
Abstract

Medication-related osteonecrosis of the jaw (MRONJ) is a pathologic process that rarely follows exposure to antiresoptive agents such as bisphosphonate or denosumab, which are used to treat lytic bone lesions in patients with osseous metastases related to carcinoma of the breast or prostate, multiple myeloma, Paget’s disease, and osteoporosis. These drugs inhibit osteoclastic bone resorption and remodeling.
The risk of osteonecrosis of the jaw in patients receiving either bisphosphonate or denosumab ranges from 0.7% to 6.7%. 1 However, this condition occurs more commonly in patients receiving the medication intravenously and after a surgical dental procedure, such as extraction or implant placement. The diagnosis of MRONJ is made clinically when there is nonhealing exposed bone persisting for more than 8 weeks in a patient with current or previous treatment with antiresorptive agents but without a history of radiation therapy to the jaws. 2
Radiologically, the bone can be normal in the early stages. In advanced cases, a mixture of bone sclerosis and rarefaction occurs. Bone sequestra are seen more commonly in the mandible and often the sequestra appear as radiopaque islands of bone in radiolucent regions (Figure 1). Large sequestrum may weaken the bone and promote pathologic fracture. In contrast to osteomyelitis, there is no periosteal bone reaction in most cases. 3
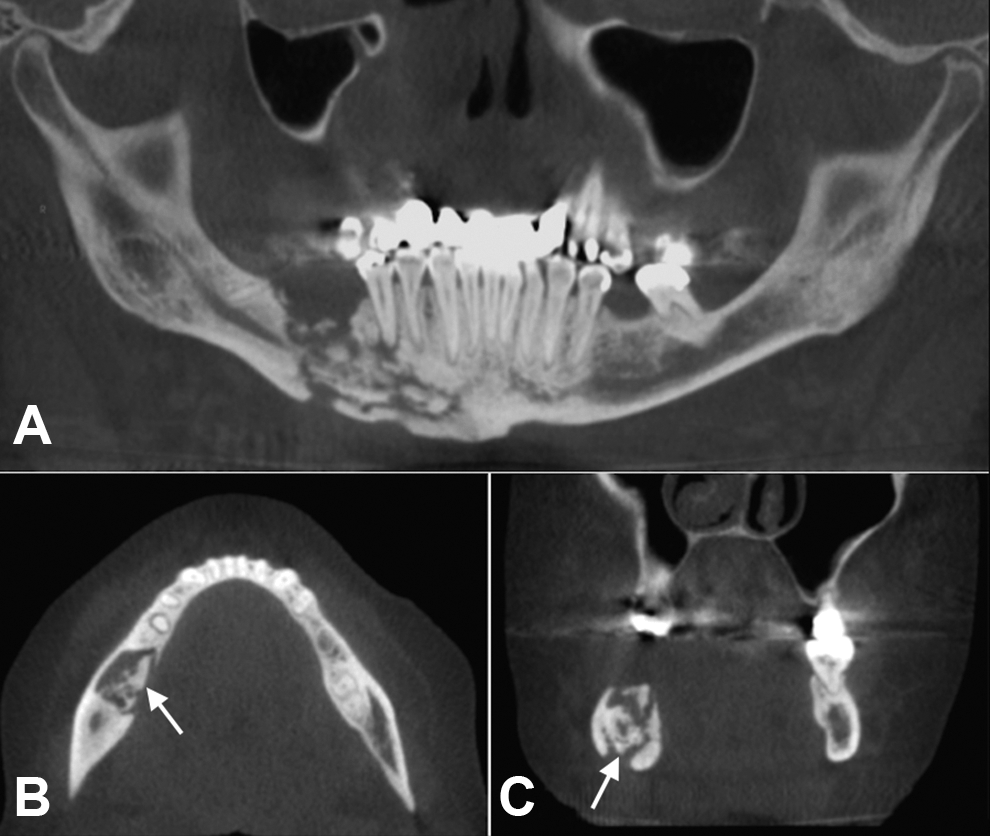
A 61-year-old woman with osteochemonecrosis of the right mandible. The patient was treated with intravenous bisphosphonates for metastatic breast cancer. A, Cone beam computed tomography (CT) reformatted thin-slice panoramic image shows large region of bone destruction in the right body of the mandible with diffuse sclerotic bone reaction and presence of multiple sequestra. Axial (B) and coronal (C) cone beam CT images show increase in density and size of the right mandible compared with the left side. Arrows (B and C) point to a large sequestrum. There is no evidence of periosteal bone formation.
Magnetic resonance imaging can detect the early stage of the disease. The bone marrow shows low signal intensity on T1-weighted images and high signal intensity on T2-weighted images. 4
In patients with osteonecrosis of the jaw, regular preventive dental care is of foremost importance. 2 Conservative treatments include maintaining good oral hygiene, eliminating sources of infection, and application of antimicrobial mouth rinses. Because of the reduced healing capacity of bone, surgical intervention should be limited to a minimal debridement of the exposed necrotic bone. Systemic antibiotics and hyperbaric oxygen may be used as adjunctive therapies. 1,2
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article