
Abstract
Objective:
Allergic rhinitis is a type 1 hypersensitivity reaction of immunoglobulin E in the rhino-ocular mucosa. This study was planned to demonstrate in patients with allergic rhinitis to evaluate changes in tear, nasal secretions, and blood osmolarity compared to healthy individuals.
Method:
Forty allergic rhinitis patients, 25 patients with acute upper respiratory tract infections, and 26 healthy participants were included in the study. Positive patients with allergic symptoms and skin prick test results were included in the allergic rhinitis group. Tear, nasal secretion, and blood osmolarity values were examined for the 3 groups.
Result:
In patients with allergic rhinitis, tear and nasal secretion osmolarity values were significantly higher in patients with acute upper respiratory tract infections and those of the healthy participants (P = .001, P = .038). In blood osmolarity measurements, there was no statistical difference between the groups (P = .489). In patients with allergic rhinitis, Schirmer test results were significantly shorter than patients who had acute upper respiratory tract infection and those of the healthy participants (P = .001, P = .001). Patients with allergic rhinitis and acute upper respiratory tract infections had significantly shorter Schirmer test results than in healthy participants (P = .001, P = .001).
Conclusion:
Tear osmolarity was increased in allergic rhinitis patients, and this was thought to lead to dry eye findings. In the presence of allergic rhinitis, nasal secretions were found more hyperosmolar than tears. Nasal secretion osmolarity was higher in allergic rhinitis patients than in patients with acute upper respiratory tract infections and control group.
Introduction
Allergic rhinitis is a type 1 hypersensitivity reaction resulting from the development of immunoglobulin E in the rhino-ocular mucosa due to allergens, and the diagnosis is made by history and physical examination. 1 Allergic rhinitis is characterized by nasal obstruction, discharge, pruritus, sneezing, and postnasal drip, due to inflammation of the nasal mucosa. 1 Many patients with allergic rhinitis have ocular symptoms. 2 It has been shown that allergic rhinitis and dry eye association are significantly higher in adults. 3 Dogru et al reported that the presence of tear film instability was higher in children with allergic conjunctivitis, allergic rhinitis, and asthma. This study showed that allergic rhinitis and dry eye association are significantly higher in children. 4
Test such as the Schirmer test, which is a tear break time measurement, is simple and useful in ophthalmologic clinics and often used. 5 Measurement of tear osmolarity is as important and is an easy method to measure when less tears are present in dry eyes, and it is the simplest measurement method for dry eye diagnosis and classification. 5 -7 Tear hyperosmolarity is caused by inflammatory factors that constitute dry eye disease and is positively correlated with the severity of the disease. 6 Tear osmolarity is in the range of 303 to 305 mOsm/L in normal eyes, whereas values above 316 mOsm/L are considered to be hyperosmolarity. 7 The aim of this study is to investigate tear, nasal secretions, and blood osmolarity of patients with allergic rhinitis and compared with normal participants.
Materials and Methods
This is a prospective study with approval dated March 1, 2017, and the decision number 5/11 was received from the Ethical Board for Clinical Research at the Faculty of Medicine, BezmialemVakif University. Written informed consents of all patients were obtained.
The study included a total of 91 consecutive patients (40 patients with allergic rhinitis, 25 patients with acute upper respiratory tract infection, and 26 control participants), who applied to the Otorhinolaryngology and Ophthalmology outpatient clinics during April to July 2017.
Criteria for excluding participants from this study were as follows: use of steroids in the last 1 month and antihistamines in the last 15 days, participants who had upper respiratory tract infection, acute airway disease such as nonallergic eosinophilic rhinitis or drug-induced rhinitis, asthma, and the presence of unilateral or isolated polyp(s). Patients who were included in the study did not have any disease that could lead to dry nose and dry eye syndrome.
Cases were divided into 3 different groups: allergic rhinitis group, acute upper respiratory tract infection group, and healthy participants (control group).
Allergic rhinitis group: 40 allergic rhinitis patients (15 male, 25 female, age range 18-43 years, average age 29.7 ± 8.6) who have allergic rhinitis symptoms and were identified as having an allergy against at least 1 active agent from the skin prick test were included. Patients with allergic rhinitis have ongoing symptoms. Symptoms and incidence rates of allergic rhinitis patients were recorded.
Acute upper respiratory tract infection group: 25 patients with acute upper respiratory tract infection (12 male, 13 female, age range 19-45 years, average age 32.2 ± 7.2) were included. Patients with acute upper respiratory tract infection who had complaints of flu or cold, who had symptoms for 2 to 3 days, and who did not use any drugs were included in the study. Symptoms and incidence rates of acute upper respiratory tract infection patients were recorded (Table 1).
Symptoms of the Allergic Rhinitis Group (Group 1), the Acute Upper Respiratory Tract Infection Group (Group 2), and Control Group (Group 3).
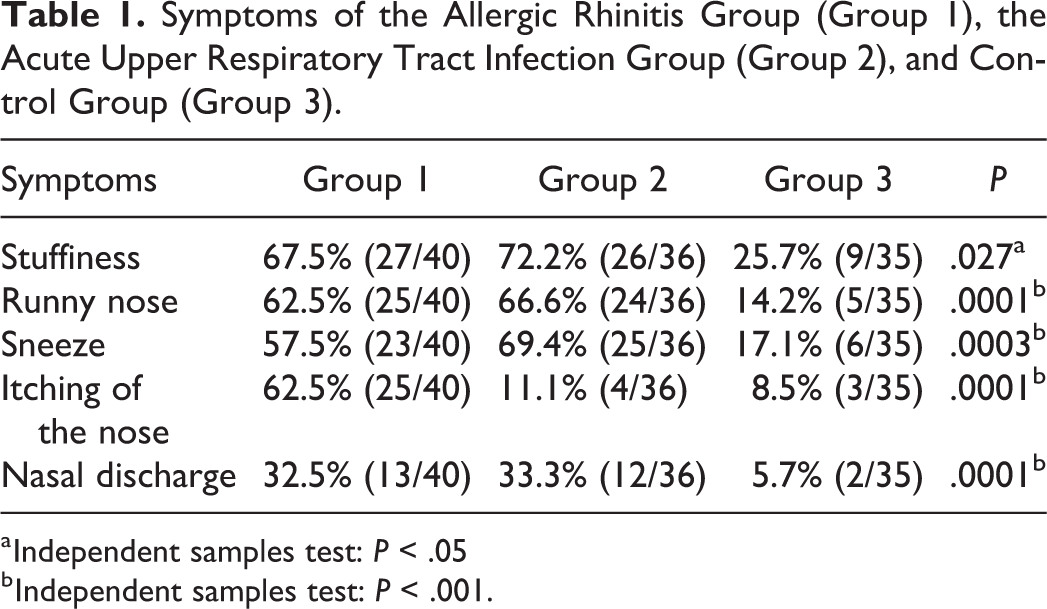
a Independent samples test: P < .05
b Independent samples test: P < .001.
The control group consisted of 26 healthy people of similar age and gender (13 male, 13 female, aged between 19 and 44 years, average age 33.7 ± 9.1) who have normal ocular examination except refractive disorders, without any history of allergic disorders, systemic diseases, or drug consumption and with negative skin prick test results. Since active nasal secretion was not present in healthy participants, only tears and blood osmolarity were evaluated in our study.
Schirmer I test (with topical anesthesia): here, 35-mm long and 5-mm wide absorbant strips were used. The Schirmer I test result was expressed as the wet length of the strip measured after 5 minutes. The results below 6 mm were accepted as dry eye. 8
Tear break-up time (TBUT) test: Two minutes after the application of fluorescein dye, the TBUT is measured at the slit lamp using the cobalt blue filter over the light source. The patient was asked to blink once and then keep her/his eyes open. Tear break-up time is defined as the time in seconds between the patient’s last blink and the first appearance of a random dry spot on the corneal surface. The test is repeated 3 times and the mean value is recorded. 9 A TBUT test score below 10 seconds was accepted as abnormal. 10
Skin Prick Test
Standard allergen extracts of the brand Alyostal ST-IR (Staller Genes S.A., Pans, France) were used for skin prick tests. Allergen extracts were drawn into Quick test applicators with 8 heads and were applied to the skin at the ventral side of the forearm, after the testing site was cleansed with alcohol. We used histamine (1 mg/mL) as a positive control and isotonic NaCl as a negative control. The results were read 15 minutes after the application. Test validity criteria were set as >3 mm for positive controls and <3 mm for negative controls. A skin reaction with an induration of 3 mm or more was accepted as positive. 11 Fourteen common allergens (Dermatophagoides pteronyssinus, Dermatophagoides farina, cockroach, trees mix, grasses mix, pine, cat feather, nuts, Penicillium mix, Cladosporium, cacao, egg, wheat, and Alterina) plus a negative and a positive control were applied to the skin of the forearm with two 8-headed applicators.
Tear and Nasal Secretion Osmolarity Measurement
When tear, nasal secretions, and blood osmolarity measurements were taken, attention was paid not to complete any procedure that would result in a different day, after a good sleep and rest period, and before reflex tear stimulation on the day after the first examinations and tests were performed. Measurements were performed with a TearLab Osmolarity tester. We used a TearLab Osmolarity device (TearLab Corporation, San Diego, California). The TearLab Osmolarity tester is a device that indirectly measures values from 275 to 400 mOsm/L. Before the measurement, the device was tested with its own calibration cartridge. After calibration, disposable commercial cartridges were used for each patient and measurement. In both groups, the tear samples were taken a few seconds after the device was moved from the right eye to the left. Osmolarity measurements were made from the nasal secretions in patients with allergic rhinitis and upper respiratory tract infection. Tear samples were taken in accordance with the guidelines of the TearLab Osmolarity device so that reliable measurements were obtained, and the resulting values were recorded in mOsm/L. The normal tear osmolarity is between 280 and 295 mOsm/L and is equivalent to normal blood osmolarity. The tear osmolarity lower limit for light dry eyes was 305 mOsm/L, and the lower limit for tear osmolarity for severe dry eye eyes was 316 mOsm/L. 7,11 All measurements were performed by the same researcher.
Statistical Analysis
The NCSS (Number Cruncher Statistical System) 2007& PASS (Power Analysis and Sample Size) 2008 Statistical Software (Utah) programs were employed for evaluating the data gathered in the study. Besides using descriptive statistics (median, standard deviation) in evaluating the data, the 1-way analysis of variance (ANOVA) test was used for comparing the quantitative data and for comparing the normally distributed parameters between groups. The significance level was set at P < .001 and P < .05.
Result
The study included 91 patients (51 females [56.0%], 40 males [43.9%] aged between 18 and 45 years, average age 32.8 ± 9.1) who were examined in our clinic. The patients were assigned into 3 groups: group 1 included 40 allergic rhinitis patients; group 2 included 25 acute upper respiratory infection patients, and group 3 included 26 healthy people.
The symptoms and frequencies of the groups were recorded and compared with each other. Group 1 and 2 patients had significantly more frequent symptoms than the control group with 1-way ANOVA test (P < .05; Table 1). The results of 1-way ANOVA test compared with the mean ages and sex of the 3 groups did not reveal any statistically significant difference (P = .641 and P = .269, respectively; Table 2).
Demographic Data of the Groups.
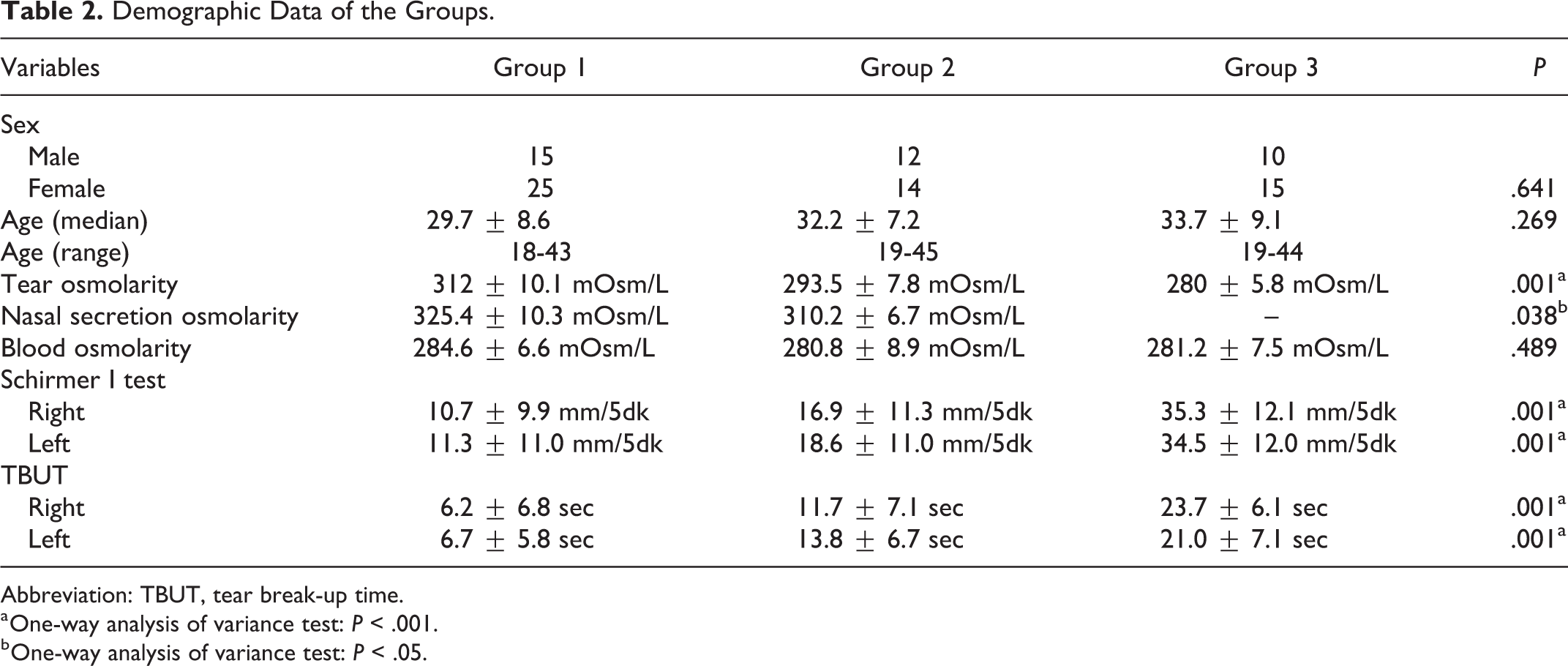
Abbreviation: TBUT, tear break-up time.
a One-way analysis of variance test: P < .001.
b One-way analysis of variance test: P < .05.
In tear osmolarity measurements, there was a statistically significant difference between the groups. In patients with allergic rhinitis, tear osmolarity values were significantly higher in patients with acute upper respiratory tract infections and healthy participants (P = .001). In nasal secretion osmolarity measurements, a statistically significant difference was observed between group 1 and group 2. In patients with allergic rhinitis, nasal secretion osmolarity values were significantly higher in patients with acute upper respiratory tract infections (P = .038). In blood osmolarity measurements, there was no statistically significant difference between the groups (P = .489; Table 2 and Figure 1).
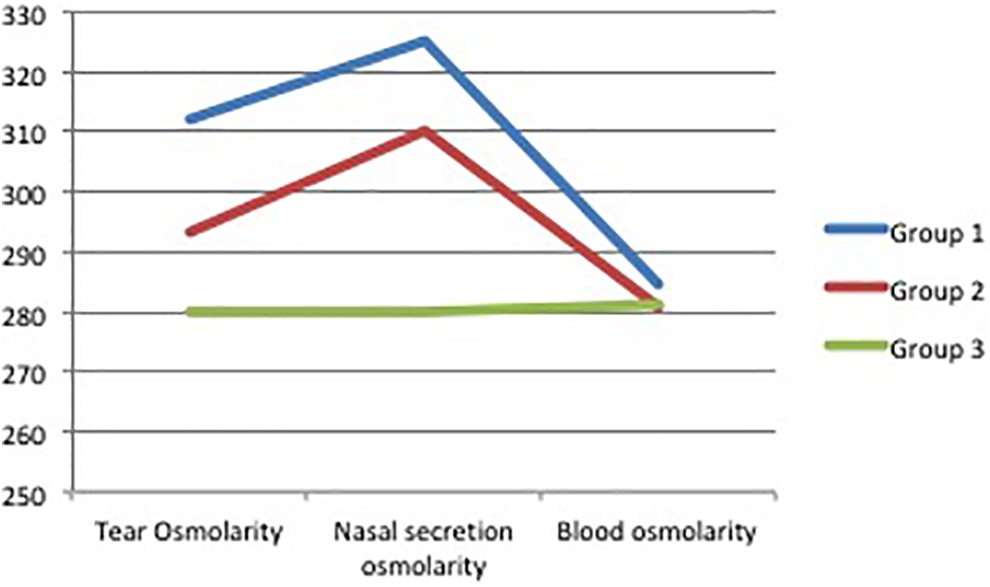
Osmolarity values of groups.
From Schirmer test results, a statistically significant difference was observed between the groups for the right and left eyes. In patients with allergic rhinitis, the Schirmer test results were significantly shorter compared to patients with acute upper respiratory tract infection and those of the healthy participants (P = .001, P = .001; Table 2 and Figure 1).
In tear break time results, there was a statistically significant difference between the groups. In patients with allergic rhinitis, patients with acute upper respiratory tract infection and those of the healthy participants were significantly shorter in terms of tear breakage time (P = .001, P = .001; Table 2 and Figure 1).
Discussion
In our study, tear osmolarity was observed in patients with allergic rhinitis diagnosed by clinical symptoms and skin test. For this reason, shortness of Schirmer test and tear breakage time showed dry eye symptoms. This result is thought to be caused by the inflammatory effects of an allergy. It was observed that nasal secretion osmolarity was higher in allergic rhinitis patients compared to those with acute upper respiratory tract infections. Allergic rhinitis and dry eye association are known. The hyperosmolar nature of nasal secretions in the presence of allergic rhinitis suggests the association of dry nose with allergic rhinitis, which was described for the first time in the literature. There were no changes in the results of allergic rhinitis, acute upper respiratory tract infections, and blood osmolarity in healthy individuals. This suggests that allergic rhinitis and acute upper respiratory tract infections have only a local inflammatory effect. 11 -13
The nasal ocular reflex creates the interaction between the nose and the eye. In order to support this reflex, it has been shown that the use of a nasal spray is beneficial for ocular symptoms of allergy after the eyes have been irrigated and after unilateral irritation of the nasal mucosa and also that dry eye symptoms in allergic rhinitis patients are significantly improved by nasal steroid therapy. 11 -13
Lemp et al reported that tear osmolarity showed 73% sensitivity and 92% specificity for dry eye syndrome. 12 Tear hyperosmolarity is caused by inflammatory factors that constitute the dry eye and is positively correlated with the severity of the disease. 6 The severity of rheumatoid arthritis, a chronic infection, has been reported to be related to dry eye and tear hyperosmolarity. 13 Miserocchi et al reported the presence of tear hyperosmolarity (mean value 322.90 ± 33.39 mOsm/L) in the presence of pemphigus, an autoimmune disease. 14 Bunya et al reported in 49 cases with Sjögren syndrome, the TearLab Osmolarity System tear osmolarity was 314.5 mOsm/L. In this study, tear osmolarity showed a significant and negative correlation with both Schirmer I test and Ocular Surface Disease Index. 15 In our study, mean tear osmolarity was 312 ± 10.1 mOsm/L and nasal secretion osmolarity was 325.4 ± 10.3 mOsm/L in patients with allergic rhinitis. Nasal secretion in allergic rhinitis patients was more hyperosmolar than tears (Table 2).
Aragona et al showed that hypotonic sodium hyaluronate eye drops in dry eye patients with Sjögren syndrome may be more useful than isotonic eye drops for the treatment of disease. 16 Acute allergic rhinoconjunctivitis has been proven to cause hyperosmolar tears due to the underlying inflammatory process, and hypotonic artificial tear application has been shown to prevent ocular surface damage by improving tear osmolarity. 11 In 1 study, hypertonic saline was shown to be more effective in children with seasonal allergic rhinitis than normal saline. 17 In our study, we also observed hyperosmolarity in the tear and nasal secretions with allergic rhinitis. In the presence of allergic rhinitis, nasal secretions were found more hyperosmolar than tears. When the results of this study are evaluated, dry nose can be defined in the presence of allergic rhinitis, as is the case with allergic rhinitis and dry eye. Investigations may be planned to determine the effect of using hypotonic nasal wash solutions for nasal symptoms of allergic rhinitis.
In our study, nasal secretion osmolarity was 325.4 ± 10.3 mOsm/L in allergic rhinitis patients and nasal secretion osmolarity in patients with acute upper respiratory tract infection was 310.2 ± 6.7 mOsm/L. Nasal secretion osmolarity was higher in allergic rhinitis patients than in patients with acute upper respiratory tract infections. In a clinical practice approach, examining the nasal secretion osmolarity values of patients with nasal discharge may help to diagnose acute upper respiratory tract infection in allergic rhinitis. Our study was the first in the literature to examine osmolarity of tear, nasal secretion, and blood in patients with allergic rhinitis.
Conclusion
Hyperosmolar effects on tear and nasal secretions are thought to be due to the underlying local inflammatory causes of allergic rhinitis. In the presence of allergic rhinitis, nasal secretions were found more hyperosmolar than tears. Therefore, dry nose can be defined in the presence of allergic rhinitis. The hyperosmolarity that is formed in nasal secretions is defined as the coexistence of allergic rhinitis and dry nose for the first time and comprehensive studies should be supported.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.