
Abstract
Objective:
To investigate the effect of drug treatment combined with psychological intervention on mental disorders in patients with persistent moderate–severe allergic rhinitis.
Methods:
Sixty patients with persistent moderate–severe allergic rhinitis who met the criteria were randomly divided into 2 groups: control group and experimental group. The control group was only given medication, whereas the experimental group was given psychological intervention on the basis of the same medication. Cognitive behavioral therapy was used for psychological intervention. After 12 weeks of treatment, Self-Rating Anxiety Scale (SAS), Self-Rating Depression Scale (SDS), and rhinoconjunctivitis quality of life questionnaire (RQLQ) were used to evaluate the changes in anxiety, depression, and quality of life before and after treatment.
Results:
The SAS and SDS scores of the control group after treatment were lower than those before treatment, and the difference was statistically significant. Similarly, the SAS and SDS scores of the experimental group after treatment were lower than those before treatment with statistically significant difference. In addition, after treatment, the SAS and SDS scores of the experimental group were statistically lower than those of the control group. The results of RQLQ showed that the scores of each dimension in the control group after treatment were lower than those before treatment, and the difference was statistically significant. Similar results were found in the experimental group. After treatment with these 2 different schemes, the RQLQ scores of sleep, nonnasal/eye symptoms, and emotion in the experimental group were statistically lower than those in the control group.
Conclusion:
Drug therapy or drug therapy combined with psychological intervention can alleviate anxiety and depression of patients with persistent moderate–severe allergic rhinitis and improve their quality of life. Moreover, based on the effect of improving mental disorder and quality of life of patients, drug therapy combined with psychological intervention is better than drug treatment alone.
Introduction
Allergic rhinitis (AR) is a type I allergic reaction of nasal mucosa mediated mainly by IgE after exposure to allergens. As one of the most common respiratory diseases, AR affects 10% to 25% of people worldwide. Due to the gradual change in medical model, in the process of exploring AR, AR has been found to have not only physical symptoms but also psychological symptoms. 1 The main physical symptoms of patients with AR are as follows: nasal itching, nasal obstruction, runny nose, paroxysmal sneezing, and so on, which may have different effects on the quality of life of patients with AR. 2 -4 The need for long-term medication to treat the nasal symptoms of patients with AR, in the long run, will affect the physical and mental health of patients and their quality of life. 5 Most research results have shown that the physical symptoms and mental disorders could interact with each other, which further aggravates these 2 aspects and may eventually have a negative impact on the quality of life of patients with AR. Allergic rhinitis can be classified into mild and moderate–severe types. Moderate–severe AR can be determined as one or more of the following: (1) unable to sleep properly, and daily activities, physical exercise, and entertainment are affected; (2) unable to work or study properly; and (3) having annoying symptoms. 6 Additionally, patients with persistent moderate–severe AR have longer course of disease and more severe somatic symptoms than other types of AR. Therefore, the degree of mental disorder in these patients is more serious than other types of patients with AR, and their quality of life is worse, which is in urgent need of improvement.
However, the main prevention and treatment methods of AR nowadays are avoiding allergens, drug therapy, specific immunotherapy, and surgery, and drug therapy is the most commonly used method. Although these treatment methods have been proved to be effective, there are still some deficiencies in the evaluation of psychological condition, quality of life, and relevant psychotherapy of patients. Psychological disorder is one of the key factors affecting the treatment and prognosis of AR. Therefore, the improvement in psychological condition in the treatment of patients with AR should be paid more attention.
At present, most studies have focused on the correlation between AR and psychological factors, the types of mental disorders in patients with AR, or the pathogenesis of neuropsychology, endocrine, and immunology. Nevertheless, there are relatively few studies on the efficacy of psychological intervention in patients with AR, and psychological intervention has not been included in the guidelines for the diagnosis and treatment of AR. Therefore, the purpose of this study is to investigate the effect of drug therapy combined with psychological intervention on the improvement in mental status of patients with persistent moderate–severe AR, to provide theoretical basis for the psychological intervention treatment, further to provide new strategies for the prevention and treatment of AR.
Method
Data and Selection Criteria
Clinical data
Sixty-seven patients with persistent moderate–severe AR who met the admission criteria from June 2016 to September 2016 were selected. Sixty-seven patients were randomly divided into control group and experimental group, and 60 of them completed 12 weeks of treatment. There were 30 patients in the control group (11 males and 19 females), aged 18 to 60 years, with an average age of 38.77 ± 10.29 years. In the experimental group, there were 30 patients (9 males and 21 females), aged 18 to 60 years, with an average age of 37.40 ± 10.25 years. Studies have suggested that gender and age have no significant effect on the mental state of patients with AR. 7 -9 So there was no significant difference in age and gender between the 2 groups (P > .05).
Inclusion criteria
Patients aged between 18 and 60, with normal cognitive function, no interpersonal communication disorders, and able to cooperate with the study. According to the diagnostic criteria and clinical classification criteria of persistent moderate to severe AR proposed in the guidelines for the diagnosis and treatment of AR
10
: ① Diagnostic criteria. Nasal itching, nasal obstruction, clear water-like runny nose, and paroxysmal sneezing are the main symptoms, accompanied by eye symptoms, such as itching, tearing, red eyes, and burning sensation; nasal endoscopy revealed pale and swollen nasal mucosa, edema of inferior turbinate, and more water-like secretions in nasal cavity; serum-specific IgE was positive. ② Clinical classification criteria. The duration of symptoms onset ≥4 days/week and ≥4 consecutive weeks; the severity or severity of symptoms has a significant impact on the quality of life.
Exclusion criteria
Suffering from hypertension, diabetes, and chronic diseases of heart, lung, liver, and kidney. Primary mental and psychological diseases. Suffering from other organic diseases that may cause mental disorders, such as tumors, neurological or craniocerebral diseases, and acute or chronic severe trauma. There were acute infectious diseases in the past week. Major life changes have taken place recently. Patients who have received psychotherapy or used psychotropic drugs in the past 6 months. Pregnant or lactating women. Those who have missing items or fall off automatically in the answer sheet.
Scales and Questionnaires of Research
Self-Rating Anxiety Scale
Self-Rating Anxiety Scale (SAS) is commonly used to test the severity of anxiety in patients and the changes of anxiety in patients undergoing psychotherapy, but SAS cannot be used as a diagnostic basis for anxiety disorders. 11 Self-Rating Anxiety Scale consists of 20 questions, which mainly evaluates the frequency of each question. There are 4 options under each question and each question corresponds to the 4 scores of “1, 2, 3, 4”. After completing the test, the total score is multiplied by 1.25, and the integral part of this result is taken as the standard score. According to the results of the Chinese norm, the demarcation value of the SAS standard score is 50, that is to say, if the score is ≥50, the patients can be judged to be in a state of anxiety. In this study, SAS was used to assess anxiety status of patients with persistent moderate–severe AR before and after treatment.
Self-Rating Depression Scale
Self-Rating Depression Scale (SDS) is usually used to assess the severity of depression. 12 Similar to SAS, SDS includes 20 questions and calculates scores in the same way as SAS. According to the Chinese norm, the standard demarcation value of SDS is 53. In this study, SDS was used to assess the depressive state of patients with persistent moderate–severe AR before and after treatment.
Rhinoconjunctivitis Quality of Life Questionnaire
Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) is widely used to evaluate the quality of life of patients with AR. 13 The standard version of RQLQ (for adults older than 18 years) consists of 28 items in 7 dimensions, each of which is evaluated with a score of 0 to 6. After the patients completed the test, the scores of each item of the 7 dimensions were added up separately, and the total scores of each dimension were finally obtained. Rhinoconjunctivitis Quality of Life Questionnaire contains different and distinct scoring content, which can reflect the state of physical symptoms, emotions, and daily life of the patients. In this study, RQLQ was used to assess the quality of life of patients with persistent moderate–severe AR before and after treatment.
Research Methods
Measurement of anxiety, depression, and evaluation of quality of life before treatment
Before the implementation of the treatment, SAS and SDS were used to assess the anxiety and depression status of the 2 groups, and RQLQ was used to evaluate the quality of life of the patients. Before the evaluation, all patients were explained the specific contents of these 3 scales in detail, and self-evaluation was conducted honestly according to the actual situation. If there are patients with special diseases, low educational level, and other special circumstances that cannot be completed by themselves, the researchers should explain and ask questions one by one, record the answers, and do not give inductive questions and answers during the inquiry process. All patients are ensured to complete these 3 scales on the spot, which are checked by researchers to ensure that the final scales are qualified.
Treatment
Control group
According to the first-line combination of agents recommended in the guidelines for the diagnosis and treatment of AR 10 (nasal glucocorticoids + antihistamines), mometasone furoate nasal spray (usage: nasal drops, 2 pinches per nostril, once a day) and loratadine tablets (usage: 10 mg, once a day) were selected.
Experimental group
Patients were given the same drug treatment as the control group, and psychological intervention was performed. In this study, cognitive behavioral therapy (CBT)
14
was used as the method of psychological intervention. The specific implementation methods were as follows:
Process. Once a week, 30 to 60 minutes a time, a total of 12 times.
Ways: Face-to-face teaching, telephone or network contact, and so on.
Contents. ① The first intervention mainly includes the following 3 steps:
First, rebuilding cognition: after the researchers have made a detailed understanding and analysis of condition of patients, they will explain the cause, development process, treatment, and prognosis of AR to the patients in detail, so as to relieve their doubts about AR and establish a correct understanding.
Second, emotional counseling: researchers should explain the relationship between AR and mental disorders to patients in detail and point out that mental disorders, especially anxiety and depression, will have adverse effects on the condition of patients. Through adequate communication, patients can be given psychological counseling, support, and help, and patients are advised to eliminate bad emotions in various ways.
Finally, behavioral correction: researchers should explain to patients the role of drugs used in this treatment, as well as possible drug reactions and corresponding treatment measures, so that patients can remove all kinds of concerns about medication and can actively adhere to regular medication. ② The 2nd to 12th interventions in the future include the following 2 steps:
The first step is still emotional counseling, but it is different from the first intervention. Before the intervention, researchers should be aware of the psychological changes, whether patients take medicine regularly during the period, the changes of their symptoms, and the changes of daily life. Then the above questions are given to the patients to answer and again given psychological counseling, so that the patients deeply understand their bad emotions and behavior and actively change these.
Second, relaxation training: instruct patients to sit or lie in bed quietly and comfortably, to get rid of mental distractions, to breathe and relax, to maintain physical and mental tranquility, and to let patients enjoy light music with slow rhythm.
Measurement of anxiety, depression, and evaluation of quality of life after treatment
At the end of treatment, SAS, SDS, and RQLQ were evaluated again after each patient. The evaluation method is the same as before treatment, and all patients are ensured to complete 3 scales on the spot, which are checked by researchers to ensure that the final scale is qualified.
Statistical Analysis
The data collected in this study were processed and analyzed by SPSS19.0 software. The measurement data were described with mean ± standard deviation, which was compared by t test. The difference was statistically significant at P < .05.
Results
1. Drug therapy combined with psychological intervention can improve the psychological condition of patients with anxiety and depression.
Before treatment, the results of SAS and SDS scores showed that there was no significant difference between the control group and the experimental group. The SAS and SDS scores of the control group after treatment were significantly lower than those before treatment. Similar results were found in the experimental group after treatment. Furthermore, the results after treatment showed that the SAS and SDS scores of the experimental group were lower than those of the control group, and the difference was statistically significant (Figures 1 and 2).
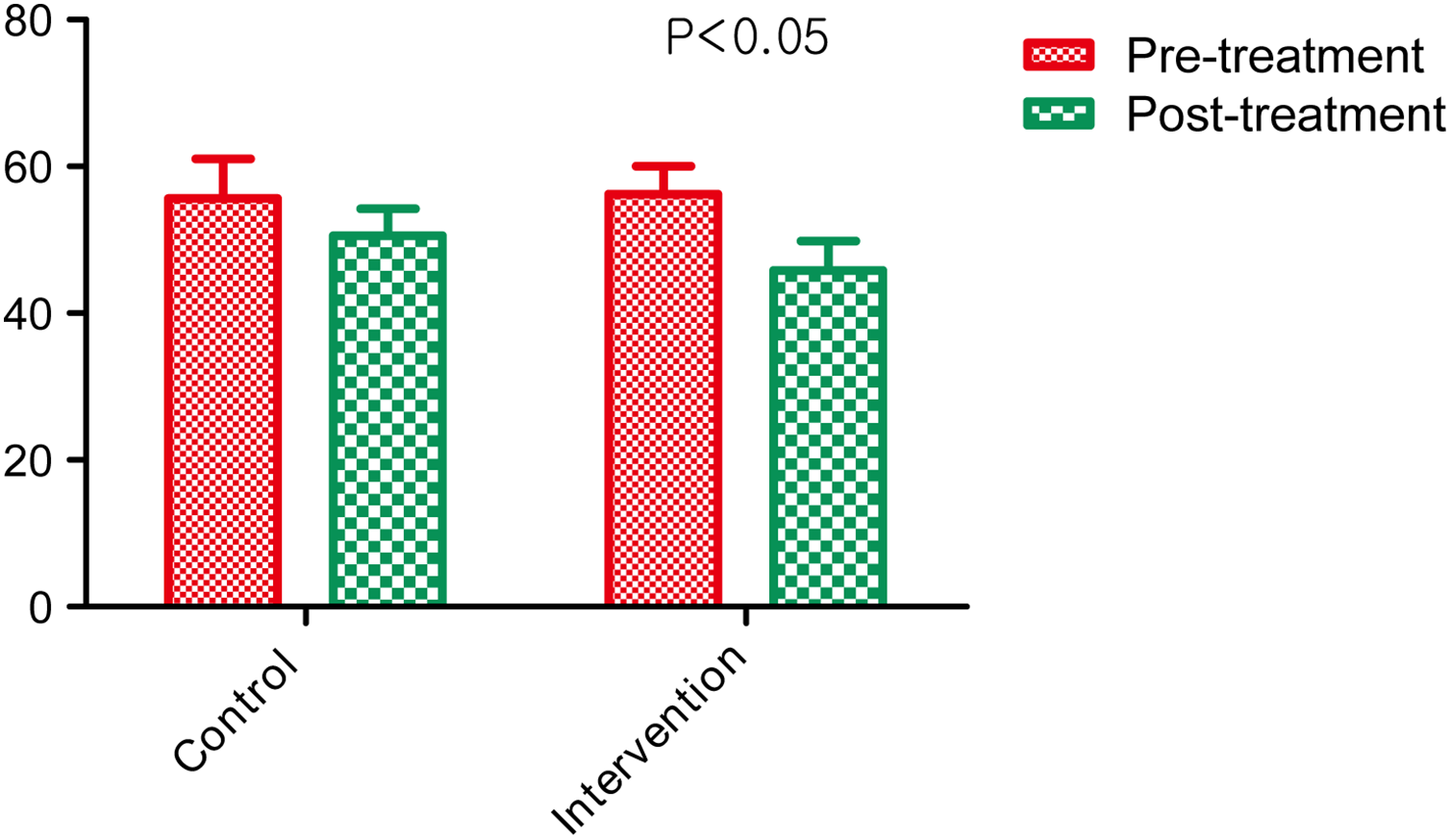
Comparison of Self-Rating Anxiety Scale scores between 2 groups before and after treatment.
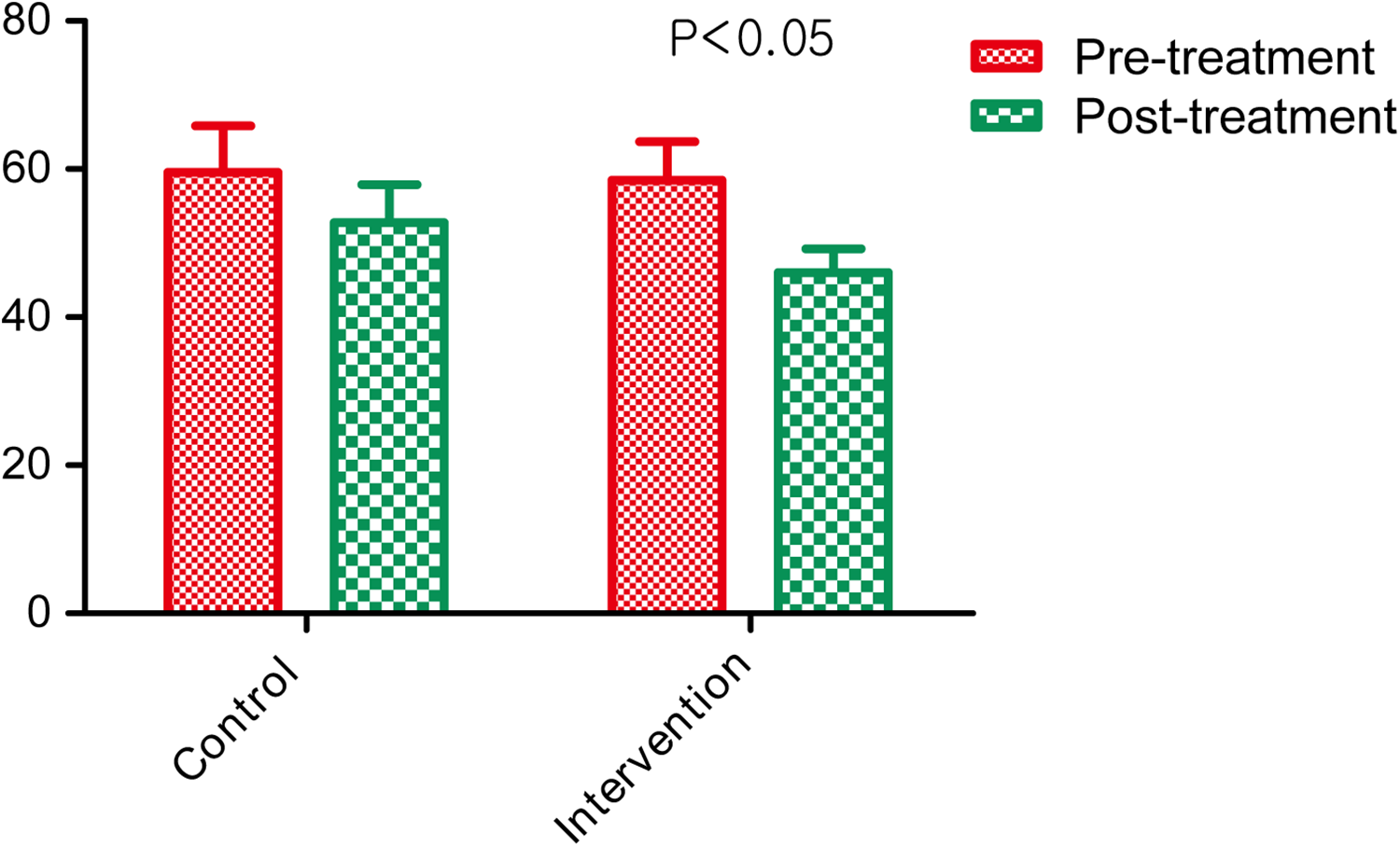
Comparison of Self-Rating Depression Scale scores between 2 groups before and after treatment.
2. The RQLQ score was reduced in both the control group and the experimental group after treatment.
After treatment, the RQLQ scores of 7 dimensions of the patients in the control group were lower than those before treatment, and the difference was statistically significant (Figure 3). Similarly, the RQLQ scores of 7 dimensions of the experimental group after treatment were statistically lower than those before treatment (Figure 4).
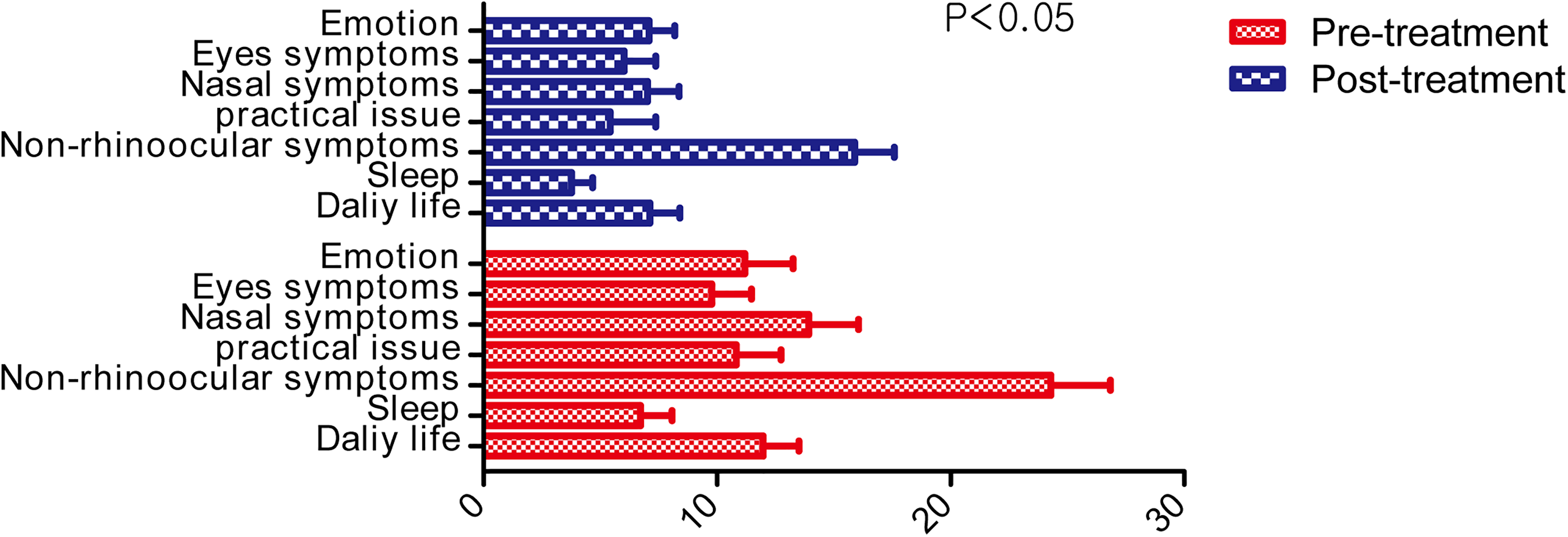
Comparison of Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) scores of patients in control group before and after treatment.
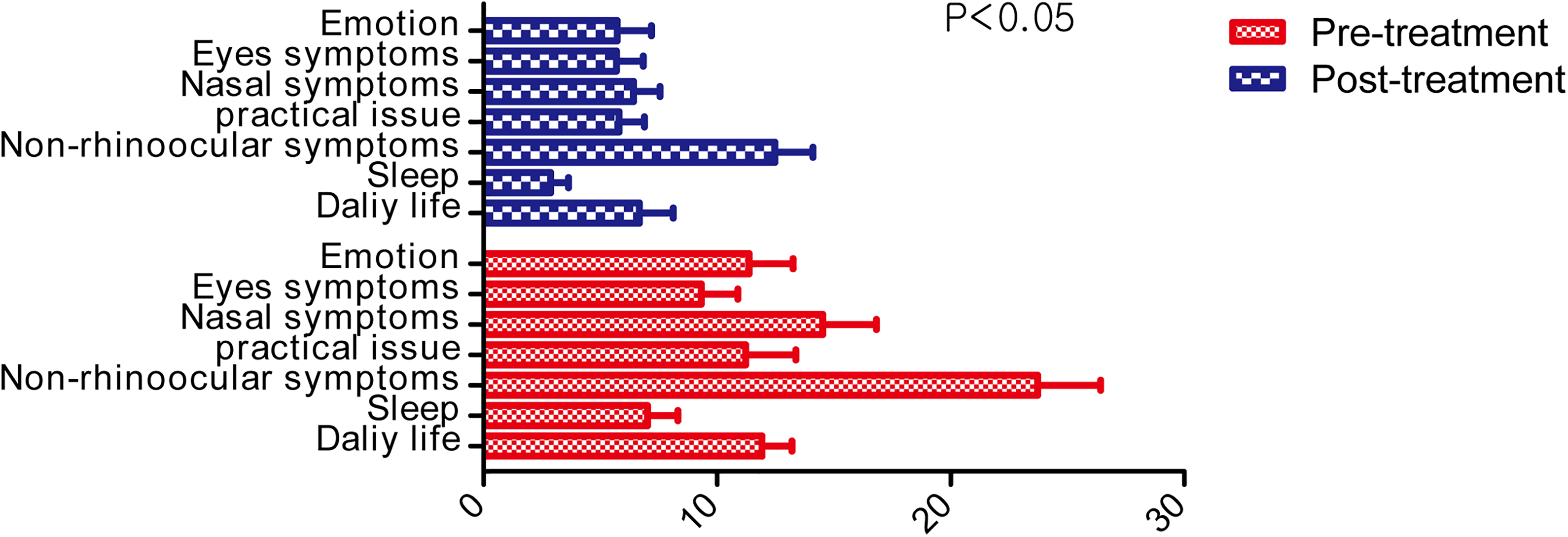
Comparison of Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) scores of patients in the experimental group before and after treatment.
3. The 3 RQLQ dimensions of sleep, nonnasal/eye symptoms, and emotions in the experimental group were improved.
After treatment with 2 different schemes, the scores of sleep, nonnasal/eye symptoms, and emotions in the experimental group were lower than those in the control group, and the difference was statistically significant. However, there was no significant difference in RQLQ dimensions of daily life, practical problems, nasal symptoms, and eye symptoms between the experimental group and the control group (Figure 5).
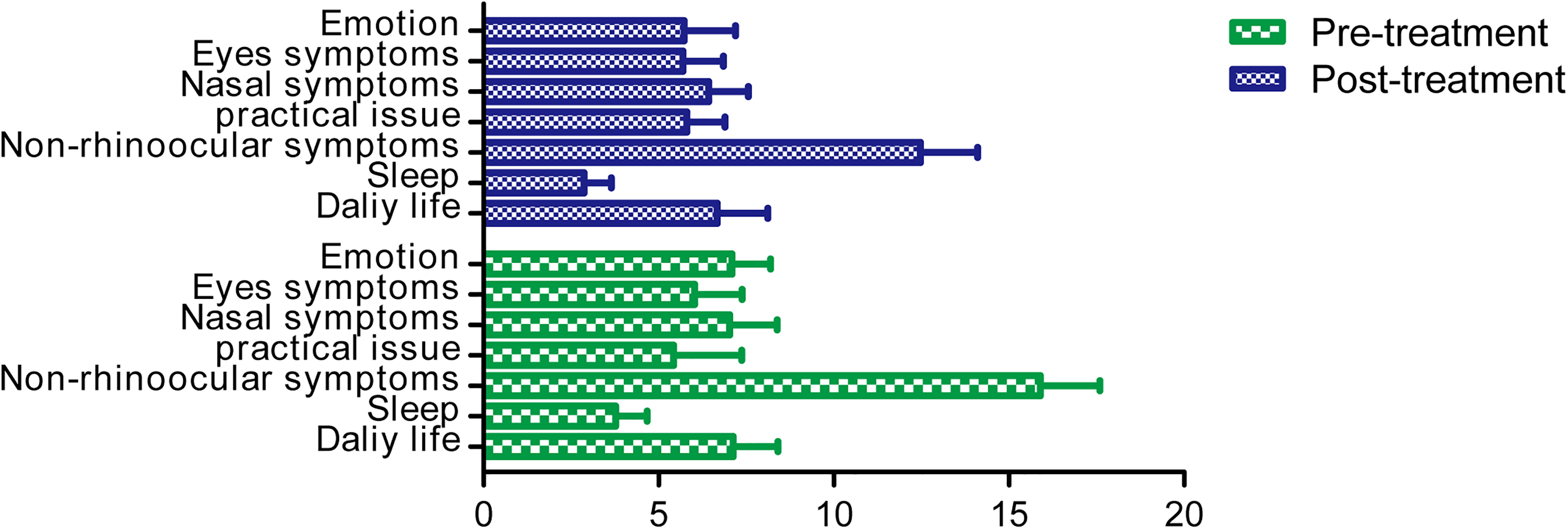
Comparison of Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) score between the control group and experimental group after treatment.
Discussion
Allergic rhinitis is closely related to mental disorders and may affect the quality of life of patients. It is reported that although AR does not directly cause death, if its symptoms recur for a long time, it will lead to a series of mental disorders such as anxiety and depression and ultimately reduce the quality of life of patients. Psychological disorders can disrupt the immune system of the body, resulting in more serious physical symptoms in patients with AR. Subsequently, more serious physical symptoms will produce a large number of negative emotions, thus forming a vicious circle. 15 Therefore, we can not only pay attention to its symptoms but also ignore their mental disorders. It has been pointed out that doctors often have a lower estimate of the mental state of patients with AR. If they pay attention to the mental and psychological problems of patients with AR and intervene appropriately, they may play a role in the treatment of AR. 16 Therefore, it is necessary to give psychological evaluation and corresponding psychological intervention to patients with AR while giving drug treatment.
The recent research results showed that anxiety and depression were the 5 most relevant psychological factors for patients with AR, and these 2 factors are most related to AR. 17,18 Furthermore, a literature review on the relationship between AR and adverse emotions has been conducted and results showed that the proportion of patients with AR whose somatic symptoms are related to anxiety and depression is quite high, 99.9% and 97.1%, respectively. 8 Besides, among all patients with AR, patients with persistent moderate–severe AR have the most serious physical symptoms and frequent mental disorders, which cause the most obvious impact on their lives. Thus, this study focused on anxiety and depression in patients with persistent moderate–severe AR, which were given corresponding psychological intervention. Psychological intervention can enable patients to obtain significant psychological counseling and support, improve their psychological endurance, maintain a good mental state in the course of treatment, and reduce the occurrence of negative psychological and social adaptation adverse reactions, thus helping to improve the recovery rate of patients. 19 At present, there are many methods of psychological intervention, but there is no clear and consistent standard on how to classify them. According to the emphases of intervention, it can be divided into 3 categories 20 : psychological counseling and psychotherapy, health education, and comprehensive reproductive health education and intervention plan. Cognitive behavioral therapy is widely used in this study. Its purpose is to try to correct the dysfunctional thinking of patients and further correct their behavior by changing their thinking and psychological state. Therefore, combined with the actual situation of patients with persistent moderate–severe AR, our study formulated the CBT implementation programs described above.
Both SAS and SDS were used in this study to evaluate the anxiety and depression of 60 patients with persistent moderate–severe AR before and after treatment. The results showed that SAS and SDS scores of patients with AR in both groups after treatment were statistically lower than those before treatment, indicating that drug treatment or combination of psychological intervention can improve anxiety and depression in patients with persistent moderate–severe AR. These results may be related to the fact that mental disorders in patients with AR are mainly affected by their physical symptoms. In this study, most nasal symptoms and complications of patients can be controlled or even alleviated to varying degrees after using drugs in 2 groups, which can improve their anxiety and depression. On the other hand, the SAS and SDS scores of the experimental group were statistically lower than those of the control group after treatment, indicating that psychological intervention based on drug treatment was better than drug treatment alone in improving anxiety and depression of patients with persistent moderate–severe AR. Studies have shown that at least two-thirds of patients with AR suffer from anxiety, conflict, and conflicting emotions because of a long-term medication of nasal glucocorticoids. 21 When using drugs alone, some patients may be unable to adhere to the long-term and regular use of drugs because of the lack of AR-related knowledge and misunderstanding of the drugs. Finally, the physical symptoms of AR cannot be well controlled, and the improvement in mental disorders is not obvious or worse than before treatment. Psychological intervention on the basis of drug treatment can help patients understand their own diseases fundamentally, reduce their worries and prejudices about long-term drug use, and also effectively help patients dispel bad emotions. These may be the reason why the SAS and SDS scores of the experimental group after treatment were lower than those of the control group. Therefore, psychological intervention can help patients understand AR, recognize the need for long-term regular use of drugs, and recognize the safety and tolerance of nasal glucocorticoids. So that patients can establish a correct understanding of the disease, reduce the adverse effects of wrong perception on treatment, and then learn how to better control their own behavior, such as active regular medication, and learn how to adjust mentality and release anxiety, depression, and other emotions.
Some studies suggest that the quality of life of patients with persistent moderate–severe AR is the worst. 22,23 In this study, RQLQ was used to evaluate the quality of life of all patients before and after treatment, including 28 items in 7 dimensions. The results demonstrated that the RQLQ scores of the 2 groups after treatment were lower than those before treatment, indicating that the 2 treatment schemes in the study had significant effect on improving the quality of life of patients with persistent moderate–severe AR. This may be mainly related to drugs that can alleviate nasal symptoms in patients with AR, as a study has shown that nasal symptoms and real-life problems were the 2 aspects that have the greatest impact on the quality of life of patients with AR. 24 The nasal symptoms of patients with AR were improved by medication, and their mental disorders would be improved accordingly, so that the quality of life would be improved. In addition, after treatment, the scores of sleep, nonnasal/eye symptoms, and emotional dimensions in the experimental group were statistically lower than those in the control group, whereas the scores of daily life, practical problems, nasal symptoms, and eye symptoms in the experimental group were not significantly different from those in the control group. The reason may be that sleep, nonnasal/eye symptoms, and emotions are related to psychosocial assessment items. Psychological intervention based on drug therapy can better improve mental disorders in patients with AR. Therefore, the experimental group scored only lower in these 3 dimensions, but there was no significant difference in the other 4 dimensions. Our study suggested that psychological intervention could guide patients with AR to acquire correct knowledge of the disease, correct their bad behavior, and relieve the bad mood of patients with AR. Psychological intervention based on drug treatment has achieved more significant effect than drug treatment alone in the study of improving the quality of life of patients with persistent moderate–severe AR.
Recently, with the gradual increase in life pressure, mental disorders will be more common than before. Under these current situations, AR has become a common global disease, and psychosocial factors are closely related to the occurrence and progression of AR. Not only the physical symptoms of patients with AR should be treated but also the mental and psychological state of patients should be fully understood. Using scientific methods to evaluate the mental state and quality of life of patients with AR and give appropriate psychological intervention improves the mental state of patients with AR and ultimately improves the overall quality of life of patients with AR. Taken together, how to further improve the psychological assessment methods and individualized treatment system of patients with AR will become the direction of our future research.
Conclusion
In conclusion, drug therapy alone or drug therapy combined with psychological intervention can alleviate anxiety and depression in patients with persistent moderate–severe AR in this study and improve their quality of life. Furthermore, in terms of the effect of improving the mental disorder and quality of life of these patients, psychological intervention based on drug treatment is better than drug treatment alone. Drug therapy combined with psychological intervention will be a new effective strategy to prevent and treat AR in the future.
Footnotes
Authors’ Note
Li-Xin Wang and Zhi-Chao Yang contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.