
Abstract
Objective:
To investigate the feasibility and the outcomes of transoral laser CO2 microsurgery (TLM) for resection of early-stage squamous cell carcinoma (SCC) of the vocal folds through several additional surgical procedures and tips improving the glottic exposure.
Methods:
Retrospective chart review of patients treated by TLM cordectomy in a single European University Hospital for early-stage vocal fold SCCs (Tis, T1a, T1b, and T2). The following TLM outcomes were studied regarding the tumor size (Tis and T1a vs T1b and T2) and the margin status (negative vs positive/suspicious): patient position; type of laryngoscope; requirement to external counter pressure; resection of supraglottic structures (eg, ventricular band, epiglottic petiole, and suprahyoid epiglottis); pre- and postoperative complications; overall survival; disease-specific survival (DSS); and disease-free survival (DFS).
Results:
A total of 148 patients were included. The TLM was realized in 95.3% of cases. External counter pressure, partial, or total vestibulectomy were necessary in 65.9%, 57.4%, and 4.2% of cases, respectively. A resection of the epiglottic petiole was required in 24.8% of cases. The realization of both epiglottis petiole resection and vestibulectomies were significantly higher in patients with T2 and T1b SCCs compared to those with T1a and Tis SCCs (P = .01). Different procedure tips were described for improving the laryngeal exposition. The 5-year laryngeal preservation rate, DSS, and DFS were significantly better in patients without SCC involvement of the anterior commissure, and did not vary according to the margin status. The laryngeal exposure difficulties did not impact the margin status.
Conclusion:
The exposure of glottis is possible in 95% of cases of early-stage vocal cord SCC but requires the use of several additional surgical procedures, especially for anterior commissure SCCs. The SCC involvement of the vocal fold anterior commissure is associated with lower DSS, DFS, and laryngeal preservation rate.
Introduction
Transoral laser CO2 microsurgery (TLM) is a well-used surgical approach for the treatment of early glottic squamous cell carcinoma (SCC). Transoral laser CO2 microsurgery is safe, effective, and associated with excellent locoregional control, overall survival (OS), and disease-free survival (DFS). 1 -5 Many factors may substantially impact the success of TLM such as the ability and experience of surgeon, the location and extension of cancer, and the laryngeal exposure. An optimal laryngeal exposure during TLM is fundamental to allow an adequate resection of early-stage glottic SCCs. To date, only a few papers have described the key factors associated with good glottic exposure. 6 -8 From a theoretical standpoint, an adequate glottic exposure would provide better tumor resection and postoperative survival outcomes. However, the impact of glottic exposure on survival outcomes and the related additional surgical procedures improving the glottic exposure have not been extensively investigated through clinical studies. The aim of this study was to investigate the feasibility and the outcomes of TLM for resection of early-stage SCC of the vocal folds through several additional surgical procedures and tips improving the glottic exposure.
Materials and Methods
The local ethics committee approved the study protocol (HEGP-APHP 2014) and the informed consent was obtained for all patients.
Setting and Patients
Authors reviewed the database of patients treated for early-stage glottic SCC in the European Hospital Georges Pompidou (Assistance Publique Hôpitaux de Paris, AP-HP, Paris, France) from January 2007 to November 2014. Patients benefited from TLM or partial laryngectomy for Tis, T1a, T1b, or selected T2 glottic carcinoma. Patients previously treated for laryngeal SCC, those with a history of cervical radiotherapy or laryngeal surgery were carefully excluded.
Surgical Approach
Transoral laser CO2 microsurgeries were performed according to the usual surgical procedures, which are well-described in a previous paper. 9 The type of TLM cordectomy was classified regarding the European Laryngological Society Classification (I-VI). 10,11 In case of inability to expose glottic SCC, patients benefited from partial laryngectomy; the type of laryngectomy depending on the tumor location and extension.
Surgical and Survival Outcomes
For TLM technique, the following outcomes were analyzed: patient position; factors for improving the exposure (external counter pressure and resection of supraglottic structures such as false vocal fold(s), petiole of the epiglottis, and suprahyoid epiglottis); and pre- or postoperative complications (tooth trauma, subcutaneous emphysema, and tracheotomy). The total vestibulectomy was defined as the resection of the entire ipsilateral ventricular band, whereas a partial vestibulectomy corresponded to a partial resection of the ventricular band. Five-year DFS, disease-specific survival (DSS), OS, and laryngeal preservation rate were assessed.
Statistical Analysis
Statistical analyses were performed with Statview software (version 5.0; SAS Institute, Inc, Cary, NC). The postoperative outcomes were analyzed through a comparison between 2 groups of patients: patients with Tis and T1a (group A) and those with T1b and T2 (group B) glottic SCC. Moreover, authors compared patients according to the margin status. Margins were classified as “negative” when greater than 0.5 mm, “positive” when the tumor invaded the resection margin, and “suspicious” when the margins were clear but with a tumor located at ≤0.5 mm. Patients with positive or suspicious surgical margins were compared to those with negative margins. With regard to the data distribution, the Mann-Whitney U test was used for the group comparison. Linear regression was used for exploring the potential associations between OS, DFS, DSS and the margin status of patients. A P value <.05 was considered as significant.
Results
The data of 148 (19 women and 129 men) patients were extracted. The mean age of patients was 64 years (32-84 years). The same surgeon (S.H.) performed 141 TLM and 7 “open” partial laryngectomies, including 2 vertical and 5 supracricoid partial laryngectomies. The tumor stage distribution was 34 dysplasia or cTis, 79 cT1a, 17 cT1b, and 11 cT2. Patients who benefited from open partial laryngectomies had cT1a (n = 2), cT1b (n = 2), and cT2 (n = 3) glottic SCC. All patients had N0M0 SCC. The following types of cordectomy were performed: type I (n = 33), type II (n = 26), type III (n = 35), type IV (n = 5), type Va (n = 32), type Vb (n = 1), type Vc (n = 2), and type VI (n = 7). The characteristics of the cohort according to the group analyses are described in Tables 1 and 2.
Technical Tips and Tricks to Improve Glottic Exposure.
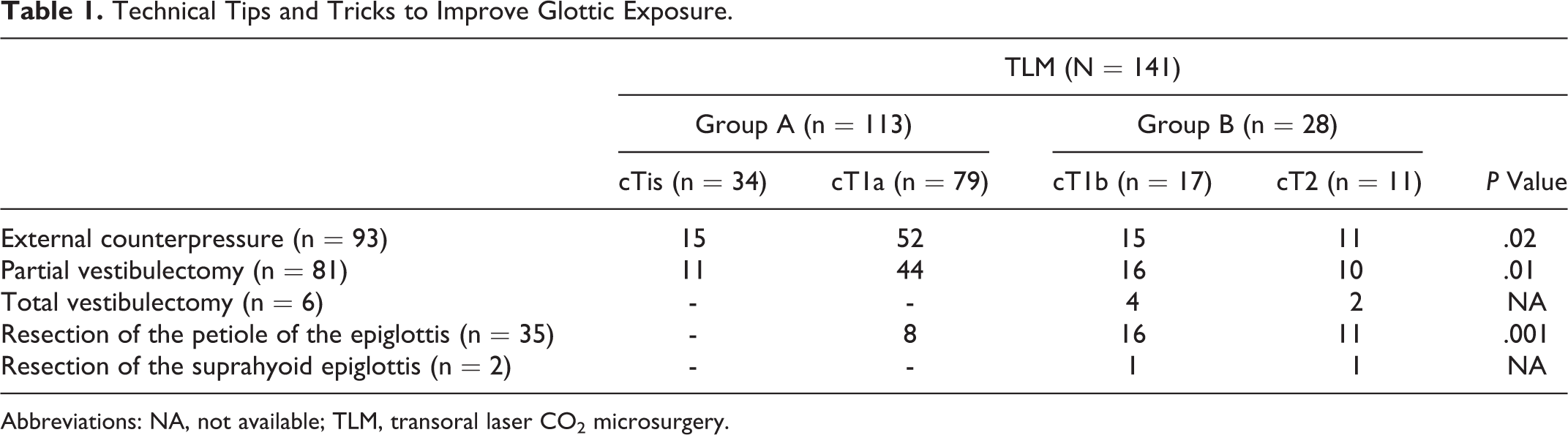
Abbreviations: NA, not available; TLM, transoral laser CO2 microsurgery.
Marge Status.
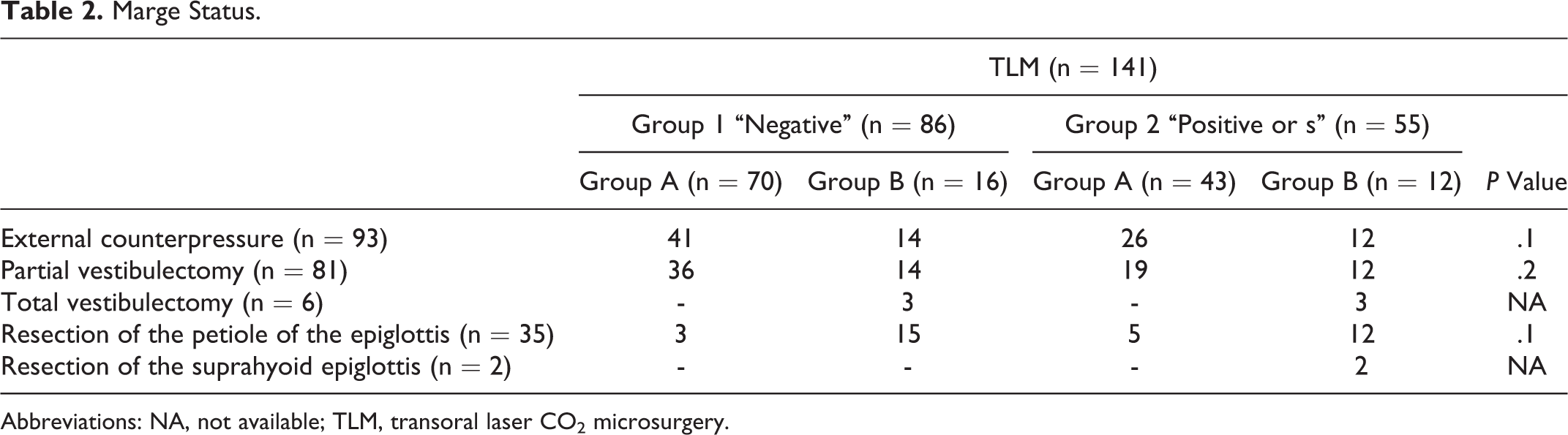
Abbreviations: NA, not available; TLM, transoral laser CO2 microsurgery.
Surgical Outcomes
The TLM was not performed regarding hypertrophic base of tongue with flaccid epiglottis in 2 patients (both T1a tumor), these patients benefiting from vertical partial laryngectomy. Five patients with T1b (n = 2) or T2 (n = 3) tumor of the anterior commissure and exposure inability benefited from supracricoid partial laryngectomy with cricohyoidoepiglottopexy. Among TLM group, many surgical steps were systematically or occasionally performed for improving the glottic exposure.
First, patients were systematically placed in the position described by Boyce et Jackson. 12 The Dedo laryngoscope (Pilling, Philadelphia, PA) was employed in the majority of cases for the glottic exposure (n = 137; 97.1%). Bouchayer laryngoscope (MicroFrance, Paris, France) was used in 4 patients.
Second, laryngeal exposure was improved by an external counter pressure to the lower laryngeal framework in 93 (65.9%; Table 2) procedures. The use of external counter pressure was significantly associated with the T stage (P = .02). Thus, this procedure was necessary in 100%, 88%, 65.8%, and 44.1% of cT2, cT1b, cT1a, and cTis stage, respectively (Table 1).
Third, a partial vestibulectomy was performed in 81 (57.4%; Table 2) of 141 cordectomies. The number of partial vestibulectomies was significantly higher in T2 and T1b than in T1a and Tis tumor groups (P = .01; Table 1). Total vestibulectomy was performed in 6 (4.2%) patients with cT1b (n = 4) and T2 (n = 2) stages. Squamous cell carcinomas were extended to the anterior commissure or the arytenoid in 39 and 2 cases, respectively. Among the patients with tumor extension to the anterior commissure, 32 and 7 patients benefited from type Va and type VI cordectomy, respectively. The exposure was improved through external counter pressure in all cases (n = 39).
Fourth, resection of the suprahyoid epiglottis was necessary in 2 (5.12%) patients with anterior commissure tumor. The petiole of the epiglottis was resected for improving glottic exposure in 35 cases of the 39 anterior commissure tumors. Resection of the petiole of the epiglottis was significantly associated with the T stage (P = .001). This procedure was necessary in 100%, 94.1%, and 10.1% of cT2, cT1b, and cT1a cases, respectively (Table 1). There were no significant perioperative complication and no tracheotomy.
Margin Status and Survival Outcomes
According to the histopathological analysis, the margins were negative in 86 (60.9%) patients, suspicious in 19 (13.4%) patients, and positive in 36 (25.5%) cases. The “positive or suspicious margins” group included 55 (39.0%) patients. There was no significant difference between margin groups regarding the requirement of a type of procedures or an exposure difficulty (Table 2).
The 5-year DFS, DSS, and OS are reported in Table 3 according to the involvement of the vocal fold anterior commissure. The 5-year DFS rate of the entire cohort was 72.2%. Among the 34 patients with local recurrence, 19 (55.8%) benefited from second TLM and were free of recurrence 5 years after the initial treatment. Considering these patients, the final 5-year DFS rate was 88.2%.
Outcomes of Anterior Commissure Involvement.
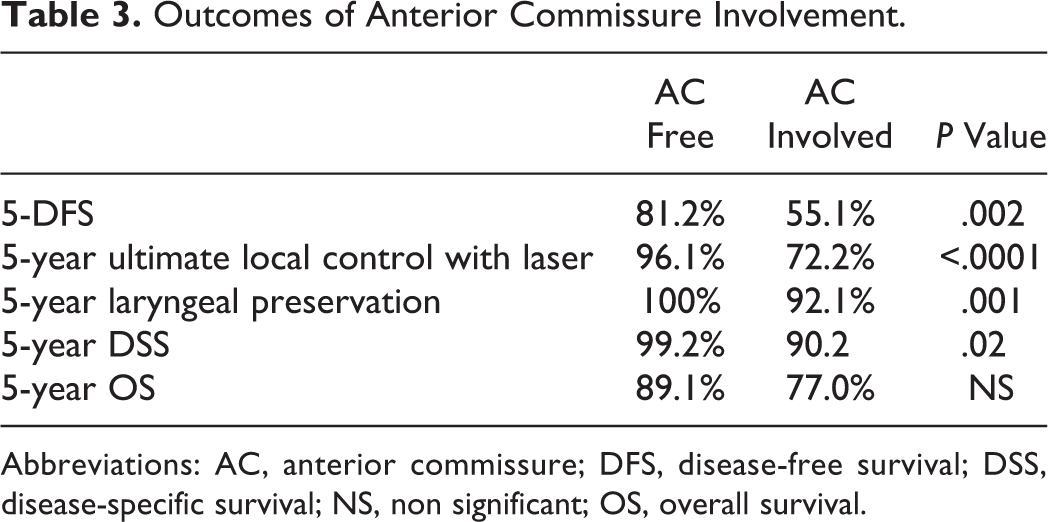
Abbreviations: AC, anterior commissure; DFS, disease-free survival; DSS, disease-specific survival; NS, non significant; OS, overall survival.
Among the 15 remaining patients with local recurrence, 9 and 2 required salvage radiotherapy and partial laryngectomy, respectively. Total laryngectomy was performed in 4 cases. The 5-year laryngeal preservation rates of patients with or without anterior commissure involvement were 92.1% and 100%, respectively (P = .001; Table 3). Regarding the linear regression analysis, there were no significant associations between OS, DFS, DSS, and the margin status of patients. Patients with a SCC involvement of the vocal fold anterior commissure had lower 5-year DSS and 5-year DFS rates compared to those without anterior commissure invasion (P < .02).
Discussion
Laryngeal exposure is a classical factor that may limit the realization of TLM cordectomy in 1.5% to 24% of cases regarding the current literature. 7 In the present study, only 4.7% of patients did not benefit from TLM cordectomy because inability to adequately expose glottic SCC. In other words, TLM cordectomy was realized in 95.3% of cases through many surgical additional procedures/tips. In the literature, a few authors have specifically analyzed the outcomes associated with glottic exposure. 6 -8 Among them, a very limited number really provided the tips and additional procedures allowing the improvement of the glottic exposure.
The patient position is the first step in getting adequate exposure. In our series, the patients were systematically placed in the position of Boyce et Jackson consisting of dorsal decubitus, anterior flexion of the neck, and head extension. 12 This position is long time know as one of the most adequate position for exposing the vocal folds and, especially, the anterior commissure. 12
The type of laryngoscope may substantially vary according to authors. In the current study, we used several types of laryngoscopes (Dedo and Bouchayer, Paris, France) with a curved end to have a better view on the laryngeal anterior commissure. The widest laryngoscope of Dedo was the most frequently employed (97.1%). In 2.1% of cases, we had to change the laryngoscope during the surgery for better exposure of anterior commissure.
The external counterpressure to the lower laryngeal framework is a traditional helpful procedure for improving laryngeal exposure. In this study, external counterpressure was necessary in 65.9% of cases for performing the cordectomy, especially in SCCs reaching the anterior commissure. The use of external counterpressure through adhesive tape or assistant surgeon maneuver for SCCs of the anterior commissure was reported in previous studies such as in the paper of Zeitels and Vaughan, who reported that the use of both external counterpressure and internal distention as an adjunct to microlaryngoscopy was most helpful for the surgical management of lesions located near the anterior commissure. 13 The disadvantage of this technique is the need to have an assistant surgeon for each TLM who has to remain motionless during the laser procedure.
The partial or total vestibulectomy may be performed for enhancing exposure of the glottis through a better visualization of the entire length of the vocal cord. This procedure was supported by Kashima et al 14 who specifically recommended the vestibulectomy as the first step of the procedure aiming to resect lesion of the full-length vocal fold. In our series, a partial vestibulectomy was performed in 57.4% of cases, while a total vestibulectomy concerned 4% of patients. The vestibulectomy is particularly interesting for large tumors (T1b and T2) compared to small tumors (T1a and Tis). In the same way, the requirement of external counterpressure procedure was significantly more frequent in large than small tumors (cT2 > cT1 > cT1a > cTis), which was, to our knowledge, not previously reported in the literature. Based on the data of the present study, the vestibulectomy would be required for SCCs that are not appropriately visualized after external counterpressure. Laryngologists should not hesitate to perform partial or total vestibulectomy regarding the potential risk of incomplete resection and related disease recurrence. The use of these additional surgical procedures makes particularly sense regarding the stronger DSS and DFS of SCCs reaching the anterior commissure, which corroborates the findings of other studies. 15,16 The stronger DSS and DFS of SCC reaching the anterior commissure may justify the realization of computed tomography scan before the surgery for assessing the invasion degree. In our practice, we often distinguish 2 types of SCCs of the anterior commissure: the vocal fold tumors that progressively reach the anterior commissure throughout the progression process and those that initially originate from the anterior commissure area. The latter would have a stronger prognosis than the first but, regarding the difficulties for precisely identifying the origin of the SCC, this hypothesis still remain undemonstrated.
The use of flexible fibers of some types of lasers (blue laser or diode) would be another way that can make the laser cordectomy possible in case of difficulties for exposing the lesion. 17 In this study, we did not investigate this option.
In this study, the OS and DFS were 86.4% and 97.8%, respectively, which is quite similar to the literature studies. 15,16,18 Interestingly, the margin status did not impact both OS and DFS. The impact of margin status on OS or DFS is still controversial in the literature regarding the pro- 16,18 and cons- 15,19 reports. Broadly, the heterogeneity between studies may be due to the different definitions of “suspicious” margin across studies, and factors related to both skills and experience of the pathologists who performed the margin analysis. The study of the role of pathologist makes particularly sense for the suspicious margins, which, depending of their proportions, may impact the results of the study. The systematic use of Narrow Band Imaging technology could improve the quality of resection of the vocal fold SCCs during the surgical time.
Conclusion
The knowledge of the different procedures that may improve the glottic exposure is an important step in the learning process of laryngeal surgeons. Some surgical tips may be particularly important for the exposure of tumors reaching the anterior commissure reducing the risk to require to partial laryngectomy. The position of patient, the use of an adequate laryngoscope, the counterpressure on the thyroid cartilage are the first procedures for improving the glottic exposure, whereas the second steps are the realization of vestibulectomy or epiglottis petiole resection. Because these tips usually lead to better exposure, the difficulties of glottic exposure do not impact the margin status of patients, which did not impact both OS and DFS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.