
Abstract

A 56-year-old woman presented with complaints of otalgia with left-sided hearing loss. She reported left tympanic membrane perforation and chronic ear infections secondary to traumatic injury as a child. She also had a history of intermittent otorrhea in the year prior to being seen at the clinic. Tympanometry of the left ear revealed restricted eardrum mobility and large equivalent ear canal volume. Audiometric testing showed a mild sensorineural hearing loss in the right ear and moderately severe mixed hearing loss in the left ear. The patient had a speech reception threshold of 45 dB hearing level (HL) and 88% word recognition at 80 dB HL with her left ear. An otoendoscope was used to examine the patient’s left external auditory canal and tympanic membrane, then advanced beyond the annulus and through the tympanic membrane perforation to the middle ear itself. A mass was seen superior to the eustachian tube opening and medial to the manubrium of the malleus (Figure 1). Subsequent computed tomography (CT) imaging revealed abnormal demineralization and lucency in the region of the facial nerve (FN) geniculate ganglion and along the rostral roof of the middle ear (Figure 2A and B). The location of the abnormality visualized by CT corresponded to the location of the mass observed during middle ear exploration. Magnetic resonance imaging (MRI) revealed an enhancing lesion present in the left FN geniculate ganglion region measuring 6 to 7 mm (Figure 2C and D). The pattern of demineralization present in the CT scan, together with the enhancing lesion observed by MRI, suggested FN hemangioma of the geniculate ganglion. Notably, the patient did not have any symptoms of FN weakness. No surgical intervention was taken; MRI follow-up 6 months later revealed no change in size of the hemangioma.
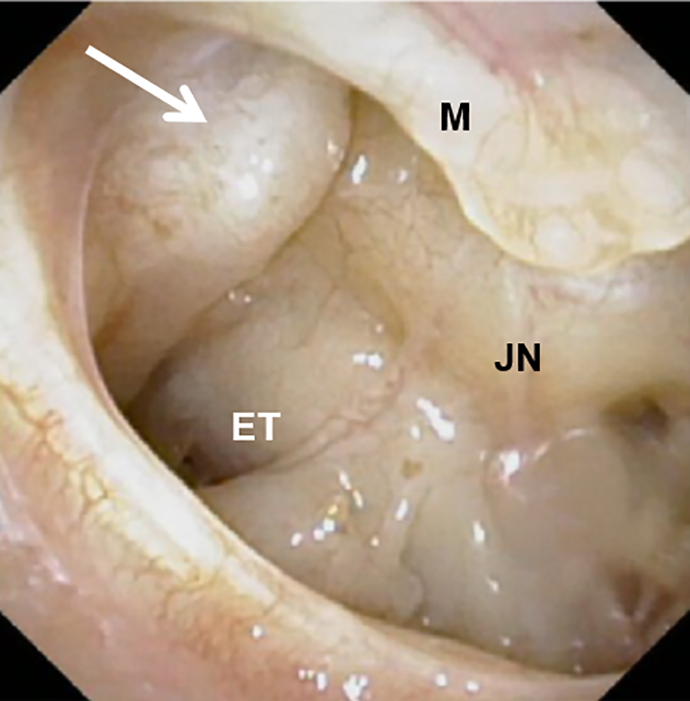
Otoscopy reveals mass in the middle ear (white arrow). ET indicates eustachian tube opening; JN, Jacobson’s nerve; M, manubriumof the malleus.
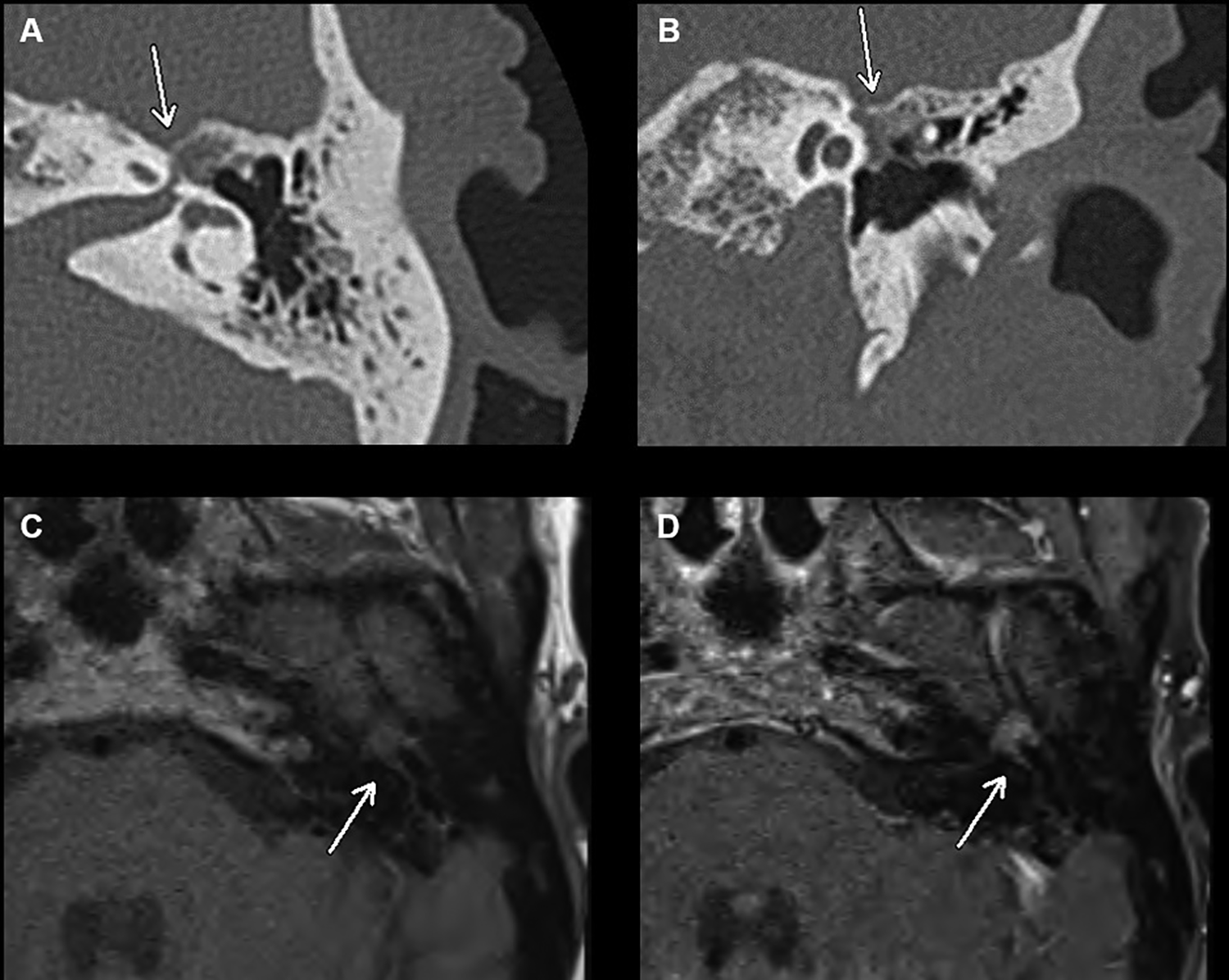
Geniculate ganglion hemangioma (white arrow) is seen by computed tomography (A, axial; B, coronal) and magnetic resonance imaging (C, no contrast; D, gadolinium enhanced).
Discussion
Geniculate ganglion hemangiomas (GGHs) are rare, benign vascular tumors of the FN involving the geniculate ganglion. 1 Facial nerve weakness is the most common presentation symptom of these tumors; a systematic review by Oldenburg et al found patients presented with FN palsy in 94% of GGH reported in the literature. Hearing loss and otalgia were less common presentation symptoms, found in 15% and 2% of reported cases, respectively. 2 There is disagreement regarding optimal management of GGH, due in part to the rarity of these lesions. Geniculate ganglion hemangiomas represent 0.7% of all temporal bone tumors, 3 with approximately 130 unique cases reported in the literature. 2,4 The limited research available suggests better outcomes when intervention is taken within the first year of onset of FN weakness along with subtotal resection of the lesion to preserve the FN. 2,5 Comment cannot be made on outcomes with surgical intervention prior to onset of FN palsy as the overwhelming majority of patients with GGH present with FN dysfunction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.