
Abstract

A 56-year-old man with chronic kidney disease on hemodialysis for 5 years presented with a growing neck mass and dysphagia. He complained of choking episodes, dyspnea on exertion, and difficulty sleeping supine. On examination, he had a firm left neck mass with right tracheal deviation and a smaller firm mass to the right of the hyoid with hyoid fixation. On flexible laryngoscopy, he had submucosal deposits resulting in deformity of the epiglottis and pharyngeal walls (Figure 1). A computed tomography (CT) scan demonstrated significant calcium deposition in his neck (Figure 2). A modified barium swallow demonstrated inhibited hyolaryngeal elevation and pooling of piriform residue with aspiration after multiple swallows (Figure 3). He was referred for surgical excision and was offered debulking for cosmesis or a total laryngectomy for dysphagia. He elected to continue medical management with cinacalcet and fosrenol and was referred for parathyroidectomy.
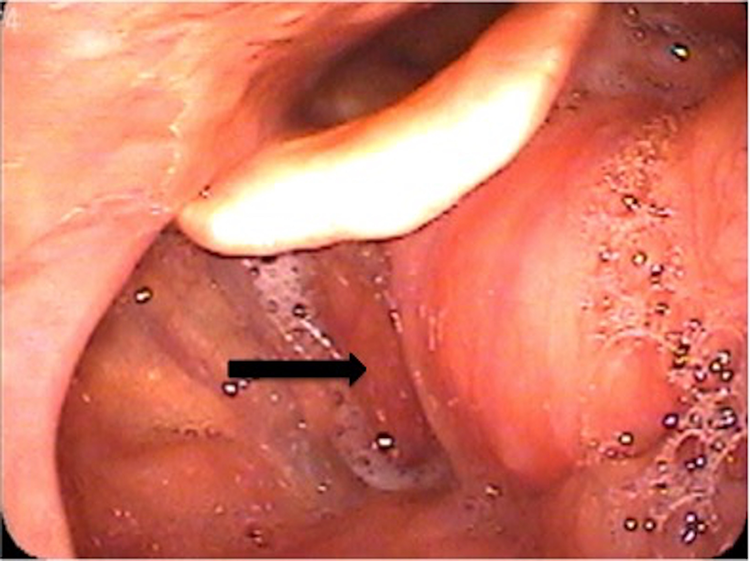
Flexible laryngoscopy with submucosal mass (black arrow) in the vallecula.

This is an axial view of a bony window computed tomography (CT) neck without contrast showing significant calcinosis extending through the level of the hyoid bone.

This is a plain film sagittal view during a modified barium swallow, showing calcinosis anterior to the airway (black arrow) and a small amount of aspiration (white arrow).
Chronic kidney disease is the most common cause of secondary tumoral calcinosis. In patients undergoing hemodialysis, the prevalence is estimated to be 0.5% to 1.2%. 1 A specific cause for an individual’s unique pattern of deposition is unknown; however, the characteristic radiographic finding is that of amorphous, cystic, and multilobulated calcium deposition in the periarticular area. 2 The treatment mainstay is medical management of the underlying condition. 3 Surgical intervention should be reserved as a last resort as it has been associated with higher rates of complications. 3 There has been only one other case report to our knowledge of tumoral calcinosis involving the airway, in which a patient with dysphagia was found to have calcifications of the supraglottis and required suspension microdirect laryngoscopy for debulking and tracheostomy. 4 Thus, in patients with significant upper airway involvement, there may be a limited role for sole medical management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.