
Abstract
Needle biopsy is a well-established component in the evaluation of thyroid nodules. The biopsy is usually performed with an ultrasound guidance and consists of either fine-needle aspiration or core needle biopsy. Although these terms are often used interchangeably, their difference is important. To our knowledge, we discuss the first reported case of biopsy-proven laryngeal nerve injury and permanent vocal fold paralysis following ultrasound-guided core biopsy of the thyroid. We advocate this complication be discussed as part of the consent process.
Keywords
Introduction
Aspiration biopsy has been used in practice for over 150 years and has become an effective technique used in the diagnosis of nodular thyroid disease. Aspiration biopsy, also called “needle biopsy,” can be performed by fine-needle aspiration (FNA) or core needle biopsy (CNB). Both procedures are routinely performed using ultrasound guidance, and although these 2 techniques have been used interchangeably, there are important differences. Fine-needle aspiration biopsy is a technique in which a fine needle is inserted into the mass and cells are aspirated yielding a cytological specimen for diagnosis. Core needle biopsy uses a lower gauge needle yielding a larger specimen that retains its cellular architecture and is used for histopathologic diagnosis.
Fine-needle aspiration for the evaluation of thyroid nodules has become a widely used and accepted tool in the diagnosis of nodular thyroid disease. 1 -5 Few reported complications of thyroid FNA have been noted, most commonly relating to hematoma formation, mild to serious hemorrhage, needle tract seeding, vascular proliferation, and infarction of a thyroid nodule. 4 In a study of 10 974 patients who underwent FNA of the thyroid, only 4 patients showed temporary vocal fold immobility on flexible laryngoscopy. Patients experienced voice changes occurring 1 to 2 days after undergoing FNA with all symptoms spontaneously resolving within 6 months. It is noted that although this study quotes an incidence of temporary vocal fold paralysis following FNA to be 0.036%, it is hard to determine true incidence as asymptomatic patients were not screened. 6
The limitations with the use of FNA in the evaluation of thyroid disease do not stem from a poor safety profile but rather from an issue of diagnostic uncertainty. It has been reported that anywhere from 3% to 30% of aspirated samples produce indeterminate or nondiagnostic results. 1,7,8 It can be challenging to obtain an adequate sample size for evaluation using the FNA technique. Collecting an adequate sample size is of the upmost importance as the cytologic specimen is most useful in conditions that rely on nuclear characteristics for accurate diagnosis. 9
It is with these limitations that ultrasound-guided CNB was proposed for the use in the diagnosis of nodular thyroid disease. Although historically not as commonly used as FNA for the evaluation of nodular thyroid disease, CNB has been advocated for routine use as the larger specimen size and retained cellular architecture have shown to provide a higher diagnostic accuracy. 7,9 Further support for its use is that results have shown the use of CNB decreased the need for further surgical intervention in patients with nondiagnostic FNA results. 9 Recent literature has been shown successful adaptation and proven the value of the CNB with diagnostic accuracy of 97% as compared to that of FNA which is around 78%. 10 With the addition of ultrasound guidance to the use of CNB, the safety profile becomes very similar to that of FNA, with Ha et al reporting that in 6169 patients undergoing ultrasound-guided CNB of thyroid lesions, only 50 (0.81%) having either a minor or major complications and of the 50 (0.06%) patients only 5 had major complications, including hematoma, pseudoaneurysm, and voice change. 7,11 Similar study by Ha et al noted only 4 patients who experienced voice changes usually concurrent with hematoma; 1 patient experienced a substantial voice change, which lasted 3 months, and the transient voice changes of the other 3 patients resolved spontaneously within a month. 11
We will discuss the first case of biopsy-proven nerve injury and immediate permanent vocal fold paralysis following CNB of the thyroid. In addition, we will discuss the current literature regarding the role of CNB in the evaluation of thyroid nodular disease. Finally, discussion of vocal fold paralysis after CNB should be considered in the informed consent process.
Case Report
A 38-year-old male was presented to our outpatient laryngology clinic for evaluation of acute-onset aphonia during ultrasound-guided core biopsy of the thyroid gland. Two weeks prior to our evaluation, the patient was seen by his otolaryngologist for intermittent otalgia. During the course of a complete history and physical examination, an incidental right thyroid fullness was identified. Of note, flexible laryngoscopy at that time showed no vocal fold motion abnormalities. An ultrasound and FNA thyroid biopsy were recommended for thyroid evaluation.
Thyroid ultrasound showed a solid right inferior pole lesion, measuring 1.32 × 1.0 × 1.61 cm, located in a lateral and posterior location within the lobe. As per the protocol of the hospital and the interventional radiologist, an ultrasound-guided core biopsy was performed, rather than an FNA, with the intent to improve diagnostic success. After achieving local anesthesia, an 18-gauge needle was inserted with ultrasound guidance to biopsy the nodule, performing several passes while under suction.
The patient reported sudden onset extreme pain over his right neck and was immediately aphonic. The aphonia was discussed with the patient and was thought to be due to inflammation or hematoma, with expected complete spontaneous resolution. He was discharged home, aphonic. His aphonia continued for the next 48 hours. The patient returned to his otolaryngologist and flexible laryngoscopy at this time showed immobility of the right true vocal fold. He was referred to our center for further treatment.
Flexible laryngoscopy with stroboscopy confirmed right true vocal fold immobility in the lateralized position and a large glottal gap (Figures 1 and 2). There were no hematomas, masses, or lesions. Review of the biopsy specimen was requested and showed, in addition to normal thyroid tissue, nerve bundle tissue seen within a fibroadipose background (Figure 3). The fibroadipose tissue seen is likely from around Berry’s ligament. A laryngeal electromyography was performed 4 months after injury, showing right recurrent laryngeal mononeuropathy characterized by the absence of voluntary motor unit recruitment. His vocal fold paralysis was treated appropriately, with excellent voice results. One year after injury, his vocal fold remained paralyzed.

Full abduction of vocal folds on flexible laryngoscopy. Right vocal fold immobility.
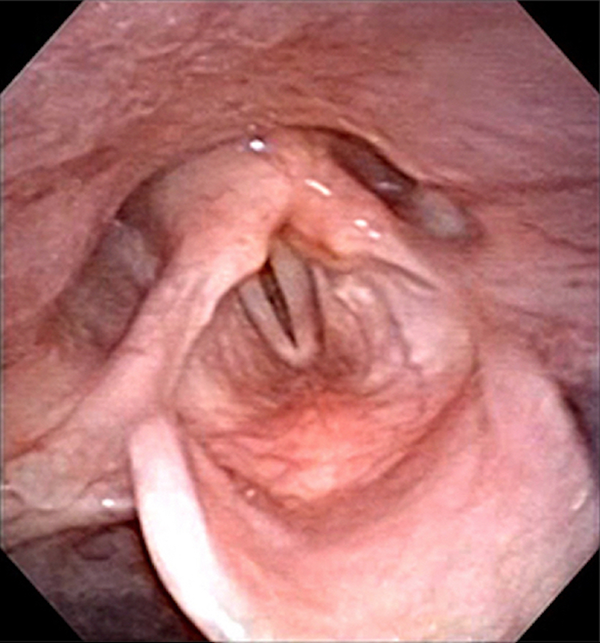
Full adduction of vocal folds on flexible laryngoscopy. Right vocal fold immobility with glottal gap.
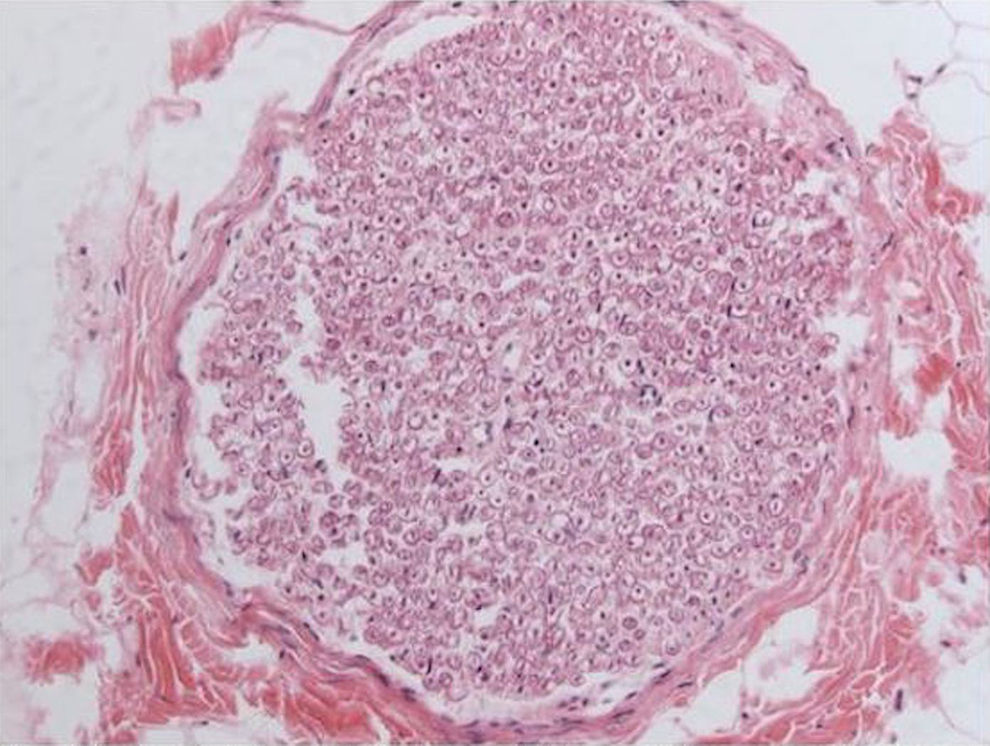
Specimen from ultrasound-guided core needle biopsy containing nerve bundle tissue seen within fibroadipose background (×410).
Discussion
This article reports, to our knowledge, the first case of biopsy-proven laryngeal nerve injury and permanent true vocal fold paralysis following an ultrasound-guided CNB of the thyroid. In light of this complication, it becomes even more important for the clinician to understand the role of CNB in the evaluation of nodular thyroid disease. In addition, this report highlights the need for the otolaryngologist to caution the patient of the possibility of vocal fold paralysis and recurrent laryngeal nerve injury during this procedure.
As noted earlier, FNA for evaluation of thyroid nodular disease has been widely used and accepted. 1 -5 However, in an effort to combat the relatively high rate of inadequate and nondiagnostic sampling with FNA, CNB has been proposed as an alternative to this procedure. 1 Core needle biopsy, as opposed to the “small needle” cytologic specimen retrieved in FNA, uses a larger, hollow needle to retrieve a “core” of tissue during biopsy.
Two major advantages in the use of core needle thyroid biopsy are (1) an ability to obtain increased tissue sample size and (2) the ability of this larger specimen to retain cellular structure. 7 In a retrospective analysis of 645 thyroid samples (with and without ultrasound guidance), Harvey et al noted that adequate samples were obtained in 87% of core biopsies compared to 60% of cytology aspirates.Additionally, they noted both core and fine-needle biopsies under ultrasound guidance had zero false-negative rates for malignancy, with 11% of patients requiring surgical confirmation of diagnosis following CNB versus 43% for patients following FNA. With these results, in addition to no significant complications during the study, they concluded that sonographically guided core biopsy provided an accurate and safe alternative to FNA in assessment of thyroid nodules. 9
Other studies have also compared the results of thyroid FNA and CNB showing similar results, 3,7,8,11 but some have even advocated CNB to be a better method for evaluation of the thyroid nodule than FNA. 1,8 A recent report from Sung et al retrospectively evaluated the results of FNA and CNB from 555 thyroid nodules where patients underwent both procedures for evaluation of each nodule. They show the sensitivity and accuracy of CNB or CNB with FNA to be significantly higher than that of FNA, with CNB being more accurate for the diagnosis of malignancy and the combination of CNB with FNA to be superior to all in the diagnosis of small nodules less than 1 cm. 1
In contrast, there are reports that have concluded that CNB or CNB/FNA was not superior to ultrasound-guided FNA, barring a few selected patients. 5 Other studies show that CNB alone was less sensitive for papillary carcinoma 2 and that combination of CNB/FNA should be considered as an alternative to surgery when patients have 2 prior nondiagnostic FNAs. 10 It is important to remember that as in FNA, CNB will not generally identify malignancy in a follicular lesion as capsular or vascular invasion cannot routinely be noted.
Complications of ultrasound-guided biopsy, either FNA or CNB, have been reported with similar rate including vocal fold paralysis (however, without image guidance, such as ultrasound), hematoma formation, mild to serious hemorrhage, needle tract seeding, and vascular proliferation. To our knowledge, this case reports the first permanent biopsy-proven recurrent laryngeal nerve injury following ultrasound-guided needle biopsy. At this point, there is no clear consensus to guide clinicians in the use of CNB for evaluation of thyroid nodular disease. Although the safety profile appears to be similar to FNA of the thyroid, the clinician must use all available information regarding CNB for evaluation of thyroid disease to determine its appropriate role in patient care.
Conclusion
Permanent vocal fold paralysis should be discussed during the consent process for ultrasound-guided core biopsy of the thyroid as a rare complication. With this in mind, the benefits of core biopsy need to be critically examined in light of possible risks. Care is to always be taken during these procedures and postprocedural dysphonia or aphonia need to be expectantly evaluated by laryngoscopy in order to institute appropriate treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.