
Abstract
Chronic otitis media is a major contributor to acquired hearing loss in developing countries. Developing countries such as India, with huge populations and poor health infrastructures, have always felt the shortage of trained specialists who can provide quality care to meet the enormous demand for treatment of this disease. This pilot study assessed the feasibility of empowering trained health workers equipped with ENTraview, a store-and-forward telemedicine device that integrates a camera- enabled smart phone with an otoscope. This device allows the screening of otology patients within the community. Three months of extensive training was provided to five community health workers on primary ear and hearing care, including training on the use of the ENTraview device. Community otology screenings were conducted to triage otology patients and provide them with specialized ENT care at a tertiary hospital. In the initial 6 months of the project, 45 screening camps were organized, which screened 3,000 patients free of cost. Of these 3,000 screened patients, 54% (1,619) were referred for ENT consultation and 215 patients reported. Nearly 50% (103) of the 215 reporting patients required surgical intervention, and 29 patients underwent surgery. Reaching out to the community by remote screening of ear diseases by trained technicians with a telemedicine device seems to be an effective and cost-effective way to triage patients with otologic pathologies.
Introduction
Telemedicine is an umbrella term that involves all medical activity having an element of distance. 1 Telemedicine has been shown to be useful in the diagnosis and treatment of diseases involving the middle ear and tympanic membrane. 2 India is a country where the prevalence of ear diseases is among the highest, especially chronic suppurative otitis media (CSOM).
Ear disease is a neglected problem, both by the patients and by our existing healthcare system. It neither gets enough community health support nor does it generate serious patient attention because of widespread community myths and lack of awareness. According to a 2004 World Health Organization (WHO) report on otitis media, the prevalence of CSOM in South Asia is more than 4%. 4 In addition to this huge burden of CSOM and its associated morbidity, the region has an average of only three ENT specialists per million population, and 77% of CSOM cases in India are associated with hearing impairment. 3 Given the inadequate healthcare infrastructure of the country, reaching out to this underserved population by means of telemedicine seems to be a cost-effective way to address the problem of ear disease.
To meet this purpose, the ENT Department at Dr. Shroff’s Charity Eye Hospital (SCEH), New Delhi, in association with Medtronic, Inc., USA, implemented an outreach otology program in the urban slum area of New Delhi. SCEH is the first institution in India to partner with Medtronic and employ a telemedicine device in its outreach centers. This pilot study assessed the feasibility of empowering trained health workers equipped with a telemedicine device in screening otology patients from within the community.
Patients and Methods
This study was approved by the Institutional Review Board at SCEH. Written informed consent was obtained from all study participants. The study was conducted between July 2013 and December 2013.
The telemedicine device used in our project, ENTraview (Medtronic, Inc., USA; Minneapolis) is a camera-enabled android phone integrated with an otoscope (figure 1). There is a built-in, rechargeable, battery-operated light source for the otoscope. The device has been developed by Medtronic, Inc., USA, and its partners and makes use of an application developed by ClickMedix, USA (Gaithersburg, Md.). It utilizes touchscreen technology and uses the store-and-forward form of telemedicine. It allows the sender to generate a case with a unique identification number, and a drop-down menu for easy navigation is provided to record the case history. [Note: The ENTraview device is not for sale in the United States; in India, it is only available through Medtronic’s Shruti ear care program.]

Photo shows the ENTraview tele-
Five candidates were chosen who had basic secondary school degrees and an aptitude for social work. They were trained in our ENT department at SCEH for 3 months. The training consisted of intensive theory and practical classes. The training curriculum was based on the basic and intermediate modules of the Primary Ear and Hearing Care program developed by WHO. The curriculum included the following broad categories: anatomy and physiology of the ear, ear diseases, examination of the ear, symptomatic approach to ear diseases, and community ear care. Special emphasis was given to patient handling and eliciting clinical history.
In addition, the candidates attended ENT clinics to directly observe examination procedures and history taking. After this basic training, hands-on otoscopic examination and ENTraview device usage were taught under the supervision and clinical expertise of the authors. At the end of 3 months, the health workers equipped with ENTraview devices were posted in peripheral centers of the hospital in three urban slum areas of Delhi state.
Health camps were regularly organized in the service areas to screen patients with ear diseases and hearing loss. A project coordinator with prior experience in handling community health projects was also engaged in the project. The coordinator organized local community camps to mobilize patients from the community. Between July 2013 and December 2013, a total of 45 camps were conducted, in which a total of 3,000 patients with subjective ear complaints voluntarily reported.
The smart phone’s digital camera captured the image of the tympanic membrane and ear canal and stored it in the memory of the smart phone. This image, along with the case summary (figure 2) was later uploaded on the ClickMedix website (figure 3). This was an asynchronous communication that allowed the sender to take the necessary time to collect data from the patient and then send the case to the consulting physician, who later responded at his/her convenience.

Patient data can be seen being saved in

ClickMedix website is medicine device. the ENTraview device. shown, with patient data and ENTraview-uploaded tympanic membrane pictures.
Patients with obvious or suspicious pathology were called for an in-clinic examination by a specialist in the ENT department at SCEH. The health workers communicated with the identified patients personally or telephonically and counseled them for an in-clinic ENT examination and relevant investigations.
All data were analyzed using the Statistical Package for the Social Sciences, v. 20.0 (IBM; Armonk, N.Y.). All analyses were two-tailed, and a difference was considered statistically significant if the p value was ≤0.05.
Results
Of the total 3,000 screened patients, 1,413 were females and 1,587 were males. In the 16- to 40-year age group, females (701) outnumbered males (425). The 0- to 15year age group and the >40-year age group showed no gender predominance.
Of the 3,000 patients screened, health workers identified 1,619 (54%) patients requiring examination by an ENT specialist or an audiologist, who were then referred to the base hospital. The remaining 1,381 (46%) people were found to be normal and did not require any further examination.
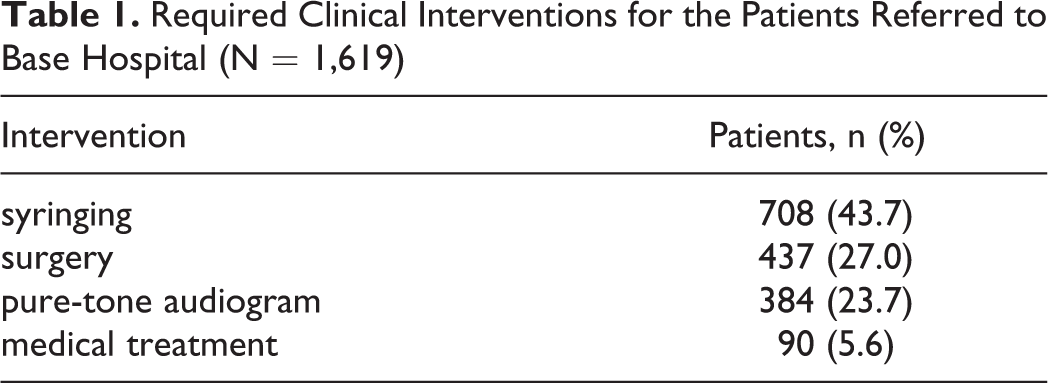
Table 1 shows the distribution of the required clinical interventions for the 1,619 patients as deemed appropriate by the health workers. Of 437 patients identified for surgical intervention, 425 were suspected to have CSOM and 12 were suspected to have secretory otitis media (SOM).
Required Clinical Interventions for the Patients Referred to Base Hospital (N = 1,619)
As of December 2013, a total of 215 patients (table 2) had reported to us, and 103 (101 CSOM cases and 2 SOM cases) of those were identified as candidates for surgical intervention. Of the 101 CSOM cases, 92 had tubotympanic disease and 9 had atticoantral disease.By December 2013, we had performed 29 subsidized surgeries (at 40% of the usual cost), including tympanoplasties (n = 26), mastoid explorations (n = 2), and myringotomy and ventilation tube insertion (n = 1). The usual cost of these surgeries at our institution is INR 10,000 (approximately $160 US). Other patients awaiting surgery were under regular follow-up and medical treatment. Thirty-one pure-tone audiograms were done, and 4 patients required hearing aids. Hearing aids were dispensed to those 4 patients at subsidized rates.
Treatment Plans/Clinical Interventions for Patients Reporting to the Base Hospital (n = 215)
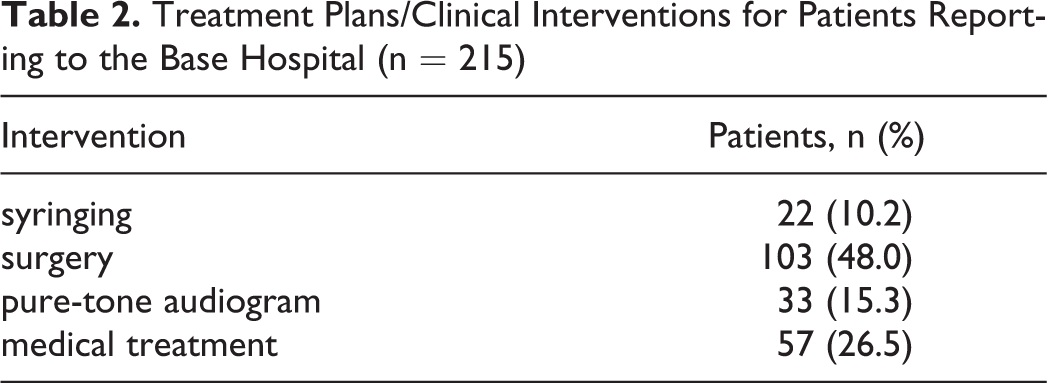
Twenty-two (3.1%) patients who reported to the base hospital underwent syringing for clearing of wax and debris from the ear canal. Fifty-seven other patients (63.3%) with ear diseases such as otitis externa, acute otitis media, otomycosis, and foreign body in the ear canal were managed with conservative treatment. Of those patients reporting to the hospital, 103 (23.6%) underwent surgery, and for 33 (8.6%) patients, pure-tone audiograms were obtained. Patients referred for medical treatment and surgery were significantly (chi-square p value <0.001) more likely to report to our hospital than patients who were referred for pure-tone audiometry and surgery.
Between July 2012 and December 2012, a total of 744 patients visited our hospital from the same three urban slum areas under investigation. Between January 2013 and June 2013, 676 patients visited and, finally, during our study period, July 2013 to December 2013, 1,050 patients visited, of whom 215 came through the 45 camps we organized.
Discussion
WHO estimates that CSOM is a major contributor to acquired hearing loss in developing countries, with the worldwide global burden of illness involving 65 to 330 million individuals. 3 Of these individuals, 60% have significant hearing impairment, indicating that CSOM may contribute more than half the global burden of hearing impairment, and that eliminating it can potentially reduce the global burden by four-fifths. 4 The aim of our study was to demonstrate the efficacy of telemedicine by remote screening of ear diseases by trained technicians using a telemedicine device.
Unlike the Kokesh et al experience, in which storeand-forward telemedicine was used for ENT care, employing the services of trained audiologists for ENT examination in remote areas of Alaska, 5 we trained community workers on the use of the ENTraview device for patient screening. As in the Alaska study, our patients got a chance to discuss their ear disease without having to travel far and could see the status of their tympanic membranes. This is a key advantage of the ENTraview device, considering that once the patients could see their ear pathology on the ENTraview screen, it motivated them to take some remedial action.
Further, at a convenient time, the specialist doctors gave their opinions by looking at the digitized data of patients and notifying the community workers to encourage the identified patients to seek further evaluation, investigation, and appropriate medical management in our tertiary hospital.
Despite providing screening services in their local area and motivating identified patients for an examination at the base hospital, the reporting rate there during the first 6 months of our study was only 13%. This is the key limitation of our study. Even patients identified for surgical intervention with significant hearing loss need a strong motivation to travel to the base hospital within the city for subsidized surgeries. To offset these issues, resources are needed to develop education and communication material and to train dedicated counselors to encourage patients to take remedial measures.
The potential for telemedicine to reduce inequalities in healthcare is immense but remains underdeveloped. This gap can only be bridged by institutions that want to bring about change in the community through innovations. Smith et al have done a similar screening program in aboriginal children of Australia and have found encouraging results. 6
One of the challenges in sustaining a telemedicine program is not only having a core champion to promote the concept, but having the right people to support that concept and make the everyday running of the program efficient and effective. 7 The health workers and the project coordinator must have good interpersonal and communication skills in the local language of the community to be screened.
Further, to ensure success and sustainability of any initiative, a robust business model is critical. There is no single business model that will work for every program because every program offers different services, operates in different environments, and relies on different amounts of external funding. 7 We believe that our model of screening patients with hearing disorders has the potential to change the way the community and national hearing programs are run in the developing world.
Conclusion
Reaching out to the community by remote screening of ear diseases by trained technicians using a telemedicine device seems to be an efficacious and cost-effective way to triage patients with otologic pathologies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by Medtronic, Inc., USA (Minneapolis), which provided the ENTraview device. ClickMedix, USA, (Gaithersburg, Md.) provided us with the software application for the project. No monetary or non-monetary compensation was provided to any of the authors.