
Abstract
Sudden sensorineural hearing loss is a common otologic disease in clinic. Systemic and intratympanic steroid treatment have been proved to be effective, but the regimens vary from center to center. The purpose of the study is to analyze the effects of the combined application of intravenous dexamethasone and intratympanic methylprednisolone injection in different time strategies for the treatment of unilateral sudden sensorineural hearing loss. A retrospective chart review was performed for the period from March 2016 to June 2018 at our Department of Otorhinolaryngology—Head and Neck Surgery. A total number of 61 patients who met the academy criteria for unilateral sudden hearing loss were included and grouped based on the time to introduce intratympanic methylprednisolone. All the patients received intravenous dexamethasone 10 mg once daily for 5 days, followed 5 mg once daily for the next 7 days. Intratympanic methylprednisolone (40 mg) was injected every other day 4 times into all patients. This regimen was commenced on day 1 in group 1 and on day 6 in group 2. The pre and posttreatment pure-tone audiograms were analyzed. Sixty-one patients met our inclusion criteria. No significant differences were observed between patients’ demographics or pretreatment hearing thresholds. In the 3 months posttreatment pure-tone audiogram assessment, the mean hearing threshold improvement were similar between groups with no frequency specificity. The curative rate in both groups were similar and satisfying. Two patients with diabetes mellitus had persistent small perforations. Some patients had other transient discomfort that disappeared before discharge. The different timing of initiation of intratympanic methylprednisolone injection does not significantly affect the outcome of the treatment for sudden sensorineural hearing loss. Thus, we suggest that intratympanic steroid injection should not be applied as a first-line method except for patients who do not respond early to systemic steroid therapy.
Keywords
Introduction
Sudden sensorineural hearing loss (SSNHL) is a common otologic disease in clinic. It is defined as an acute decrease in the hearing thresholds by at least 30 dB in 3 adjacent frequencies that has occurred within 3 days. 1 It is the condition usually appears unilaterally and is accompanied by vertigo, tinnitus, and aural fullness. The annual incidence rate of SSNHL in China is uncertain but was estimated to be 5 to 27/100 000 in the United States and 5 to 20/100 000 globally. 2,3 Although vasospasm, hair cell lesions, and viral infections are considered to be the cause of the disease, the etiologies and pathogenesis of SSNHL are still debatable. Due to the tendency for spontaneous recovery, the treatment for SSNHL is mainly symptomatic and varies from center to center but generally includes the administration of steroids, vasodilators, anticoagulants, antiviral medications, plasma expanders, and hyperbaric oxygen therapy. 4 Previous studies established systemic steroids as the first-line therapy with recovery rates of up to 70%. 5,6 However, the prognosis of systemic steroid treatment is not satisfactory for some SSNHL patients, especially those with severe hearing loss, vertigo, or late treatment. Moreover, the latent side effects of corticosteroid therapy and its contraindications have considerably limited its application, urging researchers to investigate and discover novel methods for local administration of steroids. Intratympanic steroid treatment was used in 1996 for hearing impairment and tinnitus in patients with various inner ear conditions such as Meniere disease. 7 It is an invasive way of delivering a drug directly to the affected cochlea through the round window membrane to enhance the local concentration and duration of medication action, avoiding its systemic absorption. Several uncertainties exist in this technique. For example, the existence of anatomical abnormalities of a round window niche or faulty procedures might lead to a void response. 8 Additionally, even if the implementation of different routes may decrease the outflow, the loss of the medication through the eustachian tube is still inevitable and unpredictable. However, the efficacy of intratympanic steroid treatment has been confirmed, and this approach has been used mostly as salvage therapy after systemic steroid treatment has failed. Several theories attempt to explain the mechanism of action of steroids in the inner ear. Some of them include downregulation of inflammation, promotion of cochlear blood flow, inhibition of inner ear apoptosis, improvement of the stria vascularis function, and maintenance of ion homeostasis. 9,10 Combined with the effect of systemic steroids, which decrease leucocyte count and inhibit the activities of inflammatory mediators, it is reasonable to deduce that the joint action of locally and systemically administered steroids would improve the therapeutic results. Many studies have been focused on the therapeutic results of the combined treatments. 4,11 However, the optimal timing of initiating intratympanic methylprednisolone injection in the combined therapy remains unclear. In the present study, we analyzed the outcomes of combined steroid therapy in simultaneous and secondary groups to compare the efficiency of different therapeutic regimens in the treatment of SSNHL patients.
Patients and Methods
Patients
A retrospective chart review was performed in our Hospital from March 2016 to June 2018. The following inclusion criteria were used: (1) adults older than 18 years with complete medical records; (2) patients diagnosed with unilateral SSNHL, defined as an acute decrease in the hearing thresholds >30 dB in at least 3 consecutive frequencies within 72 hours, established by pure-tone audiogram; (3) no acoustic neuroma was found by magnetic resonance imaging; (4) patients with type A tympanogram with no signs of middle ear fluid during endoscopy examination; (5) patients admitted to our ward for treatment within 1 week after the onset, who had not receive any other treatment before that; (6) patients had their pure-tone audiogram results before the treatment, and 3 and 6 months after the treatment had passed.
The exclusion criteria applied were as follows: (1) patient had medical histories of chronic otitis media, otosclerosis, Ménière disease, large vestibular aqueduct syndrome, or any other diseases that could cause sensorineural hearing loss; (2) patients who recently had otologic surgeries; (3) recurrent SSNHL; (4) patients with cerebrovascular conditions; (5) patient with a medical history of autoimmune diseases; (6) the pure-tone audiogram showed low-frequency SSNHL (patients with low-frequency SSNHL were excluded because of high rates of spontaneous recovery and much better outcomes).
The included 61 patients were divided into 2 groups based on their initiation of intratympanic methylprednisolone injection: in group 1, the patients received both therapy simultaneously; in group 2, patients were given intravenous dexamethasone for 5 days before the methylprednisolone injection started. This study was approved by the Committee of our Hospital. All patients signed informed consent forms before we collected their data for research.
Study Design
The systemic treatment was dexamethasone 10 mg ivgtt (give the medicine intravenously, iv drip) once daily for 5 days and tapering to 5 mg ivgtt once daily for another 7 days. The intratympanic methylprednisolone was administered to patients 40 mg/1 mL every other day for a total of 4 doses. Group 1 patients received combined therapy synchronously. Group 2 patients were those who didn’t respond early to systemic treatment alone and their intratympanic steroid treatment started at day 6.
The procedure of methylprednisolone intratympanic injection is described below. In our endoscope room, the patients lay down in the supine position with the affected ear upward. All patients received topical anesthesia of lidocaine (2%) for 10 minutes. Before the procedure, the lidocaine was drained and the ear canal was cleaned. An experienced otologist then punctured the tympanic membrane in the anterior inferior or posterior inferior quadrants with a 27-gauge spinal needle and slowly injected 40 mg/mL methylprednisolone using an otoendoscope. The patients were required to maintain the body position without swallowing for at least 30 minutes after the procedure. Contact of the affected ear with water had to be avoided during the course until the integrity of the ear drum had been confirmed. The blood pressure and blood sugar levels of the patients with relevant medical history were strictly monitored and treated (when needed).
Pure-Tone Audiometry
Pure-tone audiometry was conducted by 2 experienced and certified audiologists. Hearing thresholds from 250 Hz to 8000 Hz were recorded before the treatment and then 3 months after the therapy to assess the treatment efficacy. The pure-tone audiometry 6 months after the therapy was used as a long-term follow-up indicator.
Statistical Analysis
Patients’ demographic data, including sex, age, side, time from onset to treatment, concomitant symptoms (vertigo, tinnitus, and aural fullness), and accompanying underlying diseases were recorded.
Descriptive variables such as age and days from onset are expressed as means ± standard deviations or median (range). Categorical variables, such as sex, side, and medical history, are expressed as n (%). Paired t test was used to compare the intragroup age differences. The Mann-Whitney U test was implemented to compare the intragroup onset days. Other categorical variables were analyzed by the Fisher exact test or the χ2 test.
The values from the air conduction measurements of all frequencies (250, 500, 1000, 2000, 4000, and 8000 Hz) performed at the onset and 3 months after the treatment, and at the 6 month follow-up examination were determined.
The pure-tone averages (PTAs) and the mean hearing gains of each given frequency, speech frequencies (500, 1000, 2000, and 4000 Hz), and all frequencies are expressed as mean ± standard deviation and were compared using Sidak multiple comparison test after the thresholds were corrected by 2-way analysis of variance to eliminate the influence of the interference factors.
To evaluate the efficiency, the patients were also categorized based on their mean hearing gains in verbal frequencies: significant effect (≥30 dB), effect (≥15-30 dB), and no effect (<15 dB); the rate of each category was calculated and compared between groups.
All statistical analyses were 2-tailed and considered statistically significant at a P value <.05. All statistical assessments were completed using SPSS software (version 22.0; SPSS Inc, Chicago, Illinois).
Results
Patients
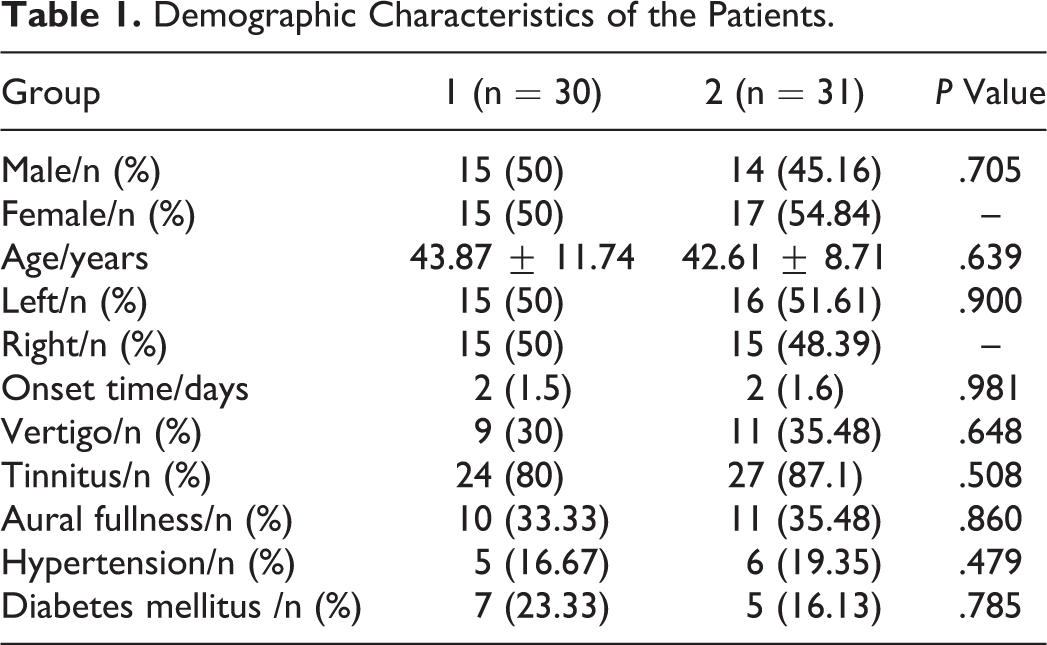
A number of 61 patients met the criteria and were grouped (group 1, n = 30; group 2, n = 31). The demographics of the 2 groups were similar (Table 1).
Demographic Characteristics of the Patients.
The PTAs of each frequency, verbal frequencies, and all frequencies before the treatment between the groups were similar (Table 2). The hearing of the unaffected ears in each frequency was within the normal range.
Average Air Conduction Measurements by Pure-Tone Audiometry at the Onset.

Evaluation of Efficacy
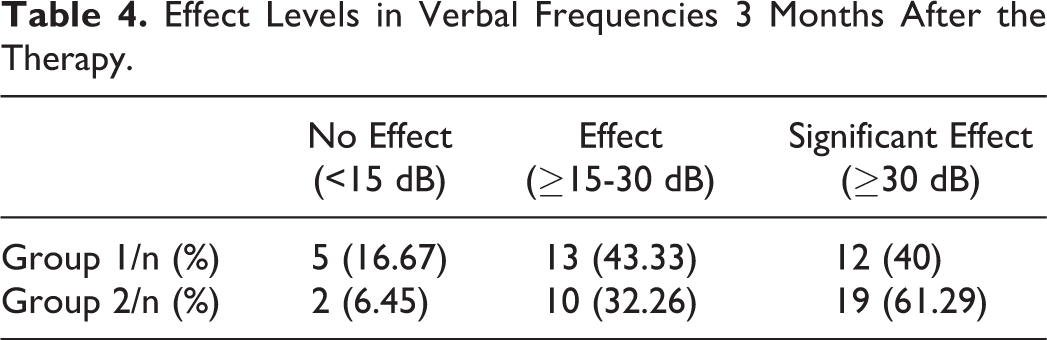
The PTAs of the treatment groups were similar 3 months after the therapy (Table 3). The mean gains in PTAs were comparable between both groups (Figure 1), with significant improvement versus those before the treatment (P < .001). Group 2 had a greater percentage of patients who have significant effect and lower percentage of patients who receive no effect from the therapy, however, there was no statistical significance between groups (P = .217; Table 4).
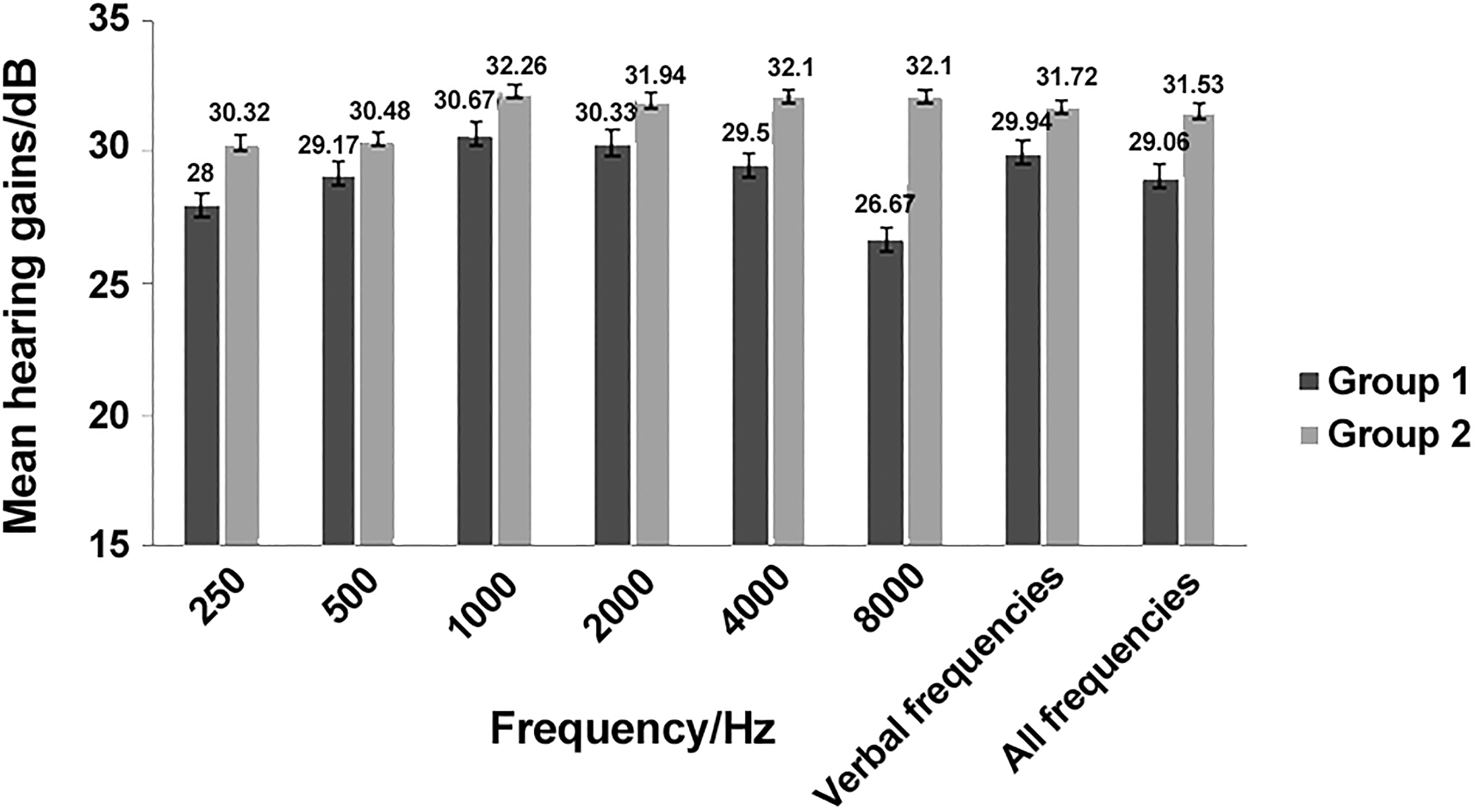
Mean hearing gains 3 months after the therapy.
Average Air Conduction Measurements by Pure-Tone Audiometry 3 Months After the Therapy.

Effect Levels in Verbal Frequencies 3 Months After the Therapy.
The curative rate was defined as the rate of patients with hearing gains ≥15 dB. We calculated the rate at the given hearing frequencies, the verbal frequencies, and all frequencies (Table 5). The curative rates in group 2 were higher at most frequencies but no significant differences were found between 2 groups.
Curative Rates 3 Months After the Therapy.

The data of long-term hearing thresholds were collected from the 6 months follow-up (group 1: 40.5 ± 21.76 dB, group 2: 38.79 ± 20.04 dB), and it seemed no different from that of 3 months posttreatment in both groups (group 1: 39.27 ± 22.28 dB, group 2: 37.61 ± 20.57 dB), which suggests that patients obtained maximum benefits through the short-term therapy.
Side Effects
The blood pressure and blood sugar levels of all patients with hypertension or diabetes were under control during the whole study. After starting the intratympanic injections, a total number of 4 (6.6%) patients complained of transient dizziness which was resolved spontaneously after rest; 10 (16.4%) patients showed ear fullness with no significant signs of otitis media which recovered as the therapy continued; and 13 (21.3%) patients experienced obvious but tolerable temporary otalgia after the procedure. Three (4.9%) patients had small perforations at discharge, and 1 was recovered at the 6-month follow-up examination; 2 patients with diabetes mellitus had persistent perforations. We recommended that the patients who refused to receive tympanoplasty should avoid contact with water in the affected ear and attend the clinic for regular check-ups.
Discussion
In this study, we evaluated different methylprednisolone intratympanic injection timing strategies in combination with intravenous dexamethasone in the treatment of SSNHL. Both groups achieved satisfactory hearing improvement during the 3-month follow-ups, and their hearing gains were comparable at frequencies ranging from 250 to 8000 Hz. Group 2 had a tendency of a greater percentage of patients who have hearing gains ≥30 dB and lower percentage of patients who receive no effect from the therapy. However, no statistically significant difference was detected (P = .217). The curative rates were satisfactory (based on the mean gains in the verbal frequencies: 83.3% vs 93.5%, P = .255), with no significant intergroup differences. Our results indicate that the timing of introducing intratympanic steroids may not influence the outcomes of the treatment of SSNHL. The long-term (6 month) hearing outcomes were not different from those established in PTAs at the 3-month follow-up, which suggests that the patients had gain maximum benefits through the short-term therapy.
Despite the unelucidated physiological mechanism, systemic steroid treatment has been established as mainstream for SSNHL for decades. Intratympanic steroid, on the other hand, has firmly remained an effective and safe salvage therapy, as reported previously. 9,12 -14 Most of recent investigations searched for other roles intratympanic steroid injection can play in the treatment in SSNHL for its pharmaceutical effect and high-precision delivery to the cochlear fluids. 15 Several studies explored its feasibility as initial therapy and achieved promising results. For instance, Kosyakov et al found that the intratympanic group had a more pronounced PTA improvement in the verbal frequencies than the systemic group. 16 Filipo et al obtained similar results after a fairly short course of treatment in a pool of 217 patients. 17 In a meta-analysis conducted by Lai et al, although the intratympanic and systemic therapies appeared to present similar efficiency, the authors still recommended a local approach as initial therapy due to the lower possibility of steroid use-associated side effects. 18 Further research probed into the efficacy of combined treatment, but the results were contradicting. In a prospective randomized controlled trial (RCT), 60 patients were randomly and equally divided into 3 groups based on the therapy applied: oral steroid, intratympanic dexamethasone injection, and both. It is noteworthy that no significant differences in the hearing gains and recovery rates among the 3 groups were established. 19 Another RCT held in Turkey also compared the efficacy of intratympanic methylprednisolone with and without oral methylprednisolone. While the hearing improvement was equivalent among patients with a mild to moderate hearing loss (PTA < 70 dB) intragroup, the combination therapy group had statistically significant greater hearing improvement compared to that of the oral steroid alone in patients with severe hearing loss. 20 Battaglia et al conducted a multicenter, double-blinded, placebo-controlled, randomized study in 2008 and found that the patients who received combined therapy had greater improvements in their speech discrimination score (SDS), and a higher portion of them achieved a significant improvement in PTAs than those who received only oral prednisone. 21 In another prospective, multicenter trial conducted by the same authors in 2014, a similar conclusion was reached. 22 Jung da et al conducted a retrospective case–control study with 105 patients and discovered that at the time point of over 90 days, the hearing thresholds of patients administered with combined steroid therapy were significantly lower than those of patients treated only with systemic steroid (43 ± 31.2 dB vs 54.8 ± 31.4 dB). A significantly greater SDS improvement was also found in the combined therapy group in this study (72.3% ± 36.2% vs 57.4% ± 42.3%). 23 The most recent meta-analysis of Han et al evaluated the superiority of combination therapy with 14 RCTs, and announced that the combination therapy exhibits statistically significant increase in hearing improvement, PTA changes, and SDS changes. 24 Above all, there is a trend of considering combined therapy as a better solution for SSNHL among otologists. However, in the lack of strong evidence, the regimen varies from facility to facility. By reviewing relevant literature, we found that specific and distinct drug combinations, injection schedules, and therapeutic approaches were used in almost each research. In our examination, we chose intravenous dexamethasone in an effort to achieve a higher drug concentration, using intratympanic methylprednisolone for its better diffusion coefficient, longer elimination half-time, and its ability to regulate sodium transport and reabsorption in the inner ear. 25
Accumulating evidence has indicated that the early intervention is an important prognostic factor in the therapy of SSNHL. Statistically significantly different response rates (76.1% vs 50%) were established between the early treatment group and the delayed treatment group in a retrospective study with 176 SSNHL patients who received intratympanic steroid injection. 26 Cvorovic et al conducted a similar study and significant recovery in hearing was achieved in 60% of the patients who received treatment within 7 days since onset. However, this rate dropped to 40% in those who received treatment later than 7 days after the onset. These authors created a mathematical model for calculating the probability for hearing recovery, and the correlation between the intervals from the onset to treatment, and the hearing gains was weak but significant. 27 Nonetheless, it is unclear whether this need for timeliness can also be applied to the initial time of intratympanic injection in combined therapy. Thus, whether synchronized intratympanic steroid injection provides better results in hearing recovery than the subsequent modality still needs to be elucidated.
In a retrospective study conducted by Chu et al divided 53 eligible patients into a concurrent group (intratympanic injection was started together with the intravenous steroid treatment) and a sequential group (intratympanic injection was started at day 4 or 5 after the intravenous steroid treatment). In this study, intravenous dexamethasone was administered 5 mg twice a day. for 5 days with an oral tapered dose for 6 days, and intratympanic dexamethasone was injected 5 mg once daily for 5 consecutive days. The hearing gains in both groups were comparable, except at frequencies of 4000 and 8000 Hz, where the hearing improvement in the concurrent group was significantly higher than that in the sequential group. Hence, Chu et al deduced that the selective beneficial effect on high frequencies was caused by the achieved base-apex drug concentration gradient. 28 Our study didn’t observe different effects in certain frequencies, however, since it is expected that most significant changes after intratympanic injections to be in high-frequency thresholds, the results may differ in 12 000 Hz or 16 000 Hz.
The complications related to intratympanic steroid therapy included perforation, otorrhea, otitis media, vertigo, dizziness, ear fullness, and otalgia. In our study, one-fifth of the patients had transient minor discomfort, and only 2 (3.3%) patients with diabetes mellitus had persistent perforations. Other studies reported similar small probabilities of adverse events. Thus, intratympanic therapy can be considered low-risk and tolerable. However, medical personnel should explain to patients these potential drawbacks and obtain their informed consent before implementation.
Limitations
Given the retrospective nature of this single institutional study, the major limitations are the small size of patients and the possible bias. To eliminate the interference of the delayed treatment, our inclusion criteria limited the time from onset to therapy for 1 week, which might have caused selection bias. The patients assigned to group 2 were those who did not response early to the systemic steroid administration, which might have weakened the results. In addition, we did not set subgroups of different types of hearing loss, which might have contributed to the occurrence of false positive results, because the prognosis varied in the different types of SSNHL. The PTA is a reflection of the impairment of inner ear function, and the parameters used for its identification include the hearing thresholds, the curve type, and the specific form. The most commonly used evaluation system simply averages the hearing thresholds, which leads to the loss of individual specificity. Therefore, to reach better interpretation of research results, it is best to obtain and evaluate detailed individual patient data.
In conclusion, SSNHL is common in the outpatient clinic and emergency room of an ENT doctor, thus, an urgent need exists for the identification of a safe and effective therapeutic strategy in daily medicine practices. Our study evaluated the success rate of different timing of initiating intratympanic methylprednisolone injection in combined therapy. We established satisfactory hearing threshold improvement in both groups and no more considerable hearing improvement was observed in the early intratympanic steroid injection group than in the late treatment one. Hence, we consider the potential side effects and recommend that intratympanic steroid injection should not serve as a first-line method. However, patients with late responses to systemic steroid treatment might benefit from intratympanic methylprednisone used adjunct to intravenous dexamethasone. Nevertheless, multicenter RCTs are needed to further elucidate that mechanism and confirm our present findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Health and Family Planning Commission of Shenzhen Municipality [Grant Number SZXJ2017065].