
Abstract
Growing skull fracture (GSF) is an uncommon post-traumatic complication, which accounts for approximately 0.05% to 1% of all skull fractures. Delayed diagnosis of GSF in adulthood is rare and often involved with a variety of neurological symptoms. Here, we reported an adult patient, with an interval of 17 years from initial head trauma to first diagnosis of GSF. The patient complained of short periods of fainting and bilateral visual hallucinations, with a hard palpable bulge around his right occipitomastoid suture region. Computed tomographic imaging demonstrated an arachnoid cyst extending into right mastoid cavity. Consequently, the delayed diagnosis of GSF was confirmed, and the patient was managed with duroplasty and cranioplasty. At the 8-month follow-up, the patient showed an uneventful postoperative recovery. A comprehensive literature review was also conducted, and a total of 70 GSF cases were identified and summarized. According to the literature review, patients with GSF generally have a history of head trauma in their childhood, and delayed diagnosis is a common situation. Diagnosis of GSF should include complete retrospective medical history, physical, and imaging examinations. Once the diagnosis is confirmed, cranioplasty accompanied with duroplasty might be the most effective way to relieve symptoms and prevent further damage.
Introduction
Growing skull fracture (GSF) is a rare post-traumatic complication, accounting for less than 1% of all skull fractures, which is commonly observed in children under 3 years of age. 1 -4 The osteodural defect resulting from head trauma gradually gets enlarged under the increasing pressure on fracture edges created by brain pulsation and herniation of intracranial tissue, which prevents them from apposition and healing. 5 -8 Since early-stage GSF usually presents with few clinical manifestations, delayed diagnosis until the development of obvious skull physical signs and neurological symptoms is a common situation. 5,9,10 In past several decades, duroplasty and cranioplasty are 2 most widely applied therapies for GSF, which have been proven to be effective in most cases. 11 -13 Here, we reported an adult patient with GSF of the temporal bone who presented with rare neurological symptoms and summarized the clinical details of 70 GSF cases identified through the literature review, with the aim of providing some evidence for adulthood GSF’s pathology, diagnosis, and principles of management.
Case Report
A 19-year-old man presented with short periods of fainting which lasted for half an hour and 1-hour bilateral visual hallucinations, without migraine, vomiting, or loss of consciousness. Physical examination only revealed a hard palpable bulge around right occipitomastoid suture region, without other abnormal neurological findings. Computed tomographic scan indicated the right mastoid cavity was substantially enlarged, of which approximately two-thirds was occupied with a soft-tissue density and likely to be connected with intracranial cavity (Figure 1A). An additional magnetic resonance imaging was performed showing locally extensive encephalomalacia with T1 and T2 prolongations, involving the right temporal lobe, occipital lobe, and cerebellum (Figure 1B-C), of which the lesion was likely to be communicating with dilated temporal angle of the right lateral ventricle. However, neither hearing test nor otoscopy showed any abnormal findings.
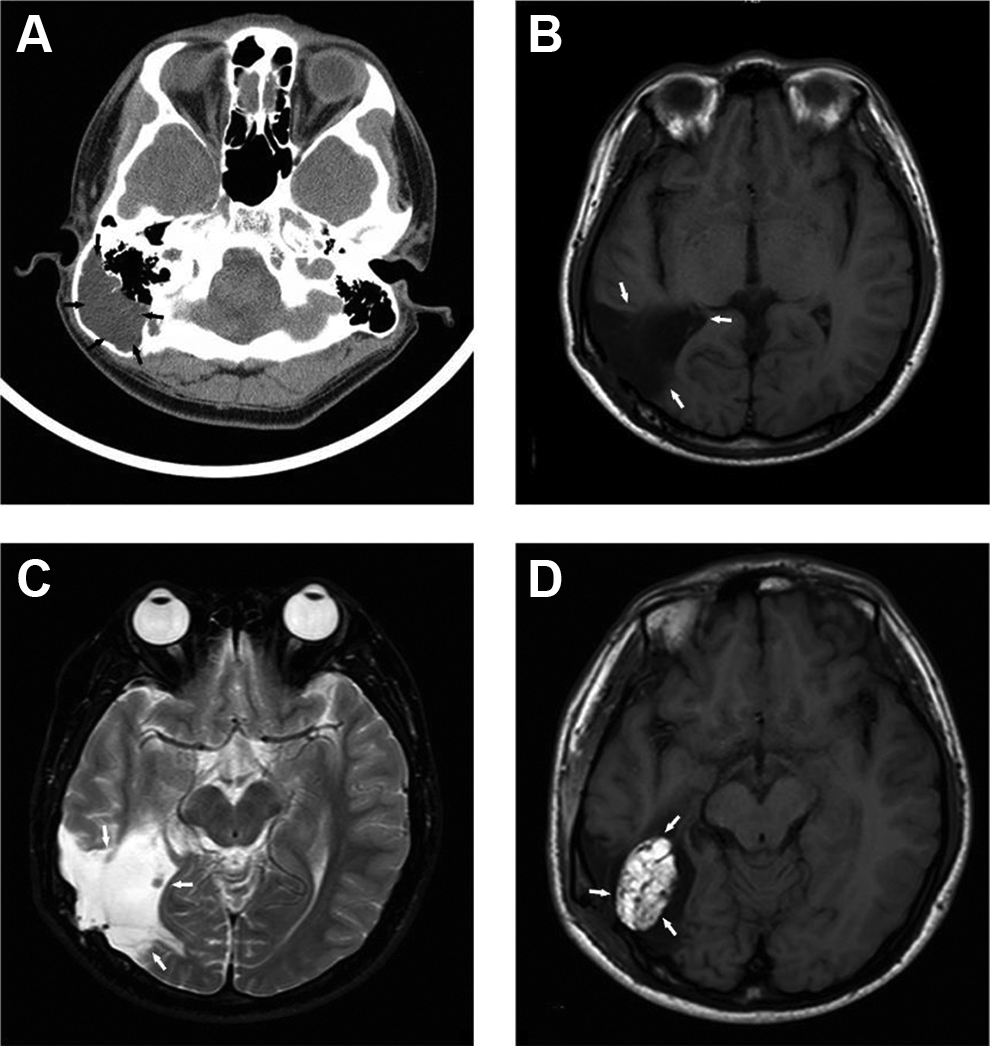
A, Preoperative high-resolution computed tomography (HRCT) scan, coronal sections of right temporal bone. Enlarged right mastoid cavity, of which approximately two-thirds were occupied with a soft-tissue density. B and C, Preoperative coronal brain magnetic resonance imaging (MRI) sections. A lesion involving temporal lobe, occipital lobe, and cerebellar hemisphere showed T1 (B) and T2 (C) prolongations with the dilated temporal angle of the right lateral ventricle possibly communicating with the lesion. D, Postoperative brain MRI (coronal section). An elliptical area with clear boundary was hyperintense on T1-weighted images, which is suggestive of the abdominal fat obliterated in the cavity.
On further questioning, the patient’s families recalled a head trauma caused by a falling brick 17 years ago. The patient lost consciousness immediately and the status lasted for 3 days without special medical intervention. After he regained his consciousness, no obvious sequelae was observed. Thereafter, he suffered from syncope twice, 1 year and 1 month before hospitalization, respectively. Both of the 2 episodes happened after playing basketball, with a short time of headache in advance (the patient couldn’t clarify the exact length of headache), accompanied with no vomiting or convulsions, and woke up with full consciousness in about half an hour without medical intervention.
The diagnosis of post-traumatic GSF and arachnoid cyst was made after complete evaluation. Subsequently, the patient underwent surgical repair of dural mater and cranium.
Under general anesthesia, a C-shaped retroauricular incision was made in the right temporal region, and the mastoid cortex was exposed. A pulsating cyst filled with clear, colorless fluid presented under the thin mastoid cortex was observed, with fluid squirting out after the cortex was opened (Figure 2A). We resected partial right skull base and obliterated the defect with abdominal fat (Figures 1D and 2B). The patient had an uneventful recovery. At the 8-month follow-up, he experienced no postoperative visual hallucinations, headache, dizziness, or syncopes, and no budging or pain were detected in his operative region.
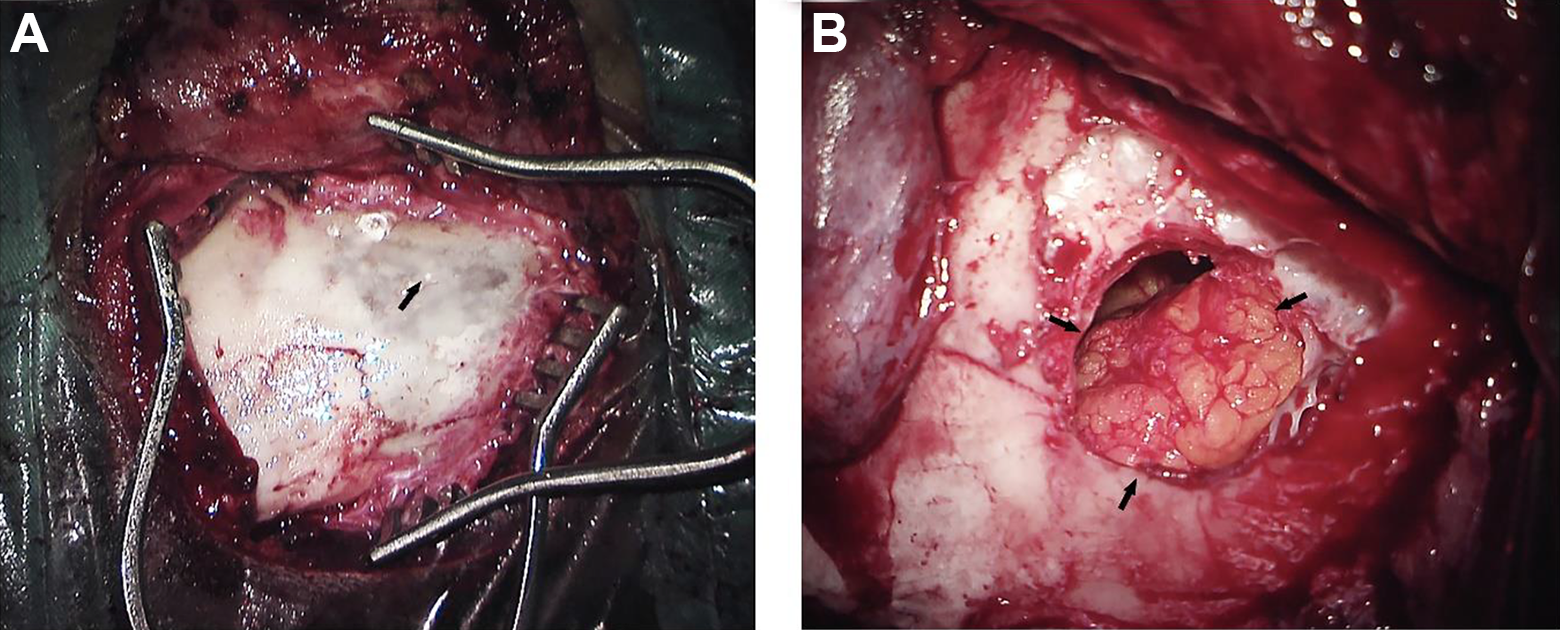
Intraoperative picture. A, Pulsatile cyst containing cerebrospinal fluid (CSF)-like fluid under the thin mastoid bone cortex was observed, with fluid squirting out after the cortex was opened. B, Closure of the cavity with abdominal fat.
Literature Review
Methods
To provide a review of previously published GSF cases, a PubMed search of the English language literature was performed from the beginning of the database through October 30, 2019. The search strategy was ((((growing skull fracture) OR growing cranium defect) OR leptomeningeal cyst)) AND ((arachnoid cyst) OR (((head) OR skull) OR brain)). We also reviewed the reference sections of all GSF case reports or series to search for additional cases and included all adulthood GSF case reports with imaging diagnosis, with the exception of head trauma due to birth injuries.
Results
We conducted a comprehensive literature review for GSF. A total of 62 literatures containing 70 post-traumatic GSF cases were identified (Table 1), with their detailed characteristics summarized in Supplementary Table 1. Approximately two-thirds of patients reported a history of head trauma under the age of 3 (n = 51, 72.9%), of which the leading cause was fall (n = 44, 62.9%), followed by vehicle accidents (n = 13, 18.6%) and child abuses (n = 3, 4.3%). Meanwhile, according to our review, parietal region was the most frequently involved location (n = 21, 30.0%), followed by parieto-occipital region (n = 9, 12.9%), parietotemporal region (n = 8, 11.4%), and occipital region (n = 7, 10.0%). Diastasis of sutures without any other bone fractures was also observed in one case. 14
Summary of Documented Clinical Details in 70 Patients With Growing Skull Fractures.
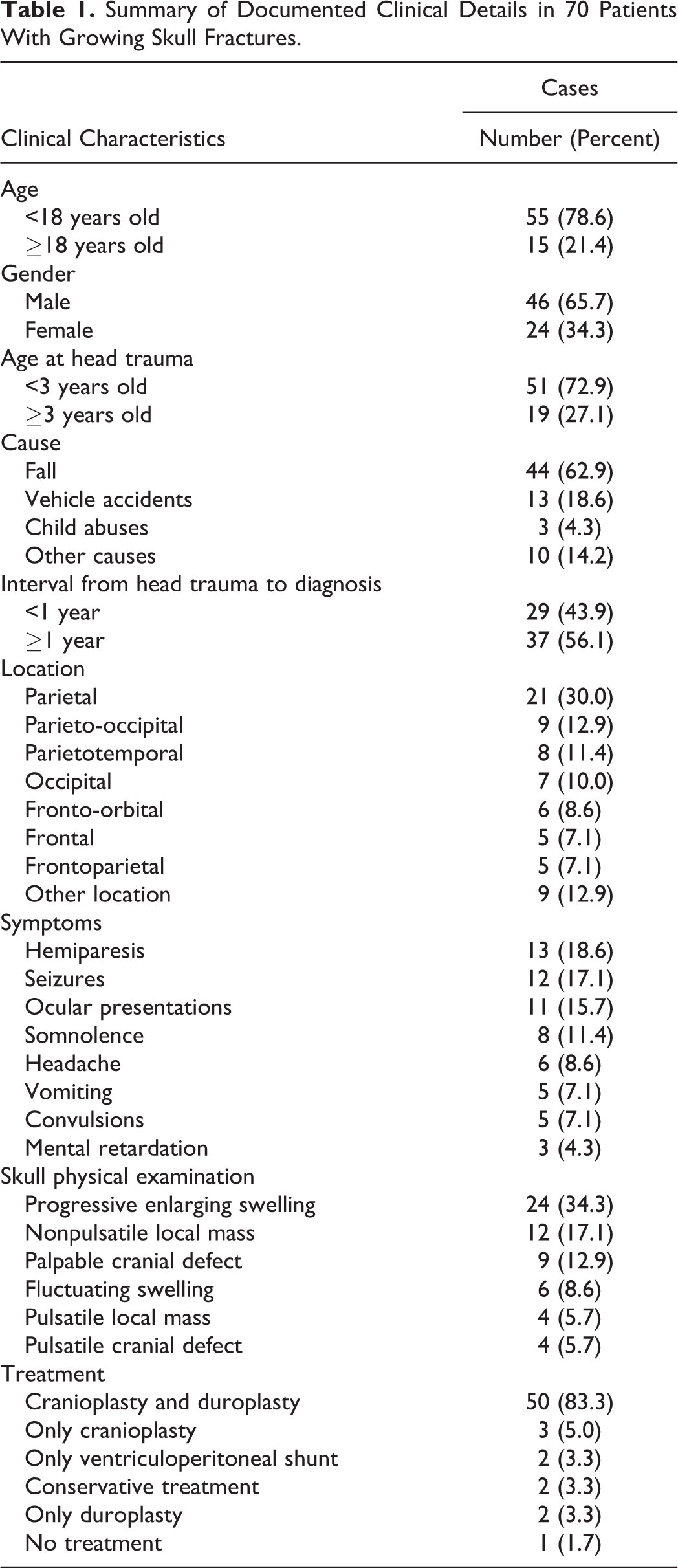
The most common physical sign was progressive enlarging swelling of scalp, accounting for over one-third of all cases (n = 24, 34.3%), followed by nonpulsatile mass (n = 12, 17.1%) and palpable cranial defect (n = 9, 12.9%). Besides, loss of consciousness immediately after head trauma occurred in over one-third of patients (n = 22, 31.4%), with the duration ranging from several minutes to more than 10 weeks. In addition, the incidence of hemiparesis and seizures accounted for 18.6% and 17.1%, respectively. Mental retardation, such as had difficulty in learning and language or presented low intelligence quotient comparatively, was reported only in 3 cases. 15 -17
More than half of those reported GSF patients received delayed diagnosis or underwent surgical management over 1 year following head trauma (n = 37, 56.1%), ranging from 2 weeks to 54 years. Meanwhile, the most common characteristics in those delayed GSF images revealed cysts filled with cerebrospinal fluid (CSF) extending through skull defects (n = 25, 40.3%), herniation of brain tissue (n = 14, 22.6%), focal ventricular dilatation (n = 13, 21.0%), and porencephalic cysts (n = 10, 16.1%), respectively. About 83.3% (n = 50) GSF patients would receive cranioplasty and duroplasty.
Discussion
The incidence of GSF is less than 1% in all skull fractures. 1 It mostly occurs in patients during their infancy and early childhood (1-3 year olds), as they are more likely to suffer from falling injuries and child abuse. 1 -4,18 The pathophysiological mechanisms of GSF remains elusive. It is widely believed that rapid brain growth and post-traumatic skull defects accompanied by dural tear are necessary for the formation of GSF. The increasing pressure on fracture edges created by brain pulsation and herniation of intracranial tissue would prevent them from apposition and healing. 5,6,8,11,12,19 In consistent with previous studies, 20,8 we don’t think the intracranial expansive force of CSF cyst can result in elevated intracranial pressure unless there was hydrocephalus (in our literatures review, such cases or speculation were not reported) because in the course of GSF, skull will accordingly enlarge. And surgical repairment of dura matter and cranium is the most widely applied treatment.
To the best of our knowledge, the present case is the first to report GSF patient presented with short periods of visual hallucinations and syncopes, with an arachnoid cyst herniation projecting into his right mastoid cavity, due to a head trauma happened as long as 17 years ago. Our case highlighted the importance of taking a thorough history and performing a complete examination when the patient manifested with rare neurological symptoms (such as visual hallucination and postexercise syncope).
Supplemental Material
Supplementary_Table1_Revised - Growing Skull Fracture of Temporal Bone in Adults: A Case Report and Literature Review
Supplementary_Table1_Revised for Growing Skull Fracture of Temporal Bone in Adults: A Case Report and Literature Review by Xiao-hong Yan, Ke Qiu, Yan Gao, Jianjun Ren, Danni Cheng, Wendu Pang, Yao Song, Wen Yang, Rong Yu and Yu Zhao in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
Xiao-hong Yan and Ke Qiu contributed equally to this study and share first authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 1·3·5 project for disciplines of excellence–Clinical Research Incubation Project, West China Hospital, Sichuan University [Grant No. 2019HXFH003]; Key Research and Development Support Programmes of Chengdu Science and Technology Bureau [Grant No. 2018-YFYF-00123-SN]; and the Fundamental Research Funds for the Central Universities [Grant No. 2012017yjsy118].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.