
Abstract
Adenosquamous carcinoma of the head and neck is a rare cancer associated with poor prognosis. Histologically, it is identified through the presence of both adenocarcinoma and squamous cell carcinoma, although it may be difficult to diagnose from initial endoscopic biopsies. We report a case of adenosquamous carcinoma of the glottis in an 82-year-old female patient who presented with progressive hoarseness of voice and in whom initial biopsies had shown only moderate to severe dysplasia. This is the first case in the literature of a primary adenosquamous carcinoma of the glottis managed successfully with a CO2 laser left type Va cordectomy. The patient remained disease-free 28 months postoperatively.
Introduction
Adenosquamous carcinoma (ASC) is a rare type of head and neck cancer, representing less than 1% of cases. However, it is an important diagnosis to be aware of as it can easily be missed on initial endoscopic biopsies due to the nature of the histology. This may have an effect on clinical outcome and long-term survival as it is known to be an aggressive disease often associated with regional or distant metastases. Due to its rarity, there is no overall consensus as to its best management, although current practice typically involves surgical excision with or without adjuvant chemo/radiotherapy, depending on staging at presentation. There are only a limited number of cases of ASC of the glottis in the literature, all treated with open laryngectomy and/or chemoradiotherapy. We present here a case of ASC of the glottis treated successfully with transoral laser surgery, as well as a literature review of previous relevant case studies.
Case Report
An 82-year-old female patient initially presented to our tertiary referral head and neck center with a 3-month history of persistent dysphonia associated with occasional difficulty swallowing. She had no history of weight loss, had never smoked, and did not drink alcohol. Flexible nasendoscopy of the upper aerodigestive tract revealed a thickened left vocal cord, with overlying normal mucosa. The patient was listed for a direct laryngoscopy under general anaesthesia that confirmed a bulky left vocal cord but no associated epithelial abnormalities. The biopsy showed only moderate dysplasia, with very focal severe dysplasia.
Regular follow-up showed no progression until 27 months later when the patient complained of worsening hoarseness. The flexible laryngoscopy on this occasion demonstrated a bulkier left vocal cord with normal mucosa, raising the possibility of a submucosal lesion. The vocal cords’ movement was normal, and there were no other abnormalities on examination. In light of the patient’s worsening symptoms, she was listed for a repeat microlaryngoscopy, which showed no evidence of mucosal changes. Histology from incisional biopsy again confirmed moderate dysplasia of the vocal cord.
The patient was initially reluctant to proceed with laryngeal microsurgery due to worries about her voice postoperatively; however, she underwent a further microlaryngoscopy that confirmed a submucosal lesion centered on the mid third of the left vocal cord, with overlying normal epithelium (Figure 1). The lesion was excised, performing a CO2 laser (Sharplan 40C set on 3.5 watts, continuous wave in super-pulsed mode) left type III cordectomy. Intraoperatively, the tumor appeared to involve the anterior ventricle, and a separate specimen was sent from the anterior deep margin of the vocal cord.
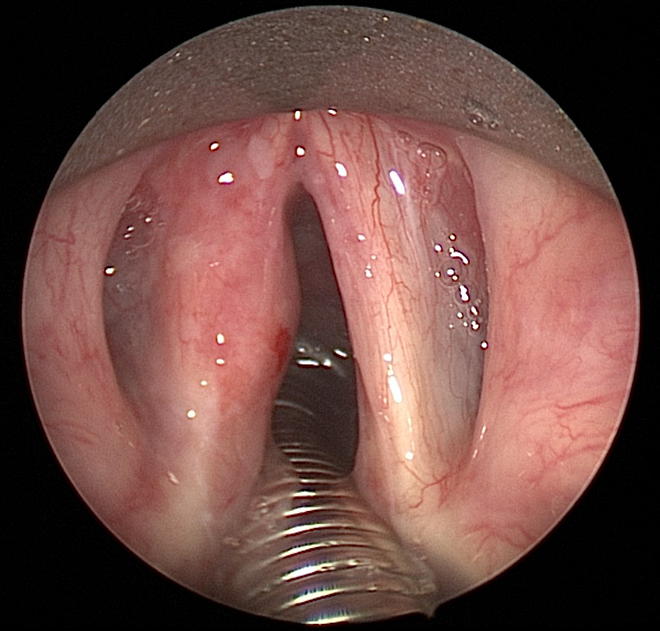
A lesion centred on the mid third of the left vocal cord demonstrated on microlaryngoscopy.
Histology demonstrated moderate to severe dysplasia, focally amounting to carcinoma in situ. The stroma was extensively infiltrated by malignant tumor with squamous and glandular differentiation, showing ductal structures without mucocytes (Figure 2). Immunohistochemistry showed the tumor to be strongly positive for CK5/6 (Figure 3) and p63 in both the squamous and glandular component, while CEA, BerEP4, CA19.9, and CAM5.2 were positive in the glandular component only. The tumor was negative for CK7, TTF1, and CDX2. Mucin was shown to be present within the glandular lumen (Figure 4). The presence of carcinoma in situ on the surface of the sample and the results of immunohistochemistry led to a diagnosis of primary ASC of the left vocal cord. The resection margins were all clear except the anterior deep margin that was positive for invasive ASC. Following multidisciplinary team (MDT) meeting discussion, the patient underwent a magnetic resonance imaging (MRI) neck and positron emission tomography/computed tomography (PET-CT). The MRI neck demonstrated no invasion of the paraglottic space or thyroid cartilage and the PET-CT showed no evidence of metastatic disease. The subsequent MDT recommendation was for further transoral laser surgery to ensure a radical resection with wider margins. Since the histology had demonstrated a positive anterior deep margin, a CO2 laser left type Va cordectomy was performed. The final histology was reported as showing only mild dysplasia but no residual carcinoma in situ or invasive malignancy. Following head and neck MDT, the tumor was staged as T2N0M0. At 28 months after surgery, there was no evidence of recurrence.
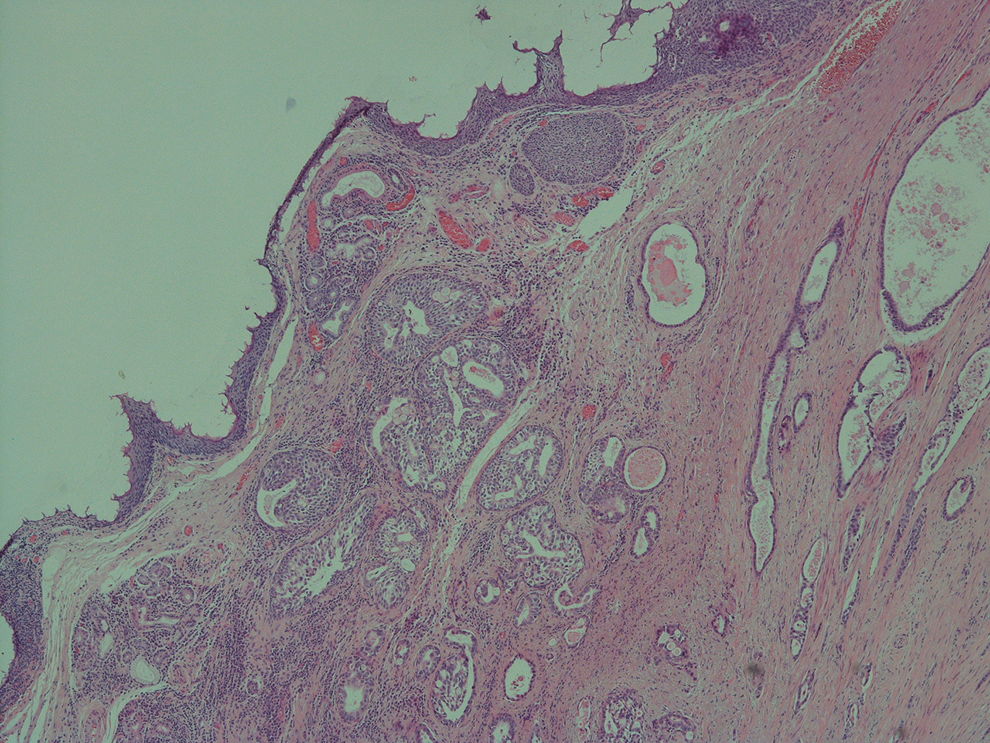
Invasive adenosquamous carcinoma.
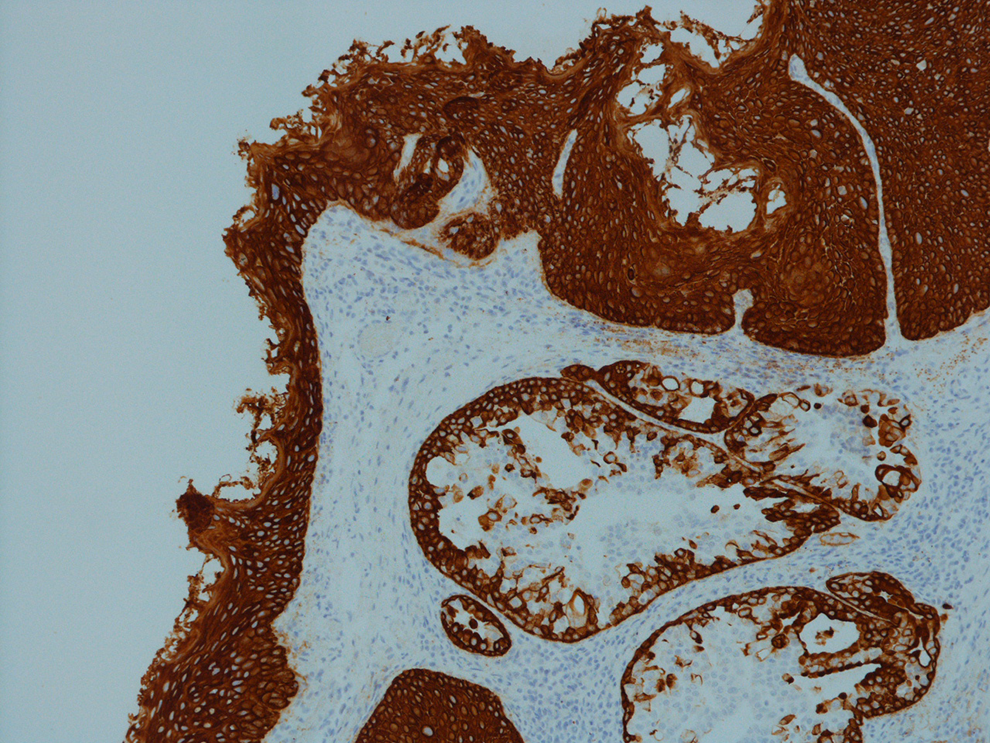
High molecular weight cytokeratins staining in both squamous and glandular components.
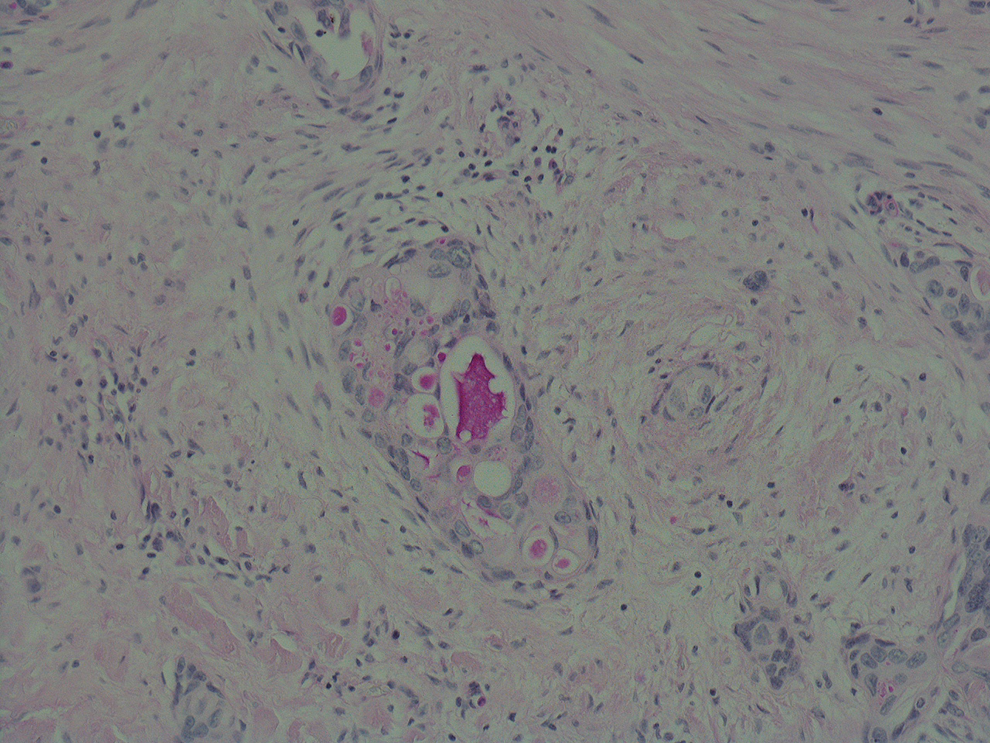
Mucin demonstrated in the glandular component using Diastase Periodic Acid Schiff (DPAS).
Discussion
Adenosquamous carcinoma is a very rare type of malignancy and is responsible for under 1% of all head and neck cancers, with fewer than 100 cases reported in the literature. 1 The larynx is the commonest site for these cancers to arise. 2 In spite of so few reported cases of laryngeal ASC, it is accepted to be a highly aggressive form of the disease, often presenting with locoregional or distant metastases. Dubal et al noted lymph node metastases in 40% of patients and distant metastases in 10% of cases they studied. 3 Subsequently, prognosis tends to be poor, with the literature suggesting median survival of less than 36 months. 3 Men in their sixth or seventh decades are most likely to be affected, with cigarette smoking and alcohol consumption along with human papillomavirus infection playing a role in the etiology of this disease. Human papillomavirus–related ASC appears to offer a more favorable prognosis. 1 Presentation is similar to other head and neck cancers with symptoms such as progressive hoarseness and dysphagia predominating. 1 Head and neck ASC was initially described by Gerughty et al in 1968 who recognized it as a distinct entity with a poor prognosis and theorized that it originated from excretory ducts of seromucinous glands 4 ; more common thinking is that the disease originates from mucosal epithelium. 5 The World Health Organization listed the histological criteria for identification of ASC of the head and neck. It is characterized by there being both adenocarcinoma and keratinizing squamous cell carcinoma. 2 Although mucin production is often seen, this is not required for the diagnosis to be made if true glands are present. There are generally features of duct-like structures with trabeculae and solid tumor nests at the tumor edge with gland formation showing punched out spaces and smooth boundaries. 2
An important differential diagnosis is that of mucoepidermoid carcinoma (MEC) that has a better prognosis than ASC. Mucoepidermoid carcinoma also demonstrates both cancer cell types but with the two components mixed together. Adenosquamous carcinoma in contrast can be identified through the separated nature of these cells, with the squamous cell carcinoma presenting as either in situ or invasive disease and the adenocarcinoma cells residing deeper within the tissue. The nature of this presentation can make diagnosis of the disease from biopsy specimens difficult, as tissue from the deeper sections of the specimen may not be retrieved. An initial diagnosis of squamous cell carcinoma may therefore be made, which might result in suboptimal therapy. Yoshimura et al reported that oral ASC was diagnosed correctly from initial biopsy specimens in only 31.6% of patients, with 36.8% of these being diagnosed as squamous cell carcinoma. 6 It is important to note that affected lymph nodes often retain both features of the disease and therefore may prove useful in establishing a diagnosis. 7
Due to its rarity, there is no consensus on the best way of managing malignancies of this type. Typically, treatment would include surgery and adjuvant radiotherapy/chemotherapy, depending on the stage. 3 There are only a handful of cases of glottic ASC published in the literature, the majority of which have been managed with open laryngectomy with or without neck dissection and/or radiotherapy. We performed a Pubmed (MEDLINE) search to identify cases of glottic ASC using the search criteria (adenosquamous ca*) AND (laryn* OR glotti* OR vocal) Filters: Full text, Humans, English. The majority of case series reviewed were concerned with head and neck or laryngeal disease as a whole, making it difficult to extrapolate information specifically regarding glottic ASC. Dubal et al identified 68 patients with laryngeal ASC from the SEER 18 database older than 40 years. 3 Thirty-two of these patients had disease affecting the glottis; however, a further breakdown of this was not given. Subsequently, we identified only 6 other cases affecting the true vocal cords where data regarding the case were separate from other laryngeal locations. Four of these were from a review by Damiani et al which classified its cases as ASC/high-grade MEC rather than purely ASC. 8 These 6 cases’ demographics, treatment, and outcomes are summarized in Table 1. Most patients were males and their average age at the time of diagnosis was 62.1 years. For the 2 patients where lifestyle was commented upon, there was a significant smoking history in both cases. Over 65% of the cases underwent laryngectomy with or without neck dissection as a definitive treatment, indicating the severity of disease as well as its late diagnosis. Fifty percent of patients died of their disease within 36 months. In conclusion, early stage ASC of the glottis can be treated successfully with a transoral approach, reserving open laryngectomy with or without neck dissection and/or radiotherapy to advanced cases. Early diagnosis is essential and this histological entity needs to be kept in consideration in case of persistent dysphonia and suspected subepithelial lesion of the vocal cord. Magnetic resonance imaging of the neck can have a role in the diagnosis and staging of submucosal lesions of the vocal cord. Mucosal biopsy is unreliable, due to the submucosal nature of the disease, leading to misdiagnosis and therefore to late diagnosis. CO2 laser excision should be preferred as first-line approach, both for diagnosis and treatment when possible. When ASC is confirmed, an extended cordectomy should be preferred to achieve oncologically safe resection margins. After transoral laser surgery, a close follow-up, including laryngoscopy and examination of the neck with or without regular repeat ultrasound of the neck, is mandatory to detect early recurrence or locoregional metastasis. This is the first documented case of ASC of the glottis being treated successfully with a transoral laser cordectomy.
Further Cases of Glottic Adenosquamous Carcinoma in the Literature.
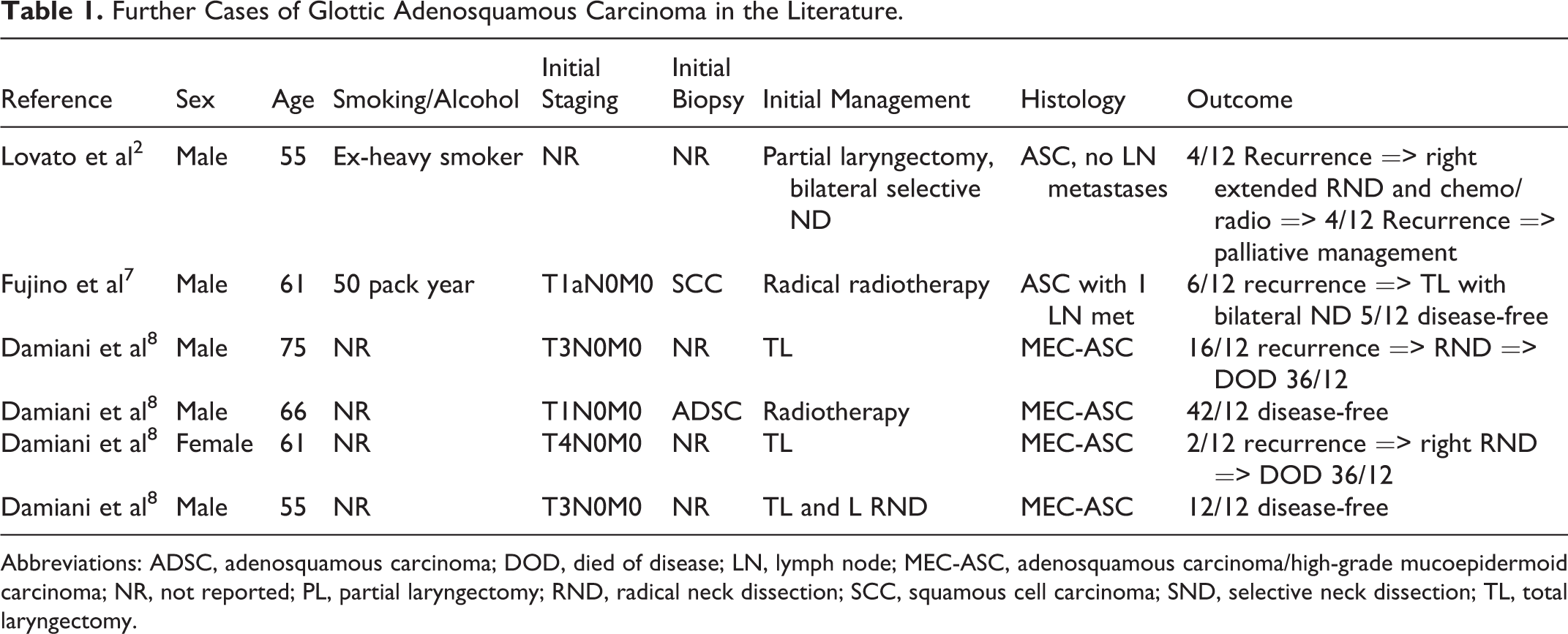
Abbreviations: ADSC, adenosquamous carcinoma; DOD, died of disease; LN, lymph node; MEC-ASC, adenosquamous carcinoma/high-grade mucoepidermoid carcinoma; NR, not reported; PL, partial laryngectomy; RND, radical neck dissection; SCC, squamous cell carcinoma; SND, selective neck dissection; TL, total laryngectomy.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for this case study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.