
Abstract
Objectives:
To discuss the indication for performing a mastoidectomy with catheter placement in patients with chronic tympanostomy tube otorrhea.
Methods:
The Medical Literature Analysis and Retrieval System Online was searched via PubMed for relevant articles using serous mastoiditis, mastoidectomy, chronic otorrhea, tube otorrhea, tympanostomy tubes, and biofilm as keywords.
Results:
Further understanding of the pathophysiology of otorrhea and the development of ototopical fluoroquinolones have made a draining tympanostomy tube more manageable. Nevertheless, chronic otorrhea refractory to an otolaryngologist’s traditional treatment algorithm still occurs and may benefit from a mastoidectomy with antibiotic irrigation using a catheter in certain cases. We theorize that resolution of otorrhea results from this technique by decreasing the burden of diseased mucosa and providing a larger concentration or dose of antibiotic to the middle ear cleft through the antrum. High-resolution images of the technique and catheter placement are included in this review.
Conclusions:
Despite being an uncommon management strategy, the literature suggests an indication for performing a mastoidectomy in a small percentage of patients with a chronically draining tympanostomy tube.
The advent of tympanostomy tubes (TTs) in the 19th century by Politzer came with a burdensome consequence: postoperative tympanostomy tube otorrhea. As Coates writes, this common sequelae resulted in the abandonment of grommet tubes until they reemerged in the 1950s and were popularized by Armstrong. 1 Today, further understanding of the pathophysiology of otorrhea and the development of ototopical fluoroquinolones has made a draining TT more manageable. Nevertheless, chronic otorrhea refractory to an otolaryngologist’s treatment algorithm still occurs and may benefit from a mastoidectomy with antibiotic irrigation using a catheter in certain cases. We theorize that resolution of otorrhea results from this technique by decreasing the burden of diseased mucosa, and providing a conduit for a larger concentration or dose of antibiotic to be delivered to the middle ear cleft via the antrum. This review will discuss our management strategy in chronic tube otorrhea and when mastoidectomy has been indicated for select patients.
Intubated tympanic membranes do commonly drain with an overall rate of 17%. 2 The etiology may in part depend on the duration and type of tube, as well as the chronicity of drainage, which can be further classified as postoperative, acute recurrent, or chronic. Most practitioners define acute otorrhea lasting less than 6 weeks and chronic drainage persisting beyond a 6 to 8 week time period. 3,4 A meta-analysis by Kay et al. reported that 16% of patients will have transient otorrhea in the early postoperative period and 26% of patients will experience drainage at some point during the lifetime of the tube. Rates for recurrent acute and chronic otorrhea, while uncommon, occurred in 7.4% and 3.4% of patients, respectively. 2
Traditional management of recurrent acute otorrhea is often successful with instillation of antibiotic drops and addressing exacerbating factors for otitis media with effusion, such as allergies, inhalational irritants, adenoid hypertrophy, or granulation tissue surrounding the tube. 5,6 Chronic otorrhea presents a much more challenging dilemma, and despite its low incidence, myringotomy with TT placement holds the title as one of the most common ambulatory procedures; over 600,000 are performed annually in children in the United States alone. 7 Thus, clinicians inevitably will have to manage this outcome and necessitates a treatment paradigm.
In our practice, which primarily consists of adults, patients often have been treated unsuccessfully by the referring otolaryngologist with topical fluoroquinolone drops and oral antibiotics. Aural toilet is performed and a culture of the drainage is taken to guide antimicrobial selection for bacterial or fungal pathogens. Treatment with sulfacetamide/prednisolone or tobramycin/dexamethasone drops, along with a discussion on the risks and complications of aminoglycosides, are typically attempted 3 times a day for 1 week. If drainage does not abate, the tube is removed and the drum is allowed to heal. At follow-up, the tube is replaced if the effusion returns. A mastoidectomy with catheter placement is then recommend at this juncture to remove any pathologic mucosa and presumed blockage of the mastoid antrum. This management strategy entails at least a few months of evaluation. We typically perform the procedure 1 to 2 times annually as a final step in the treatment plan and, anecdotally, have achieved long-term resolution in the majority of cases. Despite being an unconventional management strategy, this relatively low-risk surgical approach is favored over administering intravenous antibiotics, which often requires a peripherally inserted central catheter and its associated risks of thrombosis and infection. 8
One hypothesis for the procedure’s efficacy is that the location of persistent pathology does not just reside in the middle ear. If the mastoid air cell system becomes a significant factor in the chronically draining TT, several issues become apparent in managing this. Although topical fluoroquinolones can reach concentrations in the middle ear that are significantly greater than that of systemic oral antibiotics, delivery and dose to the mastoid may be limited by the size of the tube or antral obstruction from inflamed mucosa. 9 In 1969, Sheehy was among the first to propose that the etiology for a chronically discharging tube could originate from the mastoid. 10 This condition, termed chronic serous mastoiditis, was a “clinical syndrome of uncertain etiology, the one and only characteristic feature of which is persistent discharge through a ventilation tube inserted for the treatment of serous otitis media.” He encountered 12 patients over an 8-year period where tube otorrhea (with median duration of symptoms of 1 year) was refractory to antibiotics, and the repeated removal and replacement of a grommet weeks later resulted in persistent serous or mucoid drainage. While initially skeptical, he believed that this condition resulted from changes in the mastoid due to a secretory mucus membrane and, after reading earlier reports from Goodhill and Brockman, advocated for a cortical mastoidectomy as treatment. 11,12 This resulted in long-term resolution of the otorrhea in 4 of 6 patients in the series who underwent mastoidectomy.
Current understanding in the pathophysiology of acute recurrent and chronic otorrhea has now focused on the role of bacterial biofilm development in both the middle ear and on TTs. Biofilms, defined as a consortium of bacteria acting in a cooperated fashion, remain adherent and embed to other tissues through the production of an extracellular matrix consisting of proteins, lipids, polysaccharides, and DNA (collectively referred to as extracellular polymeric substances). 13 It is thought that the presence of biofilms allows microorganisms to survive at a low metabolic rate, at times avoiding detection, and still contributing to pathologic responses from the middle ear. 14 And while they have been implicated, no studies to date have documented the presence of biofilms in the mastoid specifically for TT otorrhea. If they are an etiologic factor, however, eradication from the mastoid may be difficult to treat medically as biofilms are relatively resistant to topical and even intravenous antibiotics. 13
Since Sheehy’s case series, reports on outcomes of mastoidectomy for chronic tube otorrhea are scarce; the most recent series by Newburgh was in 1981. 15 However, we do not believe mastoidectomy to be outdated in these circumstances, and still find it indicated for select patients with chronic otorrhea who have failed medical management, and other treatment options or etiologies, including cholesteatoma and cerebrospinal fluid leak, have been exhausted or ruled out. Unlike the original descriptions, the contemporary practice includes placing a rubber catheter in the antrum to permit antibiotic irrigation.
The procedure begins with removal of the mastoid cortex. Intraoperative findings typically include a sclerotic mastoid with thick and inflamed mucosa (Figure 1A and B). After completion of the mastoidectomy through Koerner's septum, a red rubber catheter sutured to an intravenous Luer-Lock connector is prepared (Figure 2) and inserted into the antrum (Figure 3). It is then tunneled subcutaneously to exit posterosuperiorly to the incision and secured with a drain stitch (Figure 4). The myringotomy tube is removed and replaced. Mastoid to middle ear ventilation (and elimination of antral blockage) should be checked by flushing the catheter with saline and visualizing it coming out of the tube. Patients are sent home and instructed to irrigate the catheter daily with 1 mL of antibiotic drops until their 1 week follow-up, at which time the drain can be removed.
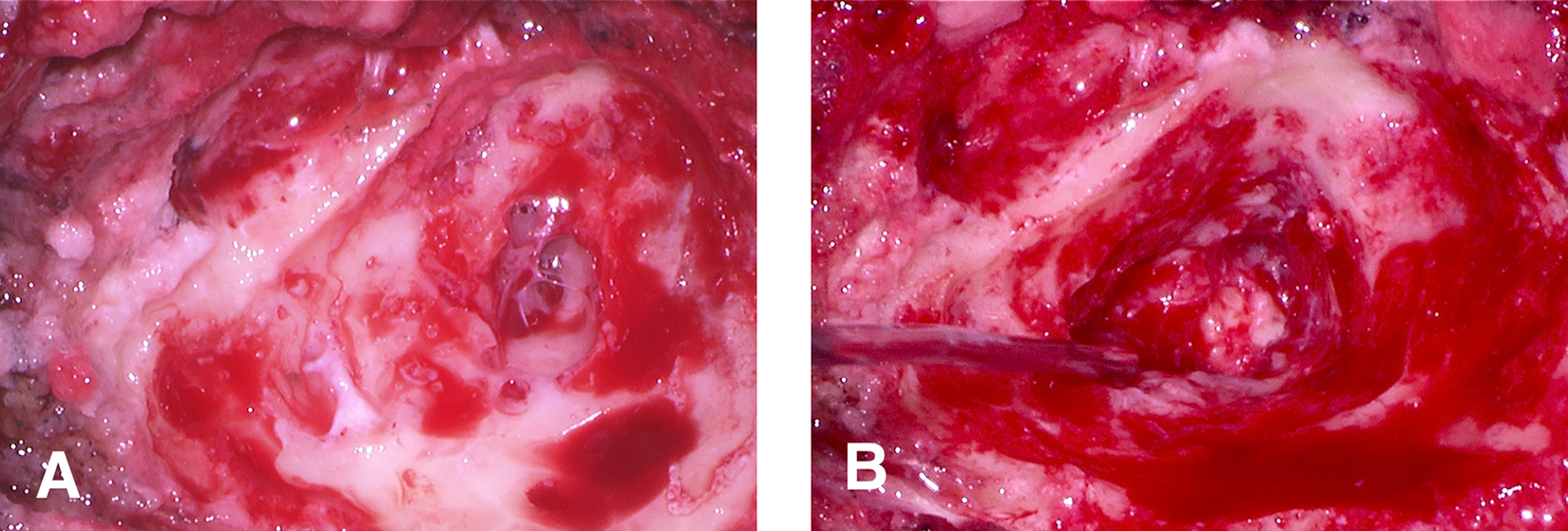
Intraoperative view following immediate removal of the mastoid cortex in a left ear (A), and opening of Koerner’s septum (B). A sclerotic bloody mastoid with thick and inflamed mucosa is typically seen.
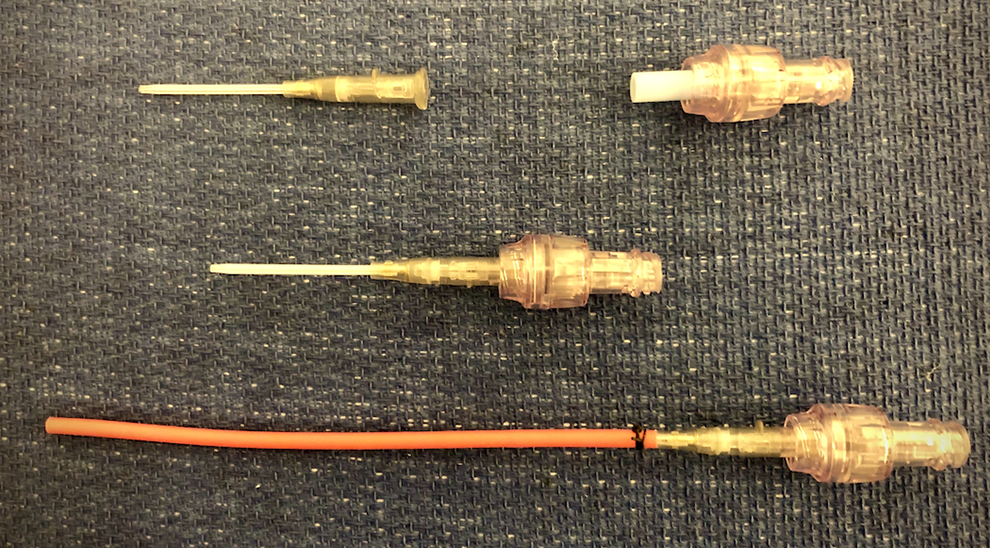
Stepwise illustration of how an 8-gauge red rubber catheter is attached to a 16-gauge angiocatheter and Luer-Lock connector with suture.
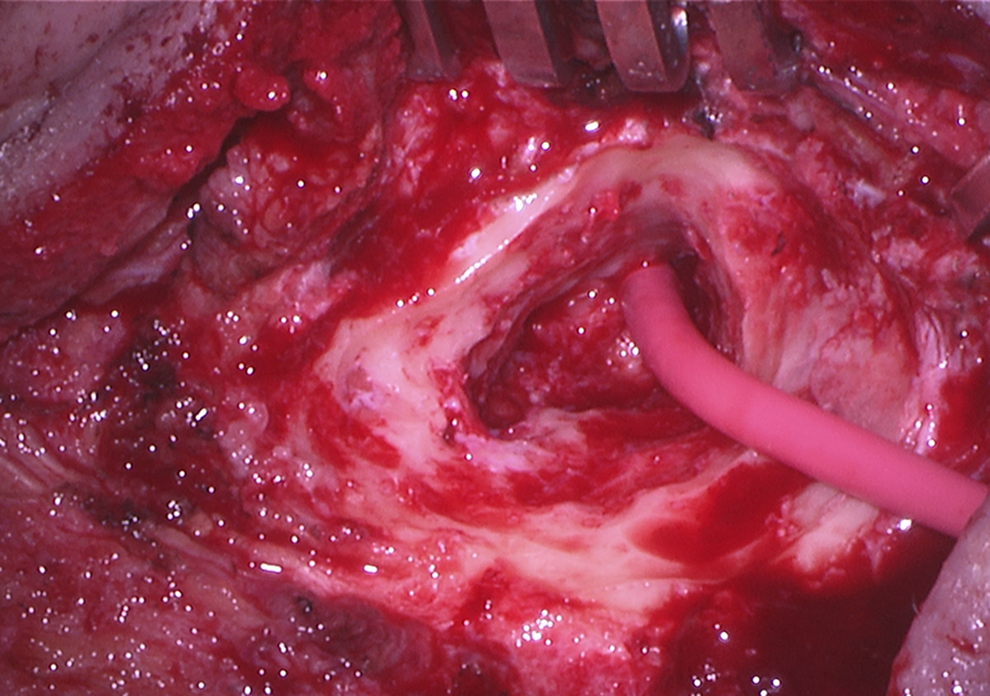
Placement of the catheter into the antrum to allow for mastoid and middle ear instillation of antibiotic drops.

The catheter should exit through a drain hole posteriorly and superiorly to the incision to allow for gravity dependent irrigation. It can then be secured to the skin with a drain stitch.
Admittedly, both recent and larger studies are currently lacking in reporting outcomes for patients undergoing mastoidectomy for draining ventilation tubes, and evaluating its efficacy compared to the use of intravenous antibiotics. Given the infrequency of the procedure, this will likely require multi-institutional efforts. Moreover, research is required to investigate whether biofilms are infiltrating the mastoid air cell system itself, and if mastoidectomy with antibiotic irrigation can result in biofilm elimination, particularly when the middle ear mucosa is not being surgically addressed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.