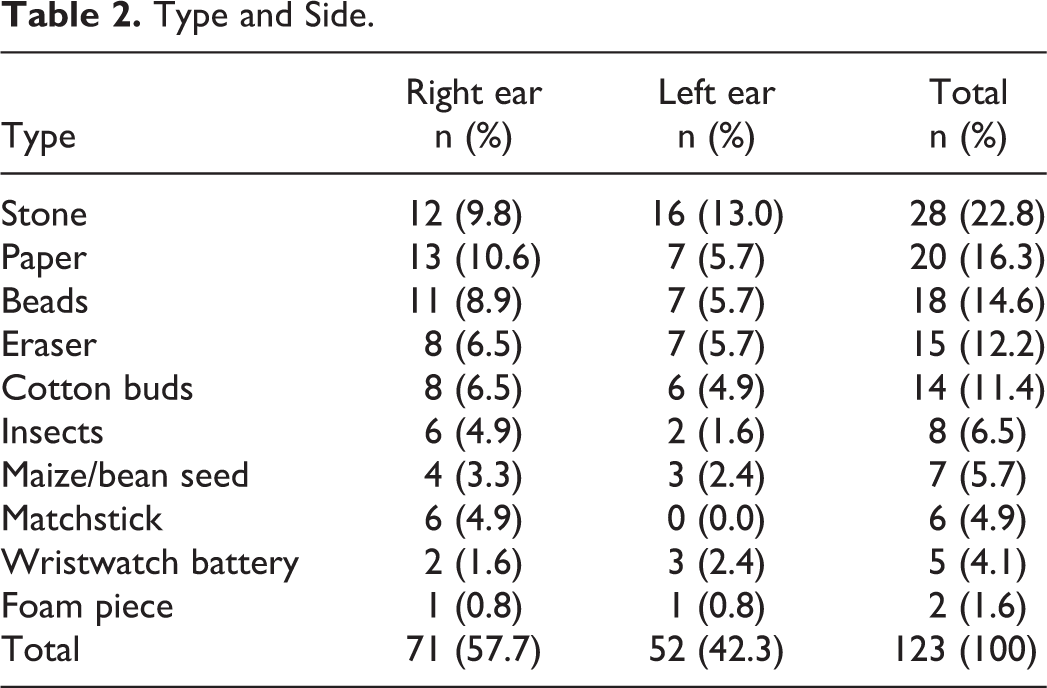
The most common foreign bodies were stones, which were found in 28 patients (22.8%). Other common substances were paper, beads, pencil erasers, and cotton buds. All the cases of cotton bud insertion occurred in adults. Eight patients had an insect in their ear; 6 believed that the insect had crawled into their ear while they were sleeping, and 2 said that the insect had flown into their ear while they were walking down the street. The right ear was affected more than the left (57.7 vs. 42.3%) (Table 2).
Type and Side.
Interval between Onset and Presentation
The time lag between insertion and presentation to our hospital varied greatly. A total of 40 patients (32.5%) presented within 12 hours, 29 (23.6%) between 12 and 24 hours, 35 (28.5%) between 1 day and 1 week, 7 (5.7%) between 1 week and 1 month, 3 (2.4%) between 1 and 3 months, and 1 (0.8%) presented after 8 years. Eight patients (6.5%) were not sure when they had acquired their foreign body.
Presenting Signs and Symptoms
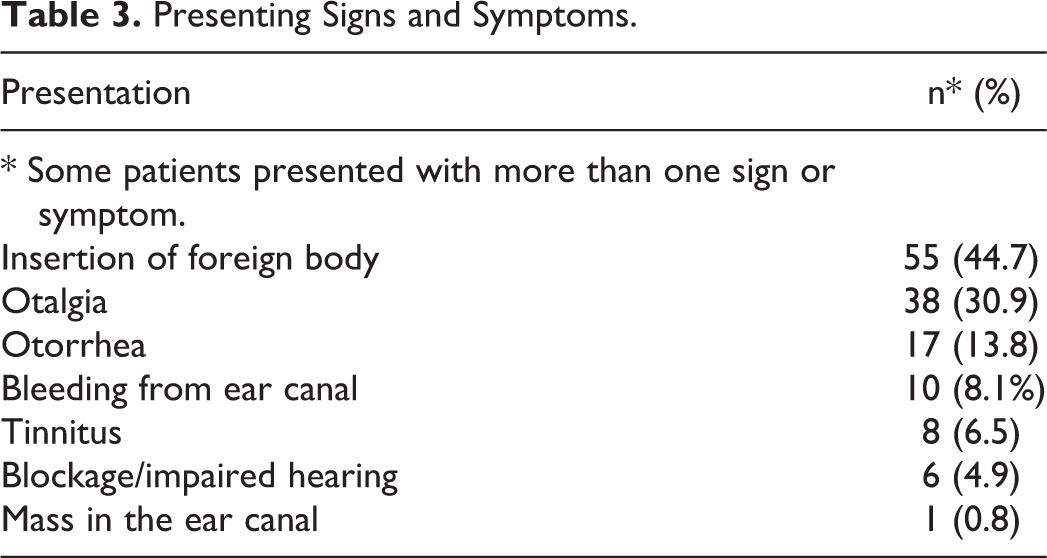
In addition to a primary complaint of an obvious object in the ear, 38 patients (30.9%) presented with otalgia, 17 (13.8%) with otorrhea, and 10 (8.1%) with bleeding from the external auditory canal (Table 3).
Presenting Signs and Symptoms.
Treatment
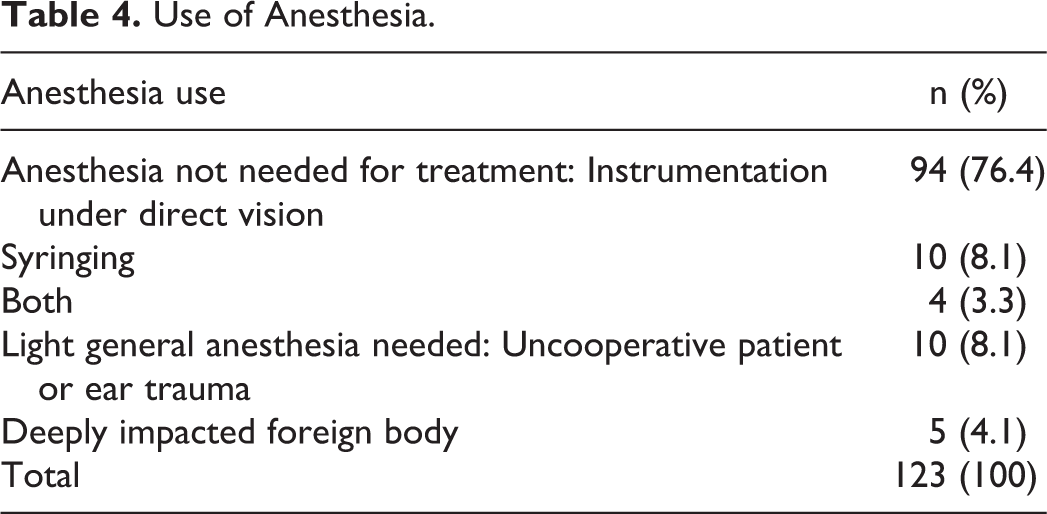
All of the foreign bodies were removed by an otolaryngologist either in the clinic or in the operating theater, depending on the circumstances of each case. In the clinic, 94 patients (76.4%) had the foreign body removed by instrumentation under direct vision, 10 (8.1%) by ear syringing, and 4 (3.3%) with a combination of both, all without the need for general anesthesia. The remaining 15 patients did require light general anesthesia and were treated in the operating theater-10 (8.1%) because they had been frightened by or had experienced considerable trauma during previous attempts at removal by a non-otolaryngologist, and 5 (4.1%) because the foreign body was deeply impacted (Table 4).
Use of Anesthesia.
Previous Attempts at Removal and Complications
Prior to presentation, 30 patients (24.4%) had undergone various attempts at removal of the foreign body by a parent, neighbor, or general physician. Of this group, 23 patients experienced a total of 41 complications. The most common was canal abrasion, laceration, and/or bleeding, which was seen in 17 patients; others were otitis externa in 8 patients, tympanic membrane perforation in 6, impaired hearing in 5, chronic suppurative otitis media in 3, and middle ear involvement in 2. By contrast, only 6 complications (6.5%) occurred in the 93 patients initially treated by an otolaryngologist: canal abrasion, laceration, and/or bleeding in 4 patients and otitis externa in 2. The difference in overall complication rates between patients treated by otolaryngologists and non-otolaryngologists was statistically significant (p < 0.001).
Discussion
The vast majority of foreign bodies that become impacted in the ear are placed there voluntarily, usually by children. 5 The reasons are many; children place things in their ears because they are bored or curious, because they wish to imitate what adults do, and simply because the objects are at hand. 3,13 Most of the patients in our study (73.2%) were classified as pediatric (≤15 yr of age); the largest of the groups categorized in 5-year increments were those aged 5 years and younger (43.1%). Other studies of aural foreign bodies have shown that 38.1 to 64.2% occurred in children aged 0 through 5 years. 3,8,11,13,14
Some 26.8% of the patients in our study were classified as adults (≥16 yr). While boys were affected more than girls in our pediatric group, women were affected more than men in our adult group. Women were more likely than men to use cotton buds to clean their ears. The tips of poorly made buds can become easily detached from the stem. Routine ear cleaning is often done by women after they have had a bath.
The types of aural foreign bodies found in our study are similar to what has been reported in other centers. 3,8,11,13,14 Our findings were unusual in one respect, however; the most common foreign bodies in our study were stones. This might be attributable to the fact that children in Nigeria have more access to stones and often play with them, especially during school recess periods.
Wristwatch battery impaction was documented in 5 of our cases. The hazard posed by these batteries is serious, especially if they remain in the ear for a prolonged time. Many of these batteries contain alkaline substances that can cause liquefactive necrosis of the canal wall and surrounding tissues if not removed promptly. 8,13 Also, adults should be advised that watch batteries must be properly disposed of so that children do not gain access to them.
Eight of our patients had a dead insect removed from their ear. Some of them had already applied palm oil, olive oil, liquid paraffin, or alcoholic spirits to kill the insect.
In our study, the right ear was more often affected than the left (57.7 vs. 42.3%). This ratio is similar to those reported in other studies. 3,8,11 The higher proportion of foreign bodies in the right ear can be explained by the fact that most of the foreign bodies were inserted by patients themselves, and most of these patients were right-handed. 3,11
The interval from onset to presentation varied from a few hours to 8 years. Some 40 patients (32.5%) presented to the hospital within 12 hours of onset, and 69 patients (56.1%) did so within 24 hours. The patient who was not treated for 8 years was in nursery school when he inserted a pencil eraser into his ear; he did not tell his parents because he was afraid of being punished. Over time, the eraser became overgrown by exuberant granulation. Two other children experienced complications months after acquiring their aural foreign body because they failed to inform anyone. The lesson here is that parents and caregivers who suspect an aural foreign body should approach the situation in a nonjudgmental manner so that these objects can be discovered and safely removed before complications develop. 5
There is little scientific evidence regarding the best method of removing foreign bodies from the ear. 5 Therefore, each treatment should be judged on its own merit for every individual case. 13 The choice of procedure should take into consideration the exact location, shape, and composition of the foreign body. For example, nonimpacted hygroscopic objects can be syringed with normal saline at body temperature. Live insects must be killed first by instillation of a suffocating fluid such as olive oil or liquid paraffin.
Instrumentation usually includes a Jobson Horne probe, ear curette, ear loop, and crocodile forceps. Otomicroscopes and cyanoacrylate (Super Glue) can also be used. General anesthesia is useful in some complicated cases and in uncooperative patients. In addition, years of experience often lead to the development of individual innovative techniques that are safe and effective.
In our study, 108 patients (87.8%) had their foreign body removed in the clinic by an otolaryngologist; 94 of the objects (76.4%) were removed under direct vision with appropriate instruments, 10 (8.1%) with syringing, and 4 (3.3%) with both. All of these patients presented without complications, and all were cooperative. In the other 15 patients (12.2%), circumstances dictated that the object be removed after the induction of general anesthesia.
Ideally, patients with an aural foreign body would first seek care from an otolaryngologist, but in Nigeria this is not always possible because there are not enough ENT specialists in most communities. Greater public education and public awareness regarding prevention and treatment would be very helpful, and we urge the leaders of our local healthcare communities to undertake such an effort. Also, we would welcome more continuing medical education for our general duty physicians and greater availability of instrumentation, which would allow them to determine which cases they could safely handle and which should be referred to an otolaryngologist. With better training of general duty physicians, patients would have more options, which might allow them to avoid journeys of hundreds of kilometers on risky roads.
In our study, 30 patients (24.4%) were initially “treated” by untrained personnel, and as a result, they incurred a total of 41 preventable complications. It is also important to recognize that each unsuccessful attempt can significantly jeopardize the success of subsequent efforts. Repeated attempts not only lead to further swelling and bleeding, but they can also compromise a patient’s cooperation. 10
From the Department of Ear, Nose, and Throat Surgery, Federal Medical Centre, Ido Ekiti, Nigeria (Dr. Olajide and Dr. Arigbede); and the Department of Ear, Nose, and Throat Surgery, College of Health Sciences, University of Ilorin, Ilorin, Nigeria (Prof. Ologe).
Footnotes
Authors' Note
Foluwasayo E. Ologe is now affiliated with Department of Ear, Nose and Throat Surgery, University of Ilorin Teaching Hospital, Ilorin, Nigeria.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.