
Abstract

A 23-year-old woman presented with a 4-month history of recurrent nasal bleeding and left-sided nasal obstruction. She had no history of antecedent trauma, nasal surgery, or bleeding diatheses. Also, she denied no significant past medical history or anticoagulant drug use. General examination and complete hematology profile and coagulation tests were normal. On nasal endoscopy, 2 large polypoid masses were observed completely obstructing the left nasal cavity, without evidence of increased vascularity (Figure 1). Computed tomography (CT) scans of the paranasal sinuses (PNS) revealed an expansile heterogeneous opacification of the left maxillary sinus bulging into the left middle meatus and ethmoid sinus associated with partial destruction of the superior medial wall of the maxillary sinus (Figure 2). The opacification between left maxillary sinus and middle meatus consisted of patchy hyperattenuating areas centrally and circumferential hypoattenuation (Figure 2). Preoperative endonasal endoscopic biopsy was performed and showed inflammatory polyp. Under general anesthesia, the mass was completely removed using middle meatal antrostomy with endoscope. A friable dark reddish blood clot and thick fibrous tissue filled the maxillary sinus. After complete removal of the mass, the maxillary sinus mucosa was slightly edematous and kept intact. The lesion consisted of hematoma with fibrosis and angiogenesis (Figure 3). These findings were consistent with the organized hematoma. The patient remained asymptomatic 12 months after surgery.
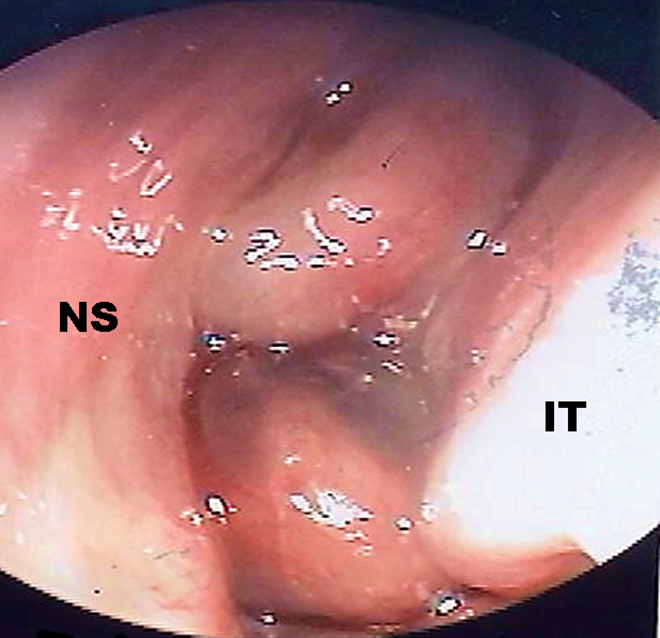
On nasal endoscopy, 2 large polypoid masses were observed completely obstructing the left nasal cavity. IT indicates inferior turbinate; NS, nasal septum.

Paranasal sinus (PNS) computed tomography scans with contrast enhancement revealed an expansile heterogeneous opacification of the left maxillary sinus bulging into left middle meatus and ethmoid sinus associated with partial destruction (thick black arrow) of the superior medial wall of the maxillary sinus. The opacification between left maxillary sinus and middle meatus consisted of centrally patchy hyperattenuating areas (white asterisk) with circumferential hypoattenuation (black asterisk; thin black arrow: mass margin, white arrow: inferior turbinate). (A & B, axial images; C, coronal image).
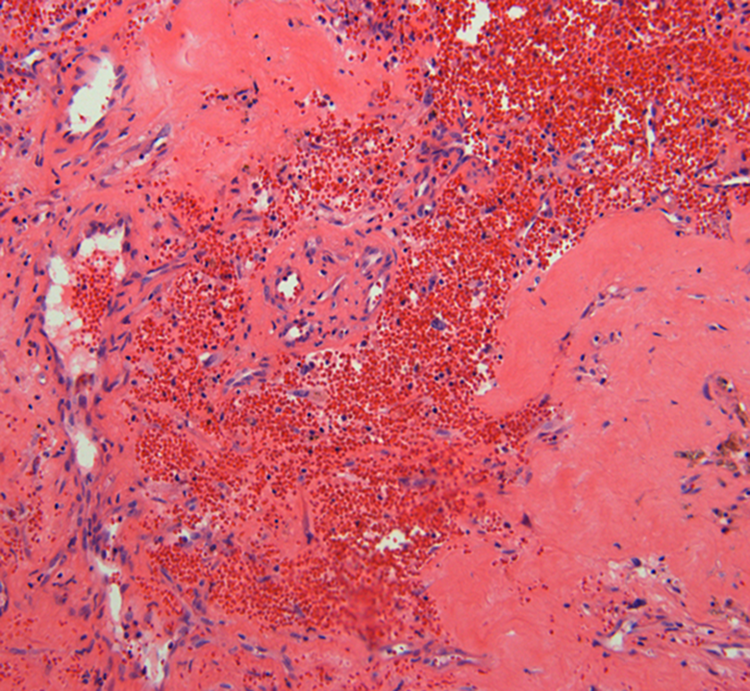
The histopathological findings were composed of a mixture of fibrous tissue with hyalinization, neovascularization, and extravasated red blood cells in the subepithelium.
Sinonasal organized hematoma (SNOH) is a rare benign disease that its clinical and radiographic characteristics result in being misdiagnosed as malignant or locally aggressive neoplasms and cause excessive worries to patients and physicians. 1 So, the highly clinical suspicion, the accurate preoperative diagnosis, and the proper therapeutic planning for SNOH are essential to avoid unnecessary excessive surgical intervention as the simple conservative endoscopic sinus surgery is typically curative with rare recurrence. 2,3 However, SNOHs present a diagnostic dilemma for most otolaryngologists and neuroradiologists.
The exact underlying etiological or pathophysiological mechanisms remain unclear, but currently, 2 prevailing hypotheses have been suggested: the vascular compromise of nasal polyps and the formation of hematoma. 4 Although SNOH can occur in any location of PNS and nasal cavity, the most commonly affected site is the unilateral maxillary sinus. 4 Because the maxillary sinus is the largest PNS that allows negative pressure, significant leakage of blood may develop in the nasal cavity into the sinus through the ostium. 5 Accumulation of blood, poor ventilation, and poor drainage prevent the reabsorption of the hematoma and lead to neovascularization and fibrosis, which results in the eventual formation of organized hematoma. 4
The presenting symptoms of SNOH may be various and nonspecific, including frequent epistaxis and nasal obstruction, followed by cheek pain, severe headache, epiphora, and exophthalmos in order of frequency. 4
Although diagnostic criteria for correctly identifying SNOHs are not well established, the number of reported cases has dramatically risen since 2005 as the characteristic radiographic and histopathological findings became clearer. 6 Until now, the most characteristic feature to confirm the diagnosis as SNOH is the biphasic appearance on magnetic resonance imaging (MRI) findings which shows marked heterogeneous signal intensity (central part, areas of fresh hemorrhage) with the distinct hypointense peripheral rim on T2WI (zone of fibrosis, “shells” of T2 hypointensity). 1,4 However, the most important limitation of MRI is that patients with severe claustrophobia cannot perform MRI scan in closed gantry systems.
Other methods for accurate preoperative diagnosis include nasal endoscopy, preoperative biopsy, and CT imaging. Nasal endoscopic examination reveals various and nonspecific features, even mimicking chronic rhinosinusitis with nasal polyposis like the present case. 3 Preoperative biopsy taken from the periphery does not help preoperative diagnosis because distinct pathological differences are observed between the central and peripheral portions of SNOHs. 6,7 Although CT findings with high diagnostic value have not been reported so far, erosion of the bony sinus walls with heterogeneous enhancement (irregular patchy, nodular, papillary, or frond-like enhancement due to hemorrhage and neovascularization in various stages) may facilitate the diagnosis of SNOH, like the present case. 4,8 The most common site of erosion is the medial wall of the maxillary sinus, including the uncinate process. 8 The histopathological findings of SNOH are characterized by a mixture of bleeding, dilated vessels, hemorrhage, fibrin exudation, fibrosis, hyalinization, and neovascularization.
Differential diagnoses of a unilateral sinonasal mass should include mucocele, fungus ball, inflammatory polyp, cholesterol granuloma, inverted papilloma, hemangioma, and carcinoma. 8 Mucocele, fungus ball, cholesterol granuloma, inflammatory polyp, and hemangioma can be easily differentiated from an organized hematoma due to different enhancement patterns of CT. 8 Differential diagnosis with inverted papilloma may be possible in 2 points, mainly occurring on the lateral wall of the nasal cavity and distinctive MRI appearances, referred to as convoluted cerebriform pattern. 8 Sinonasal carcinoma commonly shows the definite bony destruction with adjacent tissue invasion, rather than smooth erosion of the sinus walls seen in SNOHs. 5,8
In conclusion, although SNOH presents a diagnostic challenge for otolaryngologists, we should keep in mind that the correct diagnosis and proper management can be achieved by knowledge of its typical imaging features including CT and MRI.
Footnotes
Authors’ Note
The patient’s permission was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.