
Abstract
Purpose:
To identify the main complaints, diagnostic tools, as well as the treatment plan in patients presenting with oropharyngeal dysphagia in the acute care settings.
Methods:
The electronic medical chart of 100 consecutive hospitalized patients who presented an oropharyngeal dysphagia were retrospectively reviewed from January 2017 to January 2019.
Results:
The mean age of patients was 76.03 (standard deviation = 16.06) years old with 71% of patients being males. The most common admission diagnosis was pneumonia (30%), followed by stroke (28%). The swallowing evaluation was performed on the regular floor in 85% of patients and in the intensive care unit in 15% of patients. The main reasons for the swallowing evaluation are suspicion of aspiration by the medical or nursing teams (60%), systematic evaluation (20%), ear, nose and throat (ENT) complaints by the patient (14%), and aspiration pneumonia (6%). Fiberoptic endoscopic evaluation of swallowing with sensitivity testing was the most common diagnostic tool used alone in 88% of patients. Diet and postural modifications were prescribed to 71% and 62% of the patients, respectively. Swallowing exercises were performed in 43% of patients. Overall, otolaryngologist interventions resulted in an increased rate of patients getting oral intake compared to nonoral feeding routes (P = .05).
Conclusions:
This study adds knowledge about the causes and characteristics of oropharyngeal dysphagia in an acute tertiary medical setting. It also provides insights regarding the role, and the consequences of a swallowing intervention led by an ENT specialist in collaboration with the members of the health team.
Introduction
Oropharyngeal dysphagia (OD) affects different age groups. It is more common in ageing patients, affecting up to 30% of the elderly population. 1 The most common etiologies vary according to the treatment settings: acute care versus chronic care settings. 2 The most common etiologies of OD are neurological disorders of the central or peripheral nervous system (eg, stroke, Parkinson disease, Alzheimer disease, amyotrophic lateral sclerosis), structural disorders (eg, head and neck cancer tumor, surgery or radiation therapy effect), immunologic, and inflammatory disorders (eg, Myasthenia gravis, polymyositis). 3 Oropharyngeal dysphagia in the acute care setting is an underreported patient-related symptom common to several complex medical conditions. It has many consequences: it increases hospital length of stay and costs 4,5 ; it can aggravate or can be an independent risk factor for malnutrition, dehydration, and pneumonia 6 -8 ; and it can also reduce quality of life (QoL). 4,5 Early recognition and intervention are critical to avoid complications, however if there is not a high index of suspicion, OD can be overlooked. 4 Moreover, if it is not well assessed by objective instrumental diagnostic tools (functional endoscopic evaluation of swallowing and/or modified barium swallow [MBS]) and treated according to their findings, its consequences can aggravate the patient’s health status and an inadequate feeding method can be used.
The characteristics of patients with OD in a general acute care setting as well as the effect of an appropriate assessment strategy are missing in Lebanon. The aim of this study is to investigate the causes of OD, evaluation findings (with the study of a relation between diminished sensitivity or pharyngeal residue and aspiration pneumonia), main initial interventions, and the results (in terms of the feeding route and referral rates) of the intervention program in patients with OD in an acute tertiary care university hospital setting in Beirut, Lebanon.
Materials and Methods
After obtaining the approval of the local Ethics Committee (CEHDF 1437), the electronic medical chart of 100 consecutive hospitalized patients who presented an OD in Hotel-Dieu de France Hospital, Beirut (Lebanon), were retrospectively reviewed from January 2017 to January 2019. Information regarding patient demographics, admission diagnosis, OD workup, as well as management algorithms and outcomes measurements were abstracted and tabulated. Functional endoscopic evaluation of swallowing with sensitivity testing (FEES-ST) or FEES-ST associated with a modified barium swallow (MBS) were the main evaluation methods used for assessment according to our institution protocol. Functional endoscopic evaluation of swallowing with sensitivity testing findings were documented and classified as oral, pharyngeal, or esophageal phase findings accordingly. Pharyngolaryngeal sensitivity was tested using the tip of the endoscope touching one of the arytenoids. A positive laryngeal adductor reflex or a positive cough reflex were considered as indicators of intact sensitivity. 9 Pharyngeal and laryngeal motility were evaluated through the “pharyngeal squeeze manoeuver” (PSM) and the evaluation of vocal cord motility. During the PSM, the patient is asked to make high-pitched, strained phonation, preferably in a rising crescendo of effort. This will, in normal pharynges, result in obvious recruitment of the pharyngeal constrictor musculature. 9,10 The PSM was shown in previous works to be a valid surrogate measure of pharyngeal motor integrity. 11 Penetration and aspiration were assessed endoscopically based on the modified endoscopic penetration-aspiration scale. Pharyngolaryngeal residues were also assessed and documented based on the Yale pharyngeal residue scale. 12 An overall assessment supervised by our senior laryngologist contributed into the elaboration of a customized treatment protocol. This protocol consists mainly of texture modifications of solids and liquids, head posture adjustments, and swallowing rehabilitation maneuvers conducted by the in-hospital intervention speech and language pathology (SLP) team. To assess the impact of the OD intervention, we conducted a comparison between the feeding routes before and after the OD evaluation as well as the progression of referrals over time.
Statistical Analysis
Initially, descriptive analysis was performed using counts and percentages or mean ± standard deviation (SD). Bivariate analysis was then carried out to describe the association between diminished laryngeal sensitivity and variables of interest (namely route of feeding and aspiration pneumonia). In addition, OD characteristics were compared between patients who were admitted with pneumonia and those who were admitted with another diagnosis. For categorical variables, we used the Pearson χ2 or Fisher exact tests when applicable. Continuous quantitative variables were analyzed using student (independent) t test and Mann-Whitney test when normal or abnormal distribution was assumed, respectively. Valid 2-sided P values were reported, P < .05 was considered statistically significant. All analyses were done using SPSS version 21.0 (IBM Corporation, Armonk, New York).
Results
Demographic Data
The mean age of patients was 76.03 (SD = 16.06) years with 71% of patients being males and 29% females. The most common admission diagnosis was pneumonia (30%), followed by stroke (28%) and nonrespiratory infections (10%). The swallowing evaluation was performed on the regular floor in 85% of patients and in the intensive care unit (ICU) in 15% of patients. The main reasons for the swallowing evaluation are suspicion of aspiration by the medical or nursing teams (60%), systematic evaluation (20%), ENT complaints by the patient (14%), and aspiration pneumonia (6%). The main characteristics of the study population can be found in Table 1.
Main Characteristics of the Study’s Population.
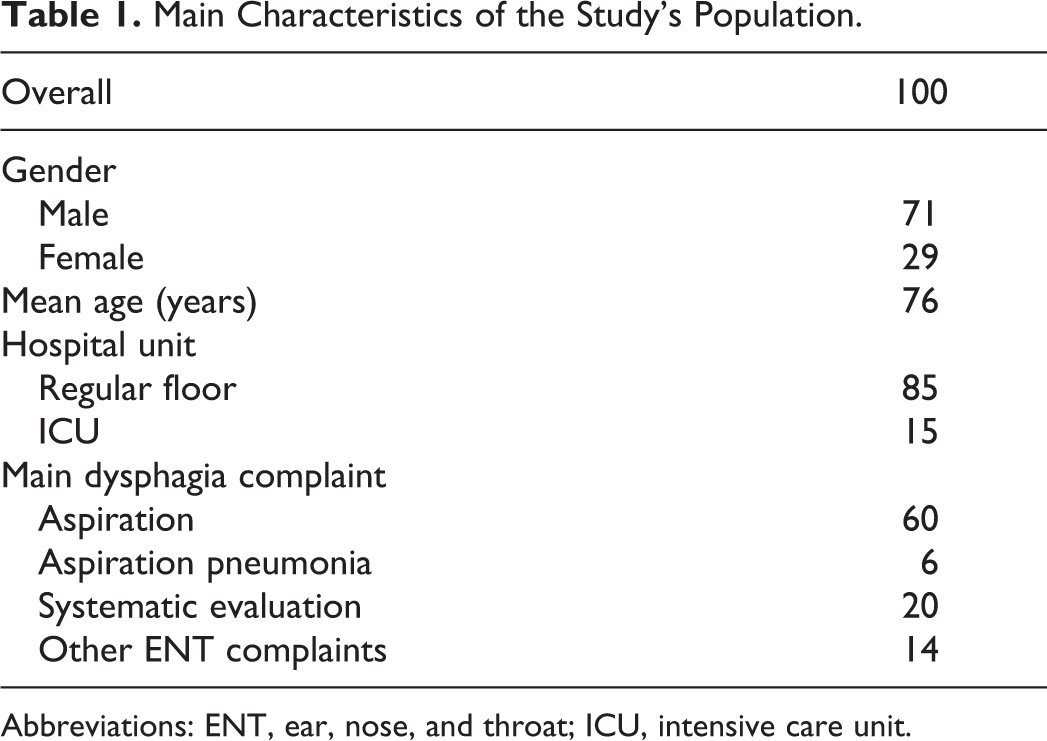
Abbreviations: ENT, ear, nose, and throat; ICU, intensive care unit.
Instrumental Evaluation of OD
Fiberoptic endoscopic evaluation of swallowing with sensitivity testing was the most common diagnostic tool used alone in 88% of patients, whereas MBS was used as an adjunct diagnostic tool in 12% of patients. Penetration-Aspiration was present in 28% of patients, moderate-to-severe residue was present in 31% of patients, and reduced sensitivity was present in 35% of patients. No correlation was found between the amount of residue and reduced pharyngolaryngeal sensitivity (P = .64), however patients with reduced sensitivity were more likely to have non-oral feeding (P = .05) when discharged from the hospital.
Interventions to Treat OD
Diet and postural modifications were prescribed to 71% and 62% of the patients, respectively. Swallowing exercises were performed in 43% of patients. Overall, otolaryngologist interventions resulted in an increased rate of patients getting oral intake compared to nonoral feeding routes (P = .05; Figure 1). During this period, we also observed a constant increase in OD referral as can be seen in Figure 2.
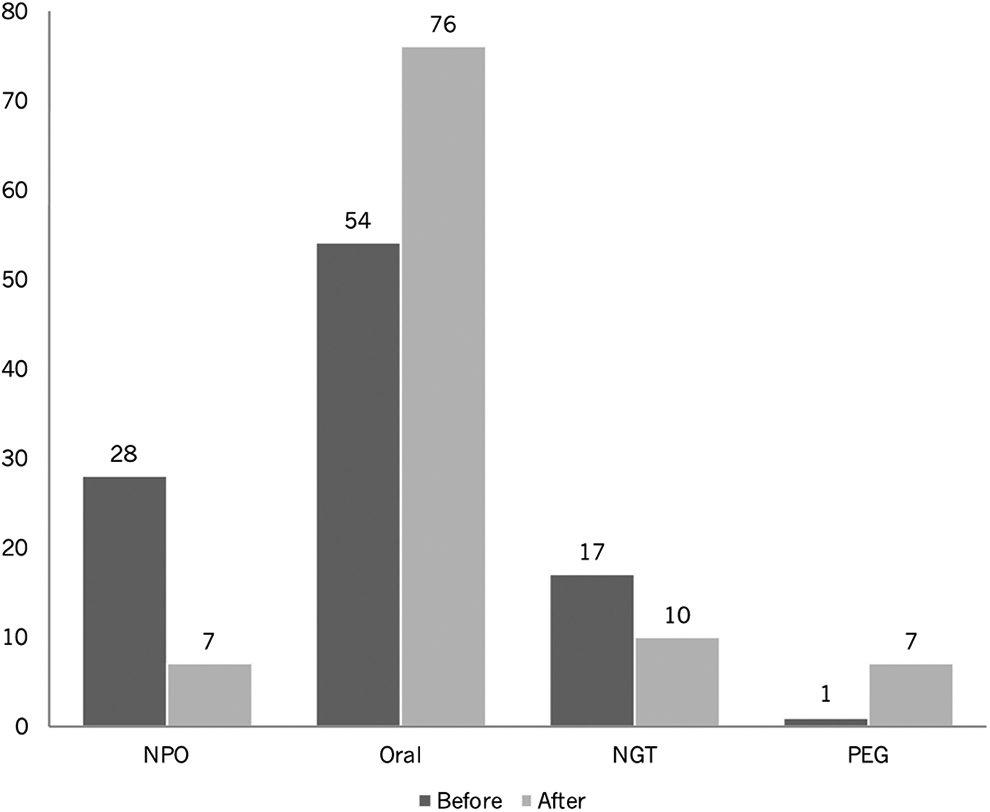
Different routes of feeding before and after OD evaluation. OD indicates oropharyngeal dysphagia.
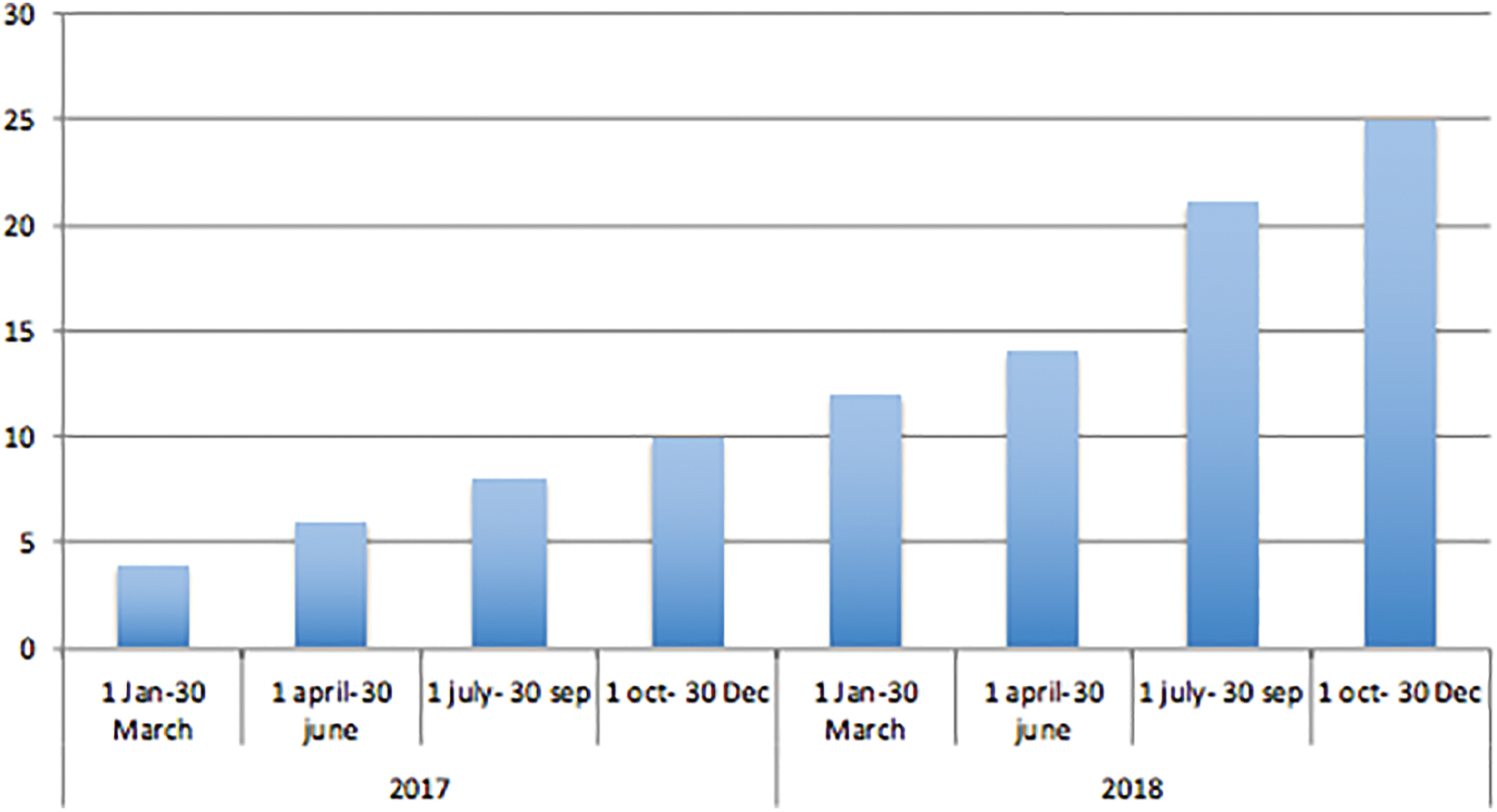
Evolution of referral rate for OD assessment. OD indicates oropharyngeal dysphagia.
Discussion
The mean age of patients in this cohort was 76 years with substantially high proportion of males (71%) compared to female patients (29%). In a similar epidemiological study, evaluating dysphagic patients in an acute care geriatric hospital, Leder et al showed similar trends with 54.7% and 44.3% of men and women, respectively. 12 It is believed that the greater incidence of dysphagia in males may be due to women retaining greater muscle reserve than men, thus resulting in a greater laryngeal displacement during swallowing. 12 The 2 most common admission diagnosis in patients referred for OD evaluation in our medical center were pneumonia and stroke, with 30% and 28% respectively. Interestingly, the main participants admitting diagnosis in Leder et al cohort were general medical conditions (33%) and pneumonia (17%). They noticed, however, that the high proportion of patients in the general medical condition category might be the reflection of the reliance on admitting diagnosis to sort patients into respective diagnostic categories. Past medical conditions, such as strokes, neurodegenerative disorders might be missed since they could differ from the admitting diagnosis. The etiologies of swallowing disorders affecting elderly people in an outpatient setting are different from inpatient setting. In a retrospective study evaluating the causes of dysphagia in a tertiary care outpatient-swallowing center, Hoy et al found that laryngopharyngeal reflux, postirradiation dysphagia, and cricopharyngeal muscle dysfunction were the main causes of dysphagia. 13 These etiologies were very rare in this study’s population. According to our findings, it is very important to have a high index of suspicion of OD in patients admitted with the diagnosis of stroke or pneumonia in an acute care hospital setting; this is especially true in men.
The main dysphagia assessment tool in this cohort was FEES-ST. It was used in 100% of referred patient, while MBS was used as an adjunct tool in 12% of patients. Functional endoscopic evaluation of swallowing with sensitivity testing can be performed at patient’s bedside with portable equipment, thus, permitting a rapid evaluation and elaboration of treatment plan. It also spares patients the need to be moved to the radiology department for MBS. Functional endoscopic evaluation of swallowing with sensitivity testing has finally the advantage of a direct evaluation of the anatomy and function of the upper aero digestive tract. In the in-patient setting especially when the patient has difficulties to move or to sit on a chair, it is a very valuable tool. 14,15 Modified barium swallow was considered whenever a cricopharyngeal muscle dysfunction or an esophageal disorder were suspected.
This study didn’t show a statistically significant association between the amount of pharyngeal residue and the sensitivity of the larynx evaluated by touching the arytenoids. Interestingly, prior studies have shown that pharyngeal residue represents a reflection of pharyngeal muscle strength and constriction rather than pharyngolaryngeal sensitivity. 16 However, our study showed that patients with reduced sensitivity were more likely to have non-oral feeding when discharged from the hospital. This finding is consistent with Borders et al prospective study that showed a clear association between altered laryngeal sensation, aspiration, and diet modification. 16 These findings emphasize the need of the evaluation of both motor and sensitivity of swallowing to have a complete view of the patient’s swallowing.
We observed that after instrumental evaluation, more patients were on oral diet. This reflects that some decisions regarding the shift of feeding to a non-oral route based on subjective bedside evaluation do not reflect the real capacities of the patient. This is why objective assessment of patients with OD can limit these inadequate decisions that may negatively impact the patient’s QoL. 17 Indeed, patients with nasogastric tube (NGT) have significantly lower QoL comparing to patients receiving oral feeding on different QoL scales. 18 If abnormal swallowing patterns are discovered than swallowing rehabilitation is the main way to guide the patient to an efficient and safe swallowing. If safe swallowing cannot be maintained despite rehabilitation than percutaneous endoscopic gastrostomy (PEG) should be considered because it is safer for long-term nonoral intake than NGT feeding.
Moreover, the referral rate to our dysphagia ambulatory unit demonstrated a steady and consistent increase in referrals throughout the study period. In our perspective, this trend reflects the increase in dysphagia awareness among primary physicians and nurses and may reflect the positive impact of our intervention on dysphagia patients.
The strengths of this study are many and varied. To date, there is a scarce number of studies evaluating the causes of OD in general tertiary medical centers, the referring paradigms, the management protocol, and the outcomes of ENT specialist intervention at different scales. To the best of our knowledge, it is the first study to evaluate the main causes of OD in a Lebanese tertiary acute care medical center. It sheds some light on the different diagnostic modalities and algorithms used to evaluate patients with OD as well as the different treatment approaches used in our institution.
This study has however some limitations. Firstly, the design of our cohort is retrospective. Thus, the conclusion of our statistical analysis should be interpreted cautiously. Secondly, the evaluation of OD was not universal for every patient in the medical center aspirating or at risk of swallowing disorders. It relies mainly on the primary physician or nursing team asking for an otolaryngology swallowing evaluation. Thus, there is a possible bias in selecting only the severe cases for swallowing evaluation. Thirdly, although the admitting diagnosis is known in our patients, each of them has past medical histories and comorbidities that can contribute to the pathophysiology and the severity of dysphagia. Thus, many confounding factors made our population less homogenous. Finally, a long-term follow-up of patients was not performed to evaluate the impact of our swallowing intervention on a long-term scale.
Conclusion
This study adds fundamental knowledge about the causes and characteristics of OD in an acute tertiary medical setting. It also provides insights regarding the role and the consequences of a swallowing intervention led by an ENT specialist in collaboration with the other members of the health team particularly the increase in the number of patients receiving oral diet compared to other feeding routes. We hope that these results will highlight the importance of having a high index of suspicion of OD in patients with a complex medical status and will lead toward implementing systematic evaluation of swallowing in high risk in-hospital populations. An important question that remains to be studied is the impact of our swallowing interventions on long-term morbidity and mortality.
Footnotes
Authors’ Note
N. Matar contributed to the conception and design of the work; acquisition, analysis, and interpretation of data for the work; revision of the manuscript; and final approval of the version to be published. H. Smaily contributed to the conception and design of the work; acquisition, analysis, and interpretation of data for the work; drafting the work and revising it critically; final approval of the version to be published. P. Cherfane and C. Hanna contributed to the conception and design of the work; acquisition, analysis, and interpretation of data for the work; drafting the work; final approval of the version to be published. Patients (or their parents or guardians) have given their written informed consent and the study protocol was approved by the local Ethics Committee (CEHDF 1437).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.