
Abstract

Clinical Cases
Recently, as we experienced 2 cases of polyps arising from the nasal septum completely resected by endoscopic surgery, we present 2 cases focusing on endoscopic differences.
Case 1
A 52-year-old healthy woman presented with progressive left-sided nasal obstruction of 3 months’ duration. Nasal endoscopic examination revealed a unilateral mass with a thin and long pedicle attached to the superior aspect of the posterior portion of the nasal septum in the left nasal cavity. The main mass was lobular in shape mimicking papillomatous lesion and hanging through the choana with its bulky portion in the nasopharynx (Figure 1A and B). Computed tomography demonstrated a 1.6 cm × 0.9 cm × 1.1 cm lobulated and pedunculated mass, originating from the left nasal septum, which protruded into the nasopharynx (Figure 1C and D). Under local anesthesia, the mass was completely excised using endoscopic instrumentation. The base of the mass, including the healthy mucosa of the left posterior septum, was removed and cauterized using suction cautery for prevention of recurrence. Histopathological examination revealed chronic inflammatory polyp. There were no signs of recurrence during a follow-up period of 6 months.
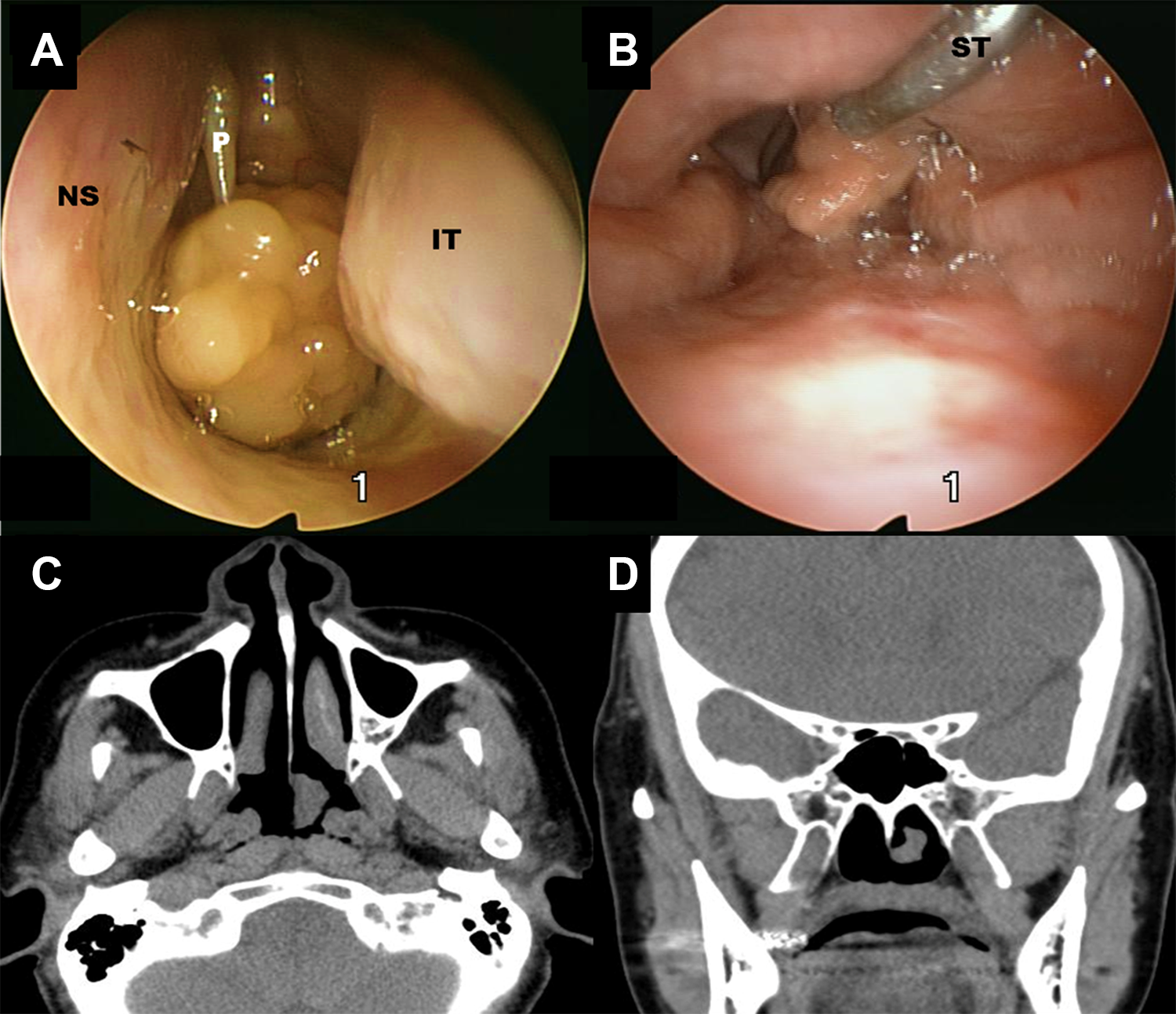
Endoscopic view and PNS CT findings. A, Nasal endoscopy showed a unilateral choanal mass with a thin and long pedicle attached to the superior aspect of the posterior portion of left nasal septum. B, Transoral retrovelar nasopharyngoscopy showed the bulky portion of the mass. C and D, showed the left choanal mass originating from the septum protruding into the nasopharynx. CT indicates computed tomography; IT, inferior turbinate; NS, nasal septum; P, pedicle; PNS, paranasal sinus; ST, suction tip.
Case 2
A 39-year-old healthy man presented with progressive left-sided nasal obstruction of 1 months’ duration. Nasal endoscopic examination revealed a unilateral mass attached broadly and tightly to the superior aspect of the posterior portion of the nasal septum in the left nasal cavity. The mass was sessile and lobular in shape mimicking papillomatous lesion and partially extended to the nasopharynx (Figure 2A and B). Computed tomography demonstrated a 1.5 cm × 1.0 cm × 1.0 cm lobulated mass, originating from the left nasal septum, which protruded into the nasopharynx (Figure 2D). Under local anesthesia, the mass was completely excised using endoscopic instrumentation. The base of the mass, including the healthy mucosa of the left posterior septum, was removed and cauterized using suction cautery for prevention of recurrence (Figure 2C). Histopathological examination revealed chronic inflammatory polyp. There were no signs of recurrence during a follow-up period of 12 months.
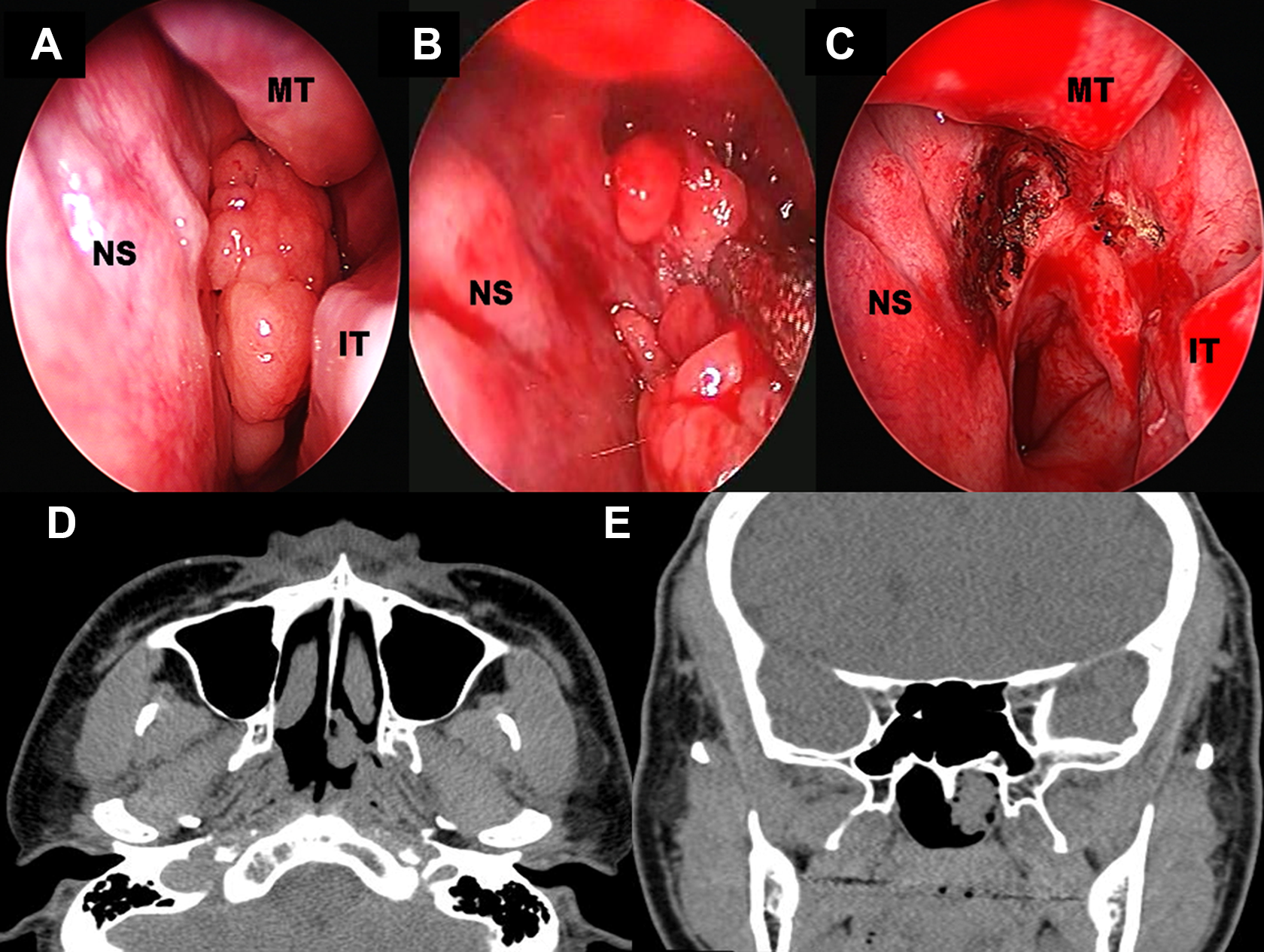
Endoscopic view and PNS CT findings. A and B, Nasal endoscopy showed a unilateral mass attached broadly and tightly to the superior aspect of the posterior portion of left nasal septum. The mass was sessile and lobular in shape mimicking papillomatous lesion and partially extended to the nasopharynx. C, After the mass was completely excised including the healthy mucosa of the left posterior septum, the base of the lesion was cauterized using suction cautery for prevention of recurrence. D and E, Computed tomography demonstrated a lobulated mass, broadly based on the left nasal septum, which protruded into the nasopharynx. CT indicates computed tomography; IT, inferior turbinate; MT, middle turbinae; NS, nasal septum.
Discussion
Choanal polyps are one form of the nasal polyps that grow and extend into the choana with a single stalk. 1 Although choanal polyps can arise from various locations of nasal cavity which are named as antrochoanal, sphenochoanal, and ethmochoanal polyp depending on the sites of origin, 2 septochoanal polyp originating from the mucosa of the nasal septum with choanal extension is a very rare disease entity, accounting for 1.5% according to Stammberger’s study which found only 3 patients with polyps originating from the posterior nasal septum. 2,3 The most common site of origin of septochoanal polyp is mainly the superior aspect of the posterior nasal septum. 2,4 -6
The commonly presenting symptoms of septochoanal polyps include nasal obstruction and snoring. 2,4 -6 Accurate preoperative detection of the site of origin by nasal endoscopic examination may be important for differential diagnosis and surgical planning. 2,5 Endoscopic findings of previously reported case reports can be divided into 2 groups, pedunculated type and sessile type. In pedunculated type, 2,4,5 the polyp had a thin pedicle attached to the posterior nasal septal mucosa and its bulky portion extended into the nasopharynx. In sessile type, 6 the gross finding of one case was not described in detail except that it was a sessile form. Based on the gross finding of our case 2, the polyp was the papilloma-like mass which broadly attached to the superior aspect of posterior nasal septum without a pedicle and partially extended to the nasopharynx. Computed tomography is not essential for the diagnosis, but it may allow for accurate identification of paranasal sinus involvement and the site of origin. 5 For differential diagnosis of mass in nasopharynx including choanal polyps, benign tumors such as juvenile angiofibroma, teratoma, meningoencephalocele, chordoma, paraganglioma, inverted papilloma, adenoid hypertrophy, and angiofibroma need to be ruled out. 5,7 On the basis of our experiences, the treatment for septochoanal polyp with or without a pedicle is complete removal using endoscopic surgery. Also, it is an important point that the resection of a small amount of healthy mucosa surrounding the site of origin is necessary in order to prevent recurrence. 2,4,5
Footnotes
Authors’ Note
Ethics approval not required. The patient’s permission was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.