
Abstract
Chronic granulomatous invasive fungal sinusitis (CGIFS) is a peculiar disease of the paranasal sinuses due to its rarity, patient subset, and disease course. We describe 7 cases of histopathologically confirmed CGIFS with different treatment plans and varying outcomes. Of particular note was that one of these patients developed allergic fungal rhinosinusitis after complete resolution of his primary invasive disease, a finding that has never been reported in the literature. Another patient had an atypical fungal species (Aspergillus nidulans) on fungal stain and culture, while one immunodeficient patient had a large intracerebral disease component and died after 2 months of treatment. We also present a review of the pertinent literature investigating this rare disease.
Introduction
Fungal sinusitis is categorized as invasive or noninvasive based on the histopathological evidence of fungal invasion of the underlying tissues. The noninvasive form is further divided into allergic fungal rhinosinusitis (AFRS), fungal ball, and saprophytic fungal infections. Invasive fungal sinusitis is a rare disease that primarily affects patients in an immunocompromised state. It is classified as acute fulminant, chronic, or chronic granulomatous disease. The chronic granulomatous subtype has been observed to occur in immunocompetent hosts. 1 -3 The overwhelming majority of chronic granulomatous invasive fungal sinusitis (CGIFS) cases are found in areas with dry climates, such as India, Sudan, and Saudi Arabia. Aspergillus species are usually isolated from these cases. 4,5 Delay in diagnosis is a typical finding across the literature; moreover, the ideal management approach is controversial and is subject to several influencing factors such as the nature of the disease, the degree of tissue invasion, and patient comorbidities. 6 In view of the paucity of reports on CGIFS, we present 7 cases of patients diagnosed with the disease and we review the pertinent literature. A summary of the cases is shown in Table 1.
A Summary of the 7 Cases of CGIFS.
Abbreviations: AFRS, allergic fungal rhinosinusitis; CGIFS, chronic granulomatous invasive fungal sinusitis; HTN, hypertension; NA, Not applicable; TB, tuberculosis.
Case Series
Case 1
A healthy, 42-year-old female presented at the neurology clinic with severe headache lasting 3 months and associated with behavioral changes. Ophthalmological and neurological examinations were normal. Computed tomography (CT) of the brain revealed a large left frontal lobe lesion. The initial impression was a malignant neoplasm, so the patient underwent craniotomy and excision of the mass with wide margins. The histopathological finding of chronic granulomatous inflammation with no evidence of malignancy was confirmed. Fungal stain and culture confirmed the presence of invasive fungal hyphae (Aspergillus flavus) within the granulomas. The patient was started on oral voriconazole and caspofungin. She was also referred to the rhinology service due to CT evidence of mucosal thickening and bone erosion of the lateral sphenoid sinus wall. The nasal endoscopy failed to show any abnormality. Endoscopic sinus surgery (ESS) was performed, during which pale, nonbleeding posterior ethmoid and sphenoid mucosa were found. A biopsy was taken from the mucosa and endoscopic debridement of all the diseased tissues was performed, revealing the lateral sphenoid wall defect with an intact dura mater layer. Histopathological diagnosis of CGIFS was established (Figure 1). The patient subsequently underwent daily bedside endoscopic debridement with application and replacement of caspofungin-soaked packing in the posterior ethmoid and sphenoid sinuses.
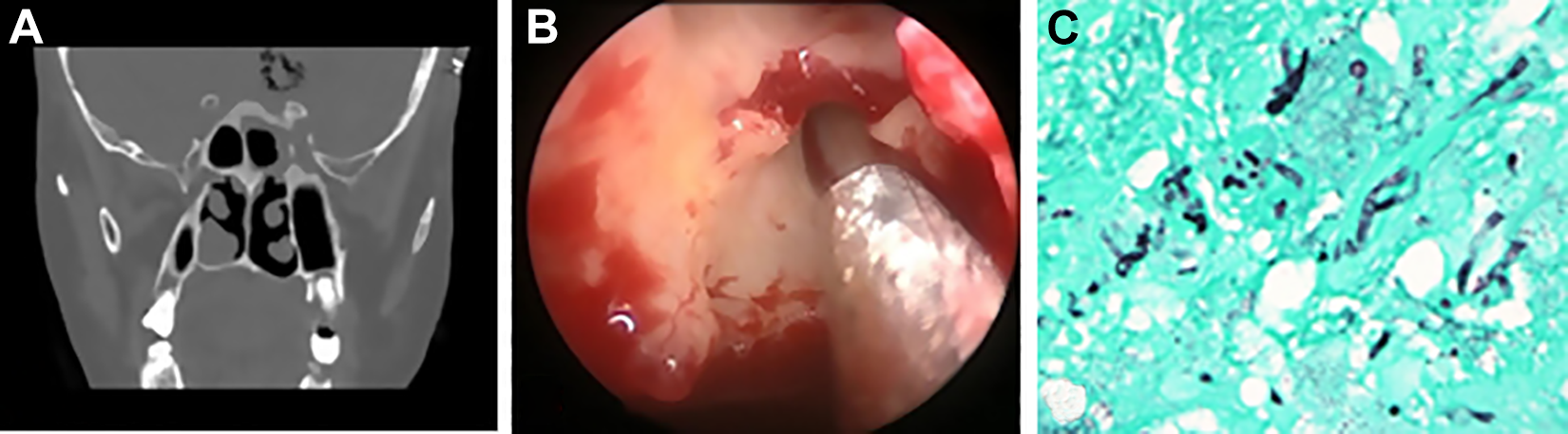
A, Thin-cut paranasal sinus computed tomography (CT) in the coronal plane at the level of the sphenoid sinus showing a left lateral sphenoid wall bony defect with surrounding mucosal thickening. Postcraniotomy brain changes can also be seen. B, Intraoperative endoscopic view of the left posterior ethmoid sinus showing pale sinus mucosa. C, Microscopic view on the histological slide confirming the diagnosis of chronic granulomatous invasive fungal sinusitis (CGIFS). Grocott’s methenamine silver (GMS) stain of the left frontal lobe tissue reveals invasive branching septate fungal hyphae.
Two weeks postoperatively, the patient developed multiple brain abscesses. Evacuation of the abscesses was performed. A second-look endoscopic debridement was performed in the operating room, and no sinonasal progression of the disease was found. The hematological and immunological workup revealed iron deficiency anemia as well as low total immunoglobulin G and immunoglobulin M levels. Immunoglobulin transfusions were carried out, and multiple myeloma was suspected. Further workup was not completed as the patient’s condition deteriorated rapidly. She succumbed to the disease in the eighth week due to bacterial salmonella–related ventriculitis.
Case 2
A 69-year-old female, known to have hypertension, hypothyroidism, and chronic anemia, presented to the rhinology clinic complaining of left nasal obstruction for the preceding 7 months associated with frontal headache, retro-orbital pain, and decreased facial sensation. Nasal endoscopy showed dry crusts filling the left middle meatus. No abnormality was seen on ophthalmological and neurological examination. Both CT and magnetic resonance imaging (MRI) of the paranasal sinuses (PNSs) showed a left posterior ethmoid and sphenoid lesion extending into the orbital apex and the pterygopalatine fossa. The patient underwent ESS with intraoperative findings of granulation tissue filling the left posterior ethmoid and sphenoid sinuses and invading the orbital apex. Endoscopic debulking of the lesion was done without violation of the periorbita. Histopathological findings confirmed the diagnosis of CGIFS, and A flavus was cultured. A 9-month course of oral voriconazole was completed. At the 3-year follow-up visit, she was asymptomatic, and nasal endoscopy showed normal sinonasal mucosa.
Case 3
A 37-year-old female presented complaining of right-sided nasal obstruction, infraorbital swelling, and diplopia for the preceding 4 months. She presented with a nasal biopsy histopathological report from an outside institute, which showed invasive fungal disease. She also reported having undergone ESS 5 years prior to her presentation, but no reports of this were available. On examination, right infraorbital swelling pushing the globe upward was found, with normal extraocular movement and visual acuity. Nasal endoscopy showed a reddish mass occupying the right maxillary sinus, with no abnormality detected on neurological examination. Both CT and MRI of the sinuses showed a right maxillary lesion extending into the cheek and pushing the orbit superiorly without periorbital invasion. Histopathological diagnosis of CGIFS and fungal culture of A flavus were confirmed. The patient was started on oral voriconazole. Endoscopic medial maxillectomy with complete removal of all the diseased tissues was performed without periorbital violation. The patient was seen in the clinic at the 1-year follow-up reporting no symptoms and showing normal, healed mucosa on nasal endoscopy.
Case 4
A 27-year-old male with a known diagnosis of Pott disease presented at the rhinology clinic, with an incidental CT and MRI finding of a left ethmoid mass extending to the extraconal orbital fat. The patient did not report any symptoms, and no abnormality was detected on endoscopic nasal examination. The ophthalmological and neurological examinations were normal. Endoscopic sinus surgery was performed, during which a pale mass occupying the ethmoid sinus and attached to the skull base and lamina papyracea was identified. The mass was grossly debrided from the skull base and orbital wall without violation of the periorbita or dura. Histopathological diagnosis of CGIFS was established. The fungal culture was positive for Aspergillus nidulans. The plan was to start oral voriconazole, but the patient refused and went home against medical advice. Six months later, he presented to the clinic with no symptoms. Endoscopic nasal examination showed no abnormality. Magnetic resonance imaging showed the same previously noted orbital disease component. The patient was strongly encouraged to start voriconazole. However, he missed his subsequent appointments, so no further follow-up information was obtained.
Case 5
A healthy 29-year-old Sudanese male presented complaining of having progressive left proptosis for 1 year with no visual disturbances. He reported having undergone ESS 6 years previously, though no reports were available. Other than proptosis, the patient’s ophthalmological and neurological examinations were normal. Nasal endoscopy showed a pale mass occupying the left ethmoidal cavity. Both CT and MRI showed a left ethmoid cavity mass eroding the lamina papyracea, extending into the extraconal fat and blocking the frontal recess. In addition, significant mucosal thickening of the maxillary sinuses with multiple bony defects was detected bilaterally on imaging (Figure 2A). The patient underwent ESS with debulking of the pale and firm tissue from the periorbita on the left (Figure 3A). Bilateral maxillary antrostomies and left frontal recess dissection were also carried out for debulking and to obtain a biopsy. Histopathological diagnosis of CGIFS and fungal culture of A flavus were confirmed (Figure 4A). The patient was started on a 6-month course of oral voriconazole. In addition, off-label topical application of 1% voriconazole was given as nasal drops: 3 drops in the lying head back position, twice daily for 6 months. At 7 months postoperatively, endoscopy showed a clear sinonasal cavity with no residual disease. At 9 months postoperatively, the patient presented with nasal obstruction, and endoscopy revealed a thick mucin-like discharge with ethmoidal polyps bilaterally. The MRI showed classic features of AFRS (Figure 2B-D). He then underwent complete bilateral ESS (Figure 3B). Multiple biopsies taken from several areas revealed evidence of mucin containing noninvasive fungal hyphae, which was cultured as A flavus. There was no evidence of invasive fungal disease in any of the specimens (Figure 4B). The patient was subsequently continued on nasal rinsing with saline mixed with budesonide respules, with no recurrence to date.
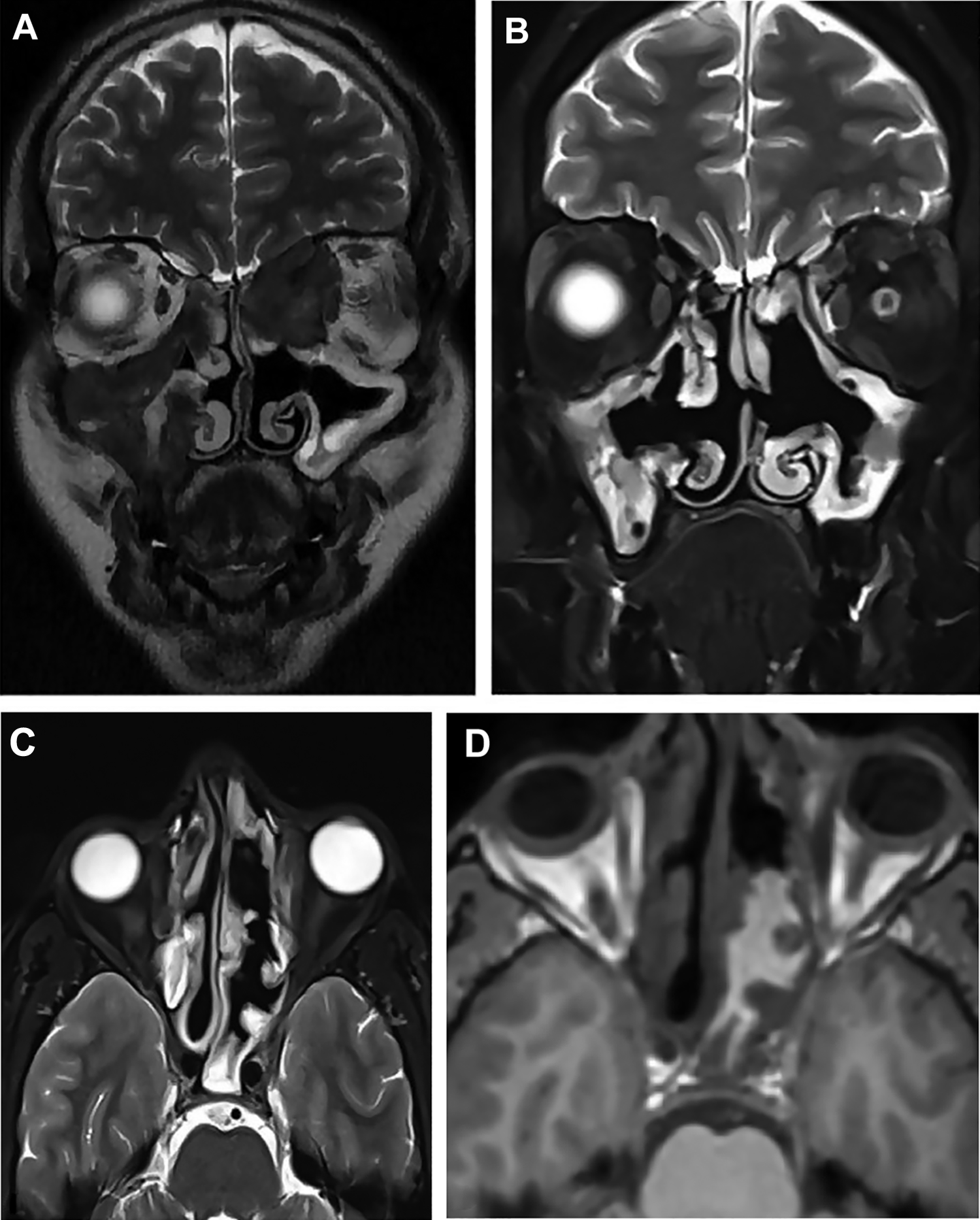
Magnetic resonance images (MRIs) of the paranasal sinus (A with a histopathologically confirmed diagnosis of chronic granulomatous invasive fungal sinusitis; and B, C, and D with confirmed diagnosis of allergic fungal rhinosinusitis). A, T2-weighted MRI in the coronal plane showing a hypointense lesion in the bilateral maxillary and ethmoid sinuses extending into extraconal fat. B, T2-weighted MRI in the coronal plane showing resolution of the previously noted lesion. C, T2-weighted MRI in the axial plane showing a signal void occupying the posterior ethmoid and sphenoid sinuses, a characteristic finding of dehydrated fungal elements and mucin. D, T1-weighted MRI at the same level as (C), showing a hyperintense lesion.
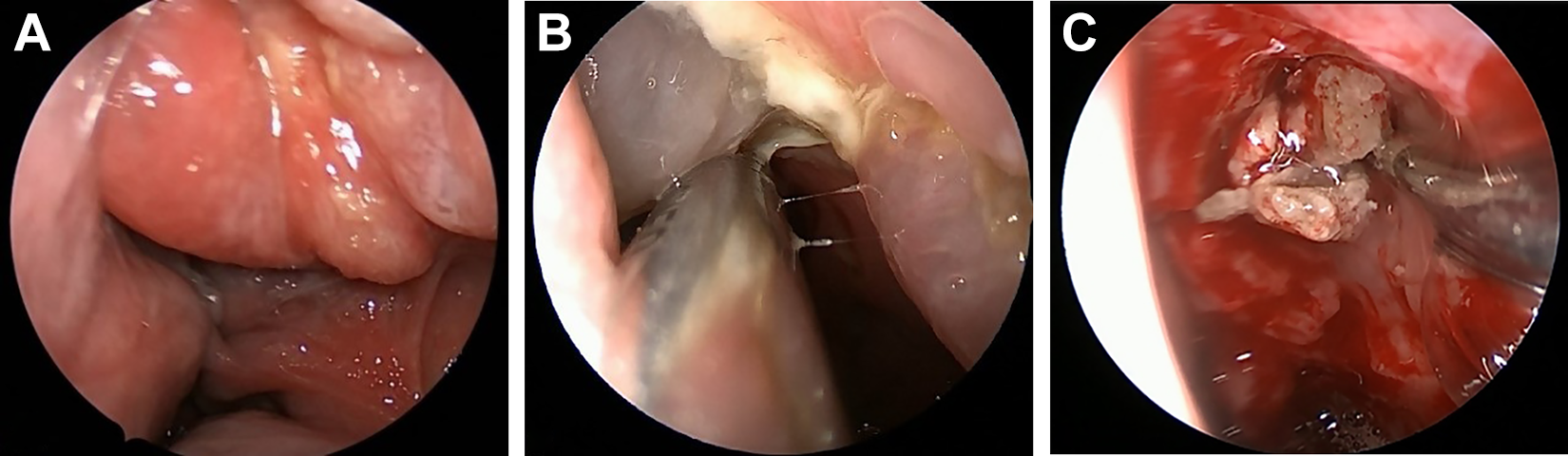
Intraoperative endoscopic appearance of the disease (A with confirmed chronic granulomatous invasive fungal sinusitis, and B and C with confirmed diagnosis of allergic fungal rhinosinusitis). A, Endoscopic image showing the mass occupying the left ethmoid cavity. B, Polyps with mucinous discharge occupying the left ethmoid cavity. C, Image obtained post-polypectomy showing mucin and fungal debris filling the left ethmoid cavity.
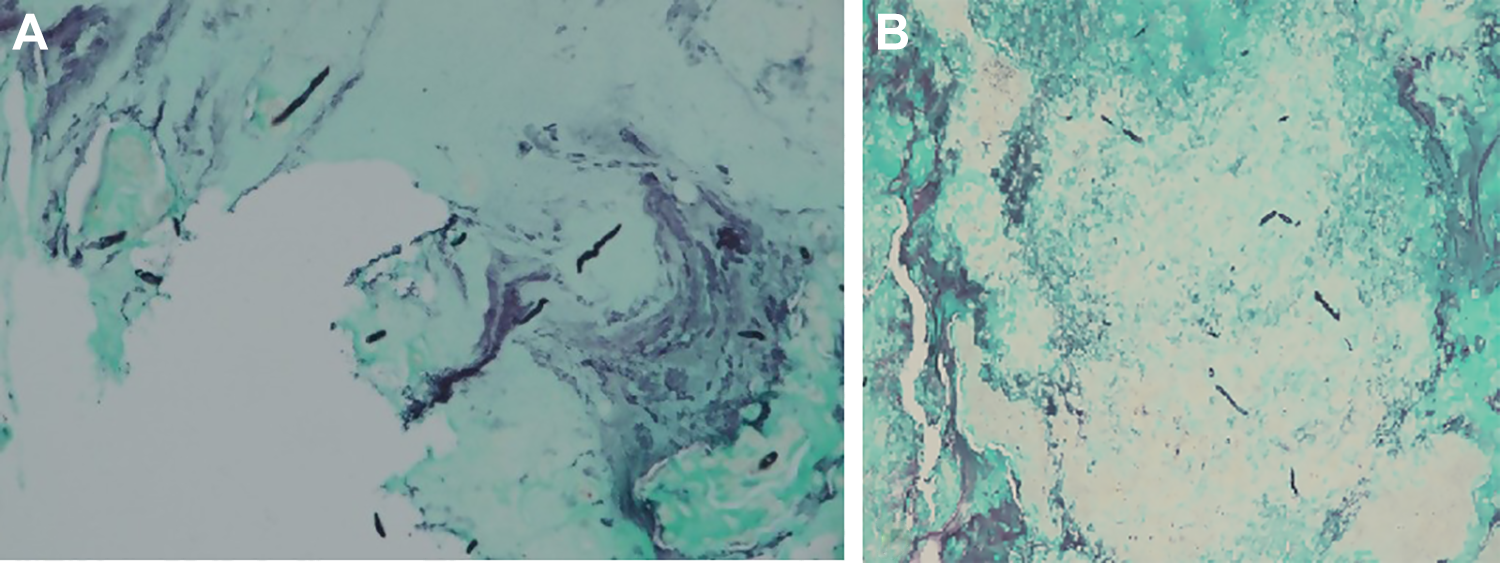
Microscopic view of the histological slides stained with Grocott’s methenamine silver (GMS) stain. A, The slide reveals branching septate fungal hyphae invading the underlying mucosa and submucosa. B, The same branching septate hyphae with a background of mucin without invasion, confirming the diagnosis of allergic fungal sinusitis.
Case 6
A 42-year-old male presented with progressive swelling at the left medial canthus, which had lasted for 6 months. An incisional biopsy was taken by an ophthalmologist at another hospital, and the patient was diagnosed as having CGIFS. Aspergillus flavus was seen on culture. The patient reported having undergone ESS more than 10 years previously, for which there were no available reports. Nasal endoscopy showed left middle meatus polyps with a normal right nasal cavity. Left medial canthal swelling, with normal ocular movement and visual acuity, was observed. No abnormality was found on neurological examination. Both CT and MRI showed a left anterior ethmoid lesion eroding through the ethmoid roof and lamina papyracea with focal intracranial extradural and intraorbital extraconal extension. The patient was booked for surgical debulking and started on oral voriconazole. After 1 week of antifungal treatment, the medial canthus swelling dramatically improved, and in view of this, the decision to postpone the surgery and continue antifungal treatment was agreed with the infectious disease and neurosurgery teams. A CT was done at the 3-month follow-up. It showed evidence of regression and a good response to the antifungal regimen. The MRI taken at the 6-month follow-up showed a significant improvement, with minimal intracranial residual and no reported symptoms. The patient missed his subsequent appointments, so no further follow-up information was obtained.
Case 7
A 40-year-old female presented with left nasal blockage and discharge associated with an infraorbital swelling for the previous 3 months. She had undergone 3 sinus surgeries, including endoscopic and external approaches, at other hospitals. The last surgery was done 1 month prior to her presentation and CGIFS was diagnosed. Endoscopic examination revealed a pale mass in the left maxillary sinus. Infraorbital swelling, pushing the orbit superiorly with normal extraocular movement and visual acuity, was noted. Both CT and MRI showed the lesion extending to the left cheek, extraconal fat, and pterygopalatine fossa. The patient underwent ESS to debulk the lesion. Histopathological diagnosis of CGIFS and fungal culture of A flavus were confirmed. Postoperatively, the patient was placed on oral voriconazole. At review 7 months later, there was clinical evidence of complete resolution of the disease.
Discussion
Main Findings of the Study
In our series, 4 of the cases were females and 3 were males. Six cases were considered to be young adults, ranging in age between 29 and 42 years. All these cases were managed by different rhinologists at different tertiary centers in Saudi Arabia. The mean duration of symptoms was 5.8 months, ranging from 3 to 12 months. All the patients were immunocompetent, except the patient in case 1. Orbital complaints were the most frequent presenting symptoms, including proptosis, infraorbital swelling, and diplopia. These symptoms were present in 5 patients. Intracranial extension was noted in 2 patients. Invasions of the cheek, pterygoid bone, and pterygopalatine fossa were documented in 3 patients. Aspergillus flavus was found to be the causative pathogen in 6 patients. The patient in case 4 had a different Aspergillus species: A nidulans. This is the first case of CGIFS primarily involving the ethmoid sinus reported to be caused by this species. This patient underwent surgical debulking but refused antifungal treatment. The other 6 patients received oral voriconazole, 200 mg twice daily, with a mean duration of 5.6 months. The patient in case 5 took a course of nasal voriconazole drops for 6 months as an adjunct to the oral regimen. Only 1 death was reported, of an immunocompromised patient with intracerebral disease (case 1). The rest of the cases showed either resolution or regression of the disease. Two patients were lost to follow-up. The remaining patients still have regular office visits and are disease-free to date.
Comparison With Other Studies: Epidemiology and Clinical Presentation
DeShazo et al defined invasive fungal sinusitis based on histological evidence of fungal hyphae within the tissue. 7 Invasive fungal rhinosinusitis can be acute or chronic. The chronic form is diagnosed if the symptoms have persisted for more than 12 weeks. The chronic form is further subdivided into nongranulomatous and granulomatous subtypes. The granulomatous form is histopathologically characterized by noncaseating granulomas with foreign bodies or giant cells, vasculitis, vascular proliferation, and perivascular fibrosis. 7 The vast majority of cases of invasive fungal sinusitis are immunocompromised, though interestingly, the granulomatous subtype affects immunocompetent individuals. 2 Chronic granulomatous invasive fungal sinusitis is typically diagnosed in patients from Sudan, India, Pakistan, and Saudi Arabia. Aspergillus flavus was the most commonly identified causative organism. 2,8 -10
Clinically, a patient having CGIFS may have all the symptoms of chronic rhinosinusitis. 7 In a Saudi Arabian study of 6 granulomatous and 17 nongranulomatous cases of chronic invasive fungal sinusitis, the most common symptom was nasal obstruction (87%), followed by proptosis. The ethmoid sinus was the most commonly affected sinus. 11 This is in line with our series, where ethmoidal involvement was found in 5 cases. Despite their critical location, lesions occupying the sphenoid sinus can be overlooked by physicians in other specialties, since they tend to be asymptomatic until they are evaluated by an otorhinolaryngologist. 12 The delay in the diagnosis may lead to a worse prognosis due to the high likelihood of intracranial spread. 13
Siddiqui et al classified the patterns of invasive fungal sinusitis in immunocompetent patients into 3 types. The first type is intracerebral aspergillosis, which has the poorest prognosis. The second type is intracranial extradural aspergillosis, which has an intermediate prognosis. The best prognosis is with the third type: orbital and cranial base aspergillosis. 14 In our series, 1 of the 2 patients with intracranial involvement died (from intracerebral disease), while the other patient continued to be in a stable condition (extradural disease) for at least 6 months of follow-up.
Medical and Surgical Treatment Modalities
The combination of surgical debridement and antifungal therapy is the mainstay of disease management, as they are considered to be the most important factors for survival. 12 According to the Infectious Diseases Society of America, voriconazole is the drug of choice for the treatment of invasive aspergillosis. 15 With regard to CGIFS, Rupa et al recently published a current therapeutic protocol and reported that azole derivatives (voriconazole or itraconazole) were consistently better than amphotericin B. 2 The duration of oral voriconazole treatment is still debatable; typically, it ranges from 6 to 18 months. 16,17
In the literature, topical antifungal application has no clear role as an adjuvant mode of therapy in CGIFS cases. We introduce the first case in which oral and nasal voriconazole were used, with an excellent response. Although there is no clear indication for combination systemic therapy in the literature, we administered voriconazole and caspofungin in case 1 to provide a synergistic effect, as suggested by Takahashi et al. 18
Surgery is aimed at slowing the progression of the disease, reducing the fungal load, and providing a specimen for culture and histopathological diagnosis. However, there is a lack of studies regarding surgical options and their outcomes in CGIFS, and most of the studies are based on nongranulomatous invasive fungal disease. 16 -18
Recently, Rupa et al have suggested a protocol for CGIFS management based on a staging system using clinical features and radiological findings of the disease extent. 2 In stage 1, the disease is confined to the nose and the PNSs. In stage 2, it extends to the orbit, the palate, or the oral cavity. In stage 3, it extends to the brain, pterygopalatine fossa, cavernous sinus, cheek, or periorbital area. Stages 1 and 2 are managed with excisional surgery (endoscopic for stage 1 and endoscopic and/or open resection for stage 2), and either itraconazole or voriconazole. Stage 3 is managed using a combined endoscopic and open approach with craniofacial resection for anterior skull base involvement, as well as voriconazole treatment. 2 However, in some cases, the radical and complete removal of all the diseased tissue could lead to significant morbidity and a possible risk of mortality when critical neurovascular structures are involved. Based on our experience to date, if feasible, we recommend using sinonasal endoscopic excision as the first step in managing these cases along with systemic and topical forms of voriconazole treatment. More aggressive forms of surgery, including enucleation and open craniofacial resection, would be reserved for patients failing with the above management.
Unique Transformation Into AFRS
In our case series, one Sudanese patient developed AFRS after resolution of his initial CGIFS (case 5). To the best of our knowledge, the transformation of CGIFS to AFRS has not yet been reported in the literature. Conversely, Edelmayer et al recently reported the first case in which AFRS was transformed into GCIFS. It developed in an African American male patient after he received multiple courses of systemic steroids. 19 However, in our case, the patient had a surgical history of ESS that was performed 6 years prior to his presentation, with no available reports. This can be interpreted as him having AFRS initially, which transformed into CGIFS and then reverted to AFRS. Although it is concerning that systemic steroids could possibly cause a transient form of immunodeficiency in the presence of certain fungal species with invasive potential, leading to the development of CGIFS, it remains a theory at this stage and is difficult to prove.
Limitations of the Study
One limitation of our study is the heterogeneity of the medical and surgical treatment protocols. This is due to multiple factors, including different pathology locations, the degree of invasion, and the surgeon’s preference. Because there is no consensus on the optimal management of CGIFS, the treatment plan should be tailored to each case. The retrospective design of this study is another limitation. Prospective multi-institutional studies are warranted in the future to develop management protocols for such rare entities.
Conclusion
Chronic granulomatous invasive fungal sinusitis is a morbid and possibly fatal disease. The etiology of this disease and its relationship to AFRS is still debatable. Early diagnosis is an important element of disease management. A multidisciplinary approach with a combination of surgery and antifungal agents is crucial for controlling these destructive infections. Topical application of antifungal medication may play a role in their management. The type of surgery should be tailored according to the extension of the disease. Our limited experience shows that endoscopic surgical debulking or excision, if feasible, has led to favorable results even in cases with orbital invasion. Because CGIFS remains a rare disease, more studies are needed to improve patient outcomes.
Footnotes
Authors’ Note
Saad Alsaleh is considered a cofirst author and contributed equally to the first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.