
Abstract
Amyloidosis is a heterogeneous group of diseases characterized by the extracellular deposition of insoluble proteins whose pathogenesis is not yet fully understood. The deposition of amyloid proteins can be systemic or localized, idiopathic or related to systemic diseases, mostly multiple myeloma or chronic inflammatory diseases. Localized head and neck amyloidosis is a rare entity, mainly involving the larynx. Given the rarity of the disease and the absence of a lasting follow-up protocol, there is no standard treatment defined for localized amyloidosis. We report a rare case of localized nasopharyngeal amyloidosis, treated with complete transoral resection and confirmed by histological examination.
Introduction
Amyloidosis is a heterogeneous group of diseases characterized by the deposition of insoluble proteins in the extracellular space. The deposition of amyloid proteins can be systemic or localized. 1,2
The systemic form can be idiopathic or related to systemic disease, mainly multiple myeloma or chronic inflammatory diseases. Localized nasopharyngeal amyloidosis is an extremely rare entity with few cases reported in the literature.
Amyloidosis can be suspected based on clinical signs and imaging studies but the definitive diagnosis requires tissue biopsy, analyzed using Congo red staining combined with polarized light and possibly immunohistochemical characterization of the proteins. There is no specific cure for amyloidosis and treatment depends on the form of the disease, the organs affected, and the underlying condition. We describe a case of an 80-year-old woman with a primary localized nasopharyngeal amyloidosis.
Case Report
An 80-year-old woman presented with a 5-month history of progressive nasal obstruction. The patient had undergone right superior lobectomy for primitive lung adenocarcinoma and hystero-salpingo-oophorectomy for endometrial carcinoma. On admission to our department, there was no evidence of recurrent disease.
Endoscopy revealed a yellowish smooth bulging mass involving the posterior wall of the nasopharynx (Figure 1). Maxillofacial magnetic resonance imaging showed a submucosal mass (26 × 14 × 43 mm) involving the posterior wall of the nasopharynx, characterized by polycyclic margins, homogeneous contrast enhancement, isointensity with muscles in T1 and T2 acquisitions, and hyperintensity in Short-TI Inversion Recovery images, without infiltrative aspects (Figure 2). A total body computed tomography (CT) scan showed no other solid lesions. The nasopharyngeal mass had inhomogeneous contrast enhancement and was accompanied by 2 retropharyngeal nodes.

Endoscopy revealed a yellowish smooth bulging mass involving the posterior wall of the nasopharynx.
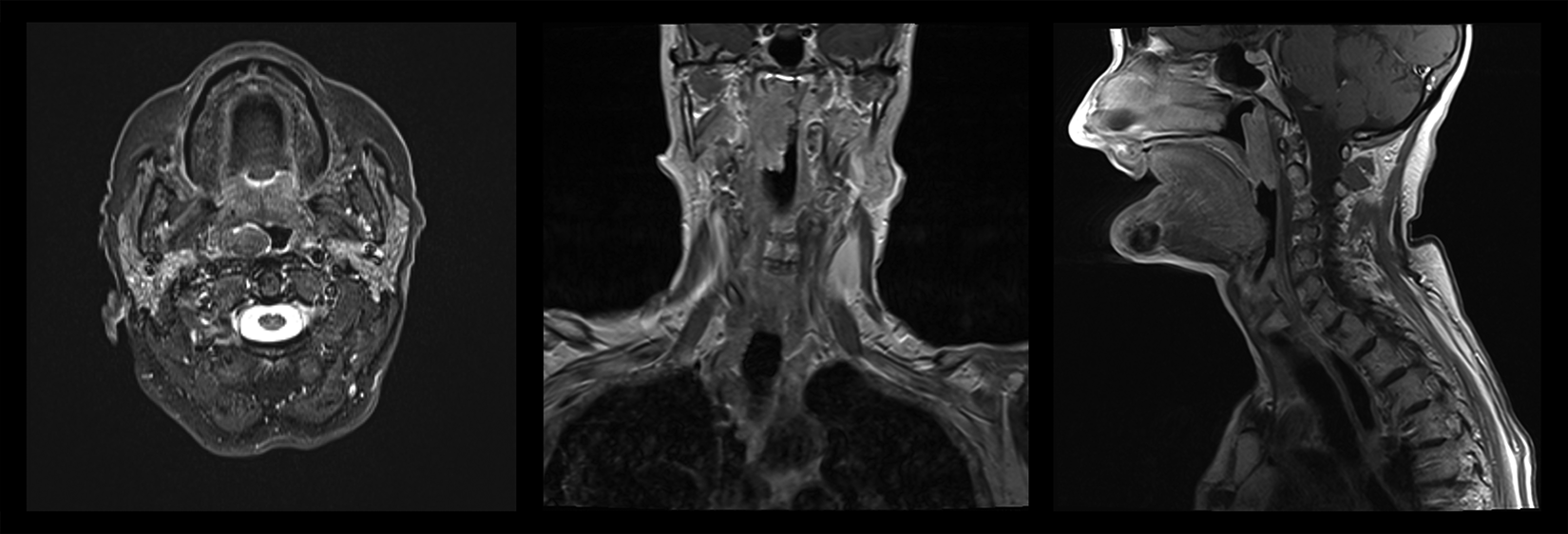
Maxillofacial magnetic resonance imaging showed a submucosal mass (26 × 14 × 43 mm) involving the posterior wall of the nasopharynx, characterized by polycyclic margins, homogeneous contrast enhancement, isointensity with muscles in T1 and T2 acquisitions, and hyperintensity in Short-TI Inversion Recovery (STIR) images, without infiltrative aspects.
Considering the radiologic features, the poor vascularization and the distance from the large neck vessels, a complete transoral resection was carried out. The surgical specimen was routinely processed. The postoperative period was uneventful.
Microscopic examination revealed a submucosal deposition of cloudy, ill-defined pinkish material highly suspicious for amyloid deposition (Figure 3). Specific Congo red staining was performed and revealed apple-green birefringence under polarized light (Figure 4). Multiple attempts were made to further characterize the type of amyloid proteins using immunohistochemistry but with negative results, thus a diagnosis of nasopharyngeal amyloid deposition, unspecific type, was made.
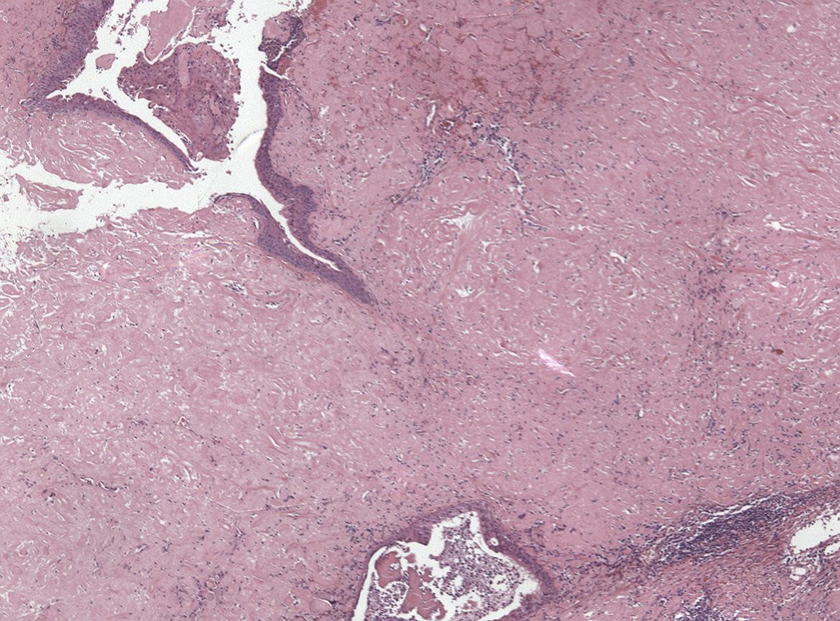
Microscopic examination revealed a submucosal deposition of cloudy, ill-defined pinkish material highly suspicious for amyloid deposition.
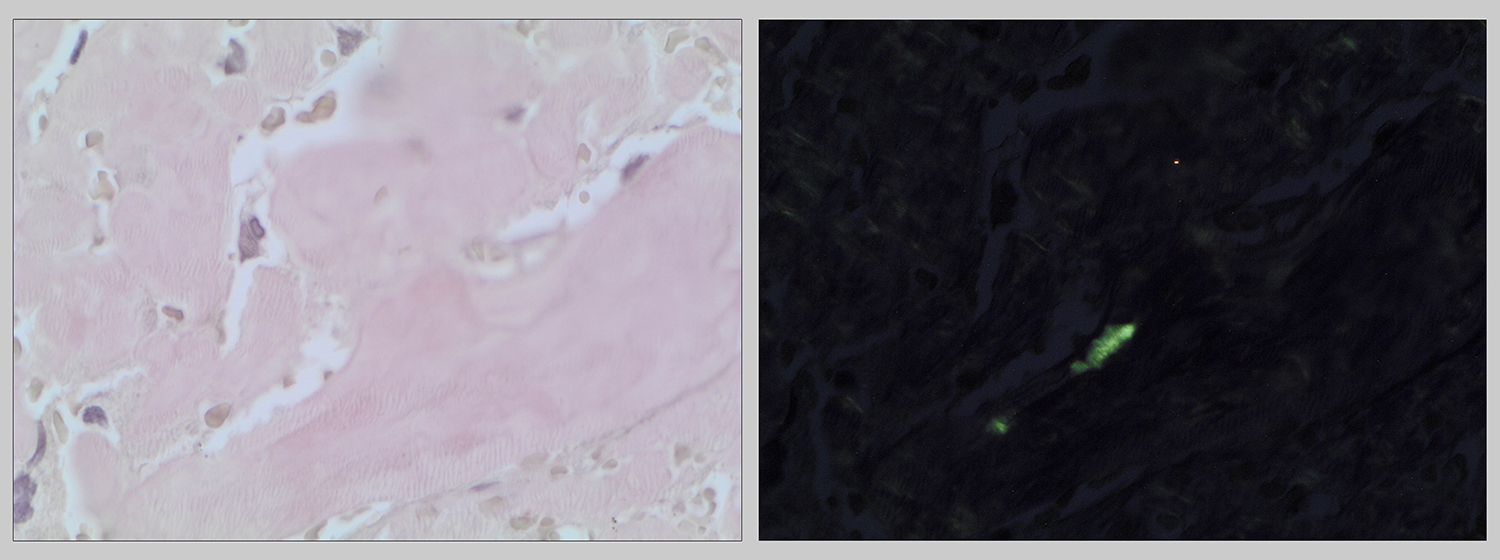
Congo red staining (left, clear light, OM 40×) revealed apple-green deposits under polarized light (right, OM 40×).
Consequently, a complete work-up was performed, ruling out systemic involvement and conditions possibly related to a secondary form of amyloidosis. A diagnosis of localized nasopharyngeal amyloidosis was then postulated. Twenty-four months after surgery, our patient is in good condition and disease-free, undergoing regular clinical endoscopic and radiological follow-up.
Discussion
Amyloidosis is a rare clinical entity, characterized by the extracellular deposition of proteinaceous material comprised of various abnormal proteins known as amyloid fibrils. 3 Amyloid deposits result from a soluble precursor protein which is misfolded resulting in the deposition of insoluble amyloid fibrils. 4 Amyloidosis is defined as localized if the amyloid deposition is limited to the tissue where its precursor protein is produced, and as systemic if the precursor protein is produced in a certain part of the body and thereafter transported to the site where the amyloid is found. 5
The modern classification of amyloidosis uses an abbreviation of the predominant protein, preceded by the letter A. Among the systemic forms, there are immunoglobulin light chain amyloidosis (AL), acute phase protein amyloidosis (AA), dialysis-related amyloidosis (Aβ2M, β2 microglobulin), and age-related amyloidosis (ATTR, transthyretin).
Microscopically, amyloidosis is characterized by deposition of ill-defined pink material. In the localized form, a plasma cell infiltrate is described. 6 Congo red staining confirms the amyloid nature with a classic apple-green birefringence. Immunohistochemistry with commercially available antibodies should be performed in order to characterize the protein component.
Clinical presentation depends on the organs affected by the deposit. The kidneys are frequently involved in AL amyloidosis and this can lead to kidney failure; the same loss of function can affect the heart or lungs. In the head and neck region, the most frequent symptoms are hoarseness and dyspnea in laryngeal forms, or macroglossia in cases with oral cavity involvement. 6
The prognosis of the AA form depends on the condition responsible for the amyloidosis itself. The AL amyloidosis can be treated with chemotherapy and stem cell transplantation; on the other hand, the AA form is treated aiming to cure the underlying disease. Localized amyloidosis in the head and neck region is rare. Most cases reported have been described in the larynx (60%), oropharynx (23%), trachea (9%), orbit (4%), and nasopharynx (3%). 7 -9
Nasopharyngeal amyloidosis is extremely rare. In their review in 2007, Panda et al described only 13 cases in over 70 years of activity (1935-2007). 10 Lately, there has been an increase in the number of reported cases, perhaps due to improvements in endoscopic and radiologic diagnostic tools. 11,12
Patients with nasopharyngeal amyloidosis mainly complain of nasal obstruction, epistaxis, posterior rhinorrhea, and hearing impairment. 13 Endoscopy generally shows an irregular, heterogeneously yellowish, smooth bulging mass. 14 On CT scan, these lesions usually appear as a well-defined, homogenous, smooth soft tissue mass without evidence of bony erosion. 15 It has also been reported to mimic slow-growing tumors and sometimes to appear as densely calcified lesions. 16
Imaging can help to define the extent of the disease but there are no characteristic imaging findings, so the diagnosis cannot be made without a biopsy or excision. 17,18 Diagnosis is then confirmed by histopathology, with characteristic apple-green birefringence on microscopy using Congo red staining combined with polarized light.
Given the rarity of the disease and the absence of a lasting follow-up protocol, no standard treatment has been defined for localized amyloidosis. Treatment of local disease is by complete excision when this is possible without significant anatomical or functional sequelae, followed by routine surveillance for recurrence. Clinical follow-up is by endoscopic examination, supported by imaging when a recurrence is suspected, based on signs and symptoms.
At present, there is no evidence in the literature suggesting a progression from nontreated localized head and neck amyloidosis to systemic disease. 19 Thus, at present, there is an ongoing debate between surgical excision, preferred when the disease causes morbidity, and a wait-and-see approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript was funded by the Regione Piemonte AD FUNCTIONEM (years 2015–2018); FPRC 5xmille 2016 Ministero della Salute Progetto ARDITE; Fondi Ricerca Corrente 2018, Ministero della Salute.