
Abstract
Objectives:
We aimed to comprehensively investigate different upper airway segments in adults, determine the predictors of the size of each segment, and identify an appropriate endotracheal tube (ETT) size chart.
Study Design:
Retrospective chart review.
Setting:
Tertiary care center.
Materials and Methods:
The data for patients aged >18 years who underwent neck computed tomography were screened. Patients with existing tumors, trauma, or any pathology that can alter the normal airway anatomy and those with intubation, tracheostomy, or nasogastric tubes were excluded. Computed tomography software was used to measure the anteroposterior diameter (APD), transverse diameter (TD), and cross-sectional area (CSA) at the glottic, proximal subglottic, distal subglottic, and tracheal levels. Multiple regression analysis was used to identify the predictors of the airway size.
Results:
One hundred patients were reviewed. The TD was consistently smaller than or equal to the APD at each level in all but 3 patients. The mean CSA and TD (170 mm2 and 11.3 mm, respectively) of the glottis indicated that the glottis was most often the narrowest level, followed by the proximal subglottis where the mean CSA and TD were 192.1 mm2 and 12.7 mm, respectively. Moreover, the mean APD was the smallest at the level of the trachea (20.1 mm). Multiple regression analysis confirmed that height and sex were the predominant predictors of measurements for the 4 airway segments. In addition, age was associated with the TD and CSA of the distal subglottic and tracheal segments, respectively.
Conclusion:
One-third of our participants exhibited a proximal subglottic diameter that was equal to or smaller than the glottic diameter. Our findings also suggested that the height and sex of the patients are important variables for the selection of an appropriate ETT size.
Introduction
The determination of the narrowest segment of the upper airway in adults has been debated for years. The conventional literature states that the glottis is the narrowest part of the adult airway and that the cricoid is the narrowest part of the pediatric airway. 1 -5 However, this notion is controversial because several in vivo and in vitro studies have reported variable findings in adults. 1 -8 The different segments of the airway have been examined regarding size, factors predisposing to diameter changes, and factors leading to postintubation complications. 6,7,9 -12 Despite the extensive research on the airway anatomy, no strong conclusions emerge regarding the narrowest segment of the adult airway.
Studies involving autopsy and pathological specimens have been conducted with emphasis on the limited areas of the upper airway. 6,13 -16 A significant limitation of this study design is the inaccuracy of the findings because postmortem soft tissue changes can hinder the accurate measurement of each airway segment. 17 Furthermore, most cadaveric studies have involved elderly patients and rarely included a normally distributed adult population. Observations made in the elderly population cannot be generalized because some studies have confirmed that the airway size changes with age. 14,18
Conversely, in vivo studies have primarily used computed tomography (CT) for evaluations. However, most of these studies have either evaluated a single point in the upper airway 7,19 -23 or failed to describe at least one significant segment or dimension. 24 -26
The importance of identifying the narrowest segment of the upper airway in adults stems from its role in proper endotracheal tube (ETT) size selection, laryngotracheal surgery planning, and general airway management. The determination of factors that can alter the airway diameters is crucial for successful airway management.
The debate surrounding appropriate ETT sizing is still ongoing. No agreement has been reached regarding the proper ETT size for adults. An oversized ETT poses a significant risk for various complications ranging from self-limiting injuries to life-threatening conditions. Glottic and subglottic stenoses, vocal cord immobility, and arytenoid dislocation are well-known complications which eventually may need complex airway surgeries or temporary or even permanent tracheostomy tube. 10 -12,27 By contrast, undersized ETTs may compromise ventilation and hinder pulmonary hygiene or fiberoptic bronchoscopy, particularly in intensive care settings. 28,29
The present study aims to measure the dimensions of multiple upper airway segments in adults to determine the narrowest segment in this population. In addition, the predictors of the size of each segment were determined, and an appropriate ETT size chart was prepared.
Materials and Methods
This retrospective cohort study was approved by the institutional review board of King Saud University Medical City, and the informed consent was waived because of the retrospective study design. The study involved a medical chart review and CT scan analysis of all patients aged >18 years who underwent neck CT at our center between September 2014 and September 2018. Another inclusion criterion was the clear visibility of the glottis, subglottis (including the cricoid cartilage), and the first tracheal ring on the CT images. Patients with tumors and/or trauma or any pathology that can alter the normal airway anatomy; those with intubation, tracheostomy, or nasogastric tubes; and those with thick CT slices (>3 mm thickness) were excluded. The exclusion occurred after a careful review of the chart and the CT scan of interest.
A Philips 256-slice Brilliance iCT scanner (Philips Healthcare, Cleveland, Ohio) was used for all screened patients. As a routine protocol, a contrast-enhanced CT neck was done with the patient supine and breathing quietly. The axial scanning was performed from the skull base to the aortic arch with the acquisition plane parallel to the fourth and fifth or fifth and sixth cervical intervertebral disc spaces to obtain scans parallel to the vocal cords. The raw axial image data set was reconstructed with a section thickness of 1, 2, or 3 mm. All the images were reviewed in soft tissue windows. Using the inbuilt software, the anteroposterior diameter (APD), transverse diameter (TD), and cross-sectional area (CSA) for the glottis, proximal subglottis (6 mm below the vocal cords), distal subglottis (lower margin of the cricoid), and trachea (first tracheal ring) were measured. Kumar and Ravikumar concluded that the level 5 mm below the vocal cords presented the smallest coronal and sagittal diameters. 26 On the basis of this finding, we selected the proximal subglottis (6 mm below the vocal cords) in the present study. A cutoff distance of 6 mm from the vocal cords was chosen because our CT scan slices include 2- and 3-mm thickness; therefore, the 5 mm could not be attained in all patients. The subcricoid level was reported as an area of constriction in the upper airway. 7 To elaborate this finding, we selected the distal subglottis (lower margin of the cricoid) as the second level. Tracheal measurements have also been investigated; D’Anza et al selected the first tracheal ring, 21 while Kumar and Ravikumar selected a level of 2 cm below the cricoid cartilage. 22 Hence, we selected the first tracheal ring as the third level of measurement. Finally, the glottic level was not measured in any of the previous studies and was accordingly selected as the fourth segment in our study.
The airway column was outlined in the software to form a perimeter, where CSA was automatically calculated, and straight lines were drawn for the calculation of the diameters (Figure 1). The patient data, including age, sex, height, weight, and body mass index (BMI), were obtained from their charts on the day of CT scanning. After the statistical analysis, we proposed a cutoff value for the outer diameter (OD) of ETT to be 2 gender-specific standard deviations below the predicted diameter of the selected airway segment. On the basis of this equation, we proposed an ETT size chart by using the Smiths Medical Portex Cuffed Endotracheal Tube 30 as a model.
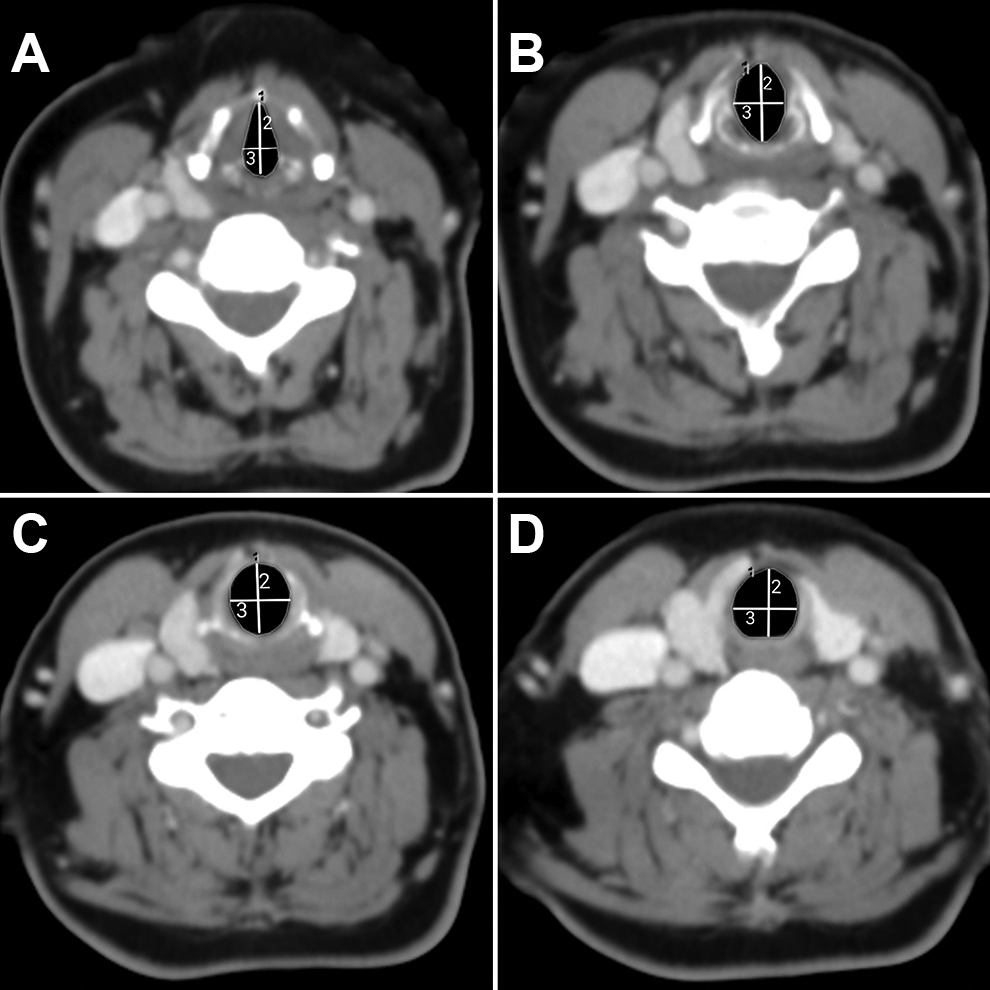
Computed tomography images for measurements of different upper airway levels in adults. A, Glottis. B, Proximal subglottis. C, Distal subglottis. D, First tracheal ring. (1) Cross-sectional area outline, (2) anteroposterior diameter, and (3) transverse diameter.
Statistical Methods
All the statistical analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC, USA). The means and standard deviations were obtained for continuous variables, and the frequencies and percentages were computed for categorical variables. Correlations among independent variables were assessed using the Pearson linear correlation or Spearman rank correlation coefficients, as appropriate. Moreover, correlation indicates the dependency among independent variables; therefore, it is the first step in addressing collinearity in multivariate regression. We also explored the variance inflation factor, and it suggested the exclusion of either weight or BMI. The robust multivariate regression analyses were performed to determine the association between the patient characteristics and the measurements for the glottis, proximal subglottis, distal subglottis, and trachea. A robust regression is a form of iteratively weighted and reweighted least squares regression used to derive stable results in the event of influential data or outliers. Twelve separate robust multivariate regression analyses were performed for each of the 3 measures (APD, TD, and CSA) obtained for the 4 segments. The maximum likelihood estimation (M-estimator) based on Huber weights was used to obtain robust regression estimates and standard errors (SEs). 31,32 In the case of the detection of influential data with bad leverage in any regressions, the MM estimation was used to compute robust regression estimates and SEs. 33 The initial regression diagnostics indicated a fair number of outliers including influential data in our sample, thereby supporting the use of robust regression analysis on the basis of the M-estimation method. We detected highly influential bad leverage points for analyses involving the CSA of the proximal and distal subglottis and the APD of the distal subglottis; therefore, the MM estimation was used to determine the associations between patient characteristics and these measures in multivariate robust regression analyses. A P value of .05 was considered statistically significant.
Results
From the 1163 screened patients, 100 were included and further analyzed. The majority of the cases were excluded due to the presence of head and neck tumors, laryngocele, pneumothorax, pneumomediastinum, or atelectasis; patients who had nasogastric tubes or were intubated or tracheostomized; and known history of upper airway pathology or stenosis. Table 1 shows the descriptive statistics for the patient characteristics. We did not stratify our analysis based on gender. We also reported descriptive statistics for all the participants separately by gender to provide scientific knowledge that may be relevant to future studies and understand the natural anatomical differences between men and women.
Descriptive Data for Adult Patients Selected for Multilevel Upper Airway Measurements.
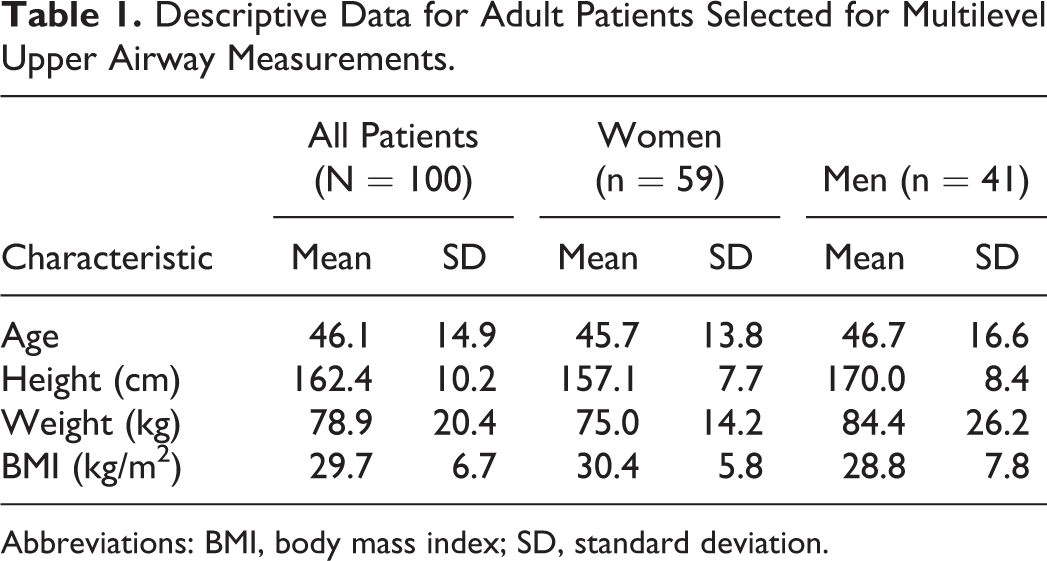
Abbreviations: BMI, body mass index; SD, standard deviation.
The narrowest CSA was most common at the level of the glottis (85%) followed by the proximal subglottis (15%). The narrowest TD was at the level of the glottis (67%), while the TD of the proximal subglottis was the narrowest in 13% of the patients. The TD was the same at the glottis and proximal subglottis in 20% of the patients.
Table 2 lists the descriptive statistics for all the measurements. The mean APD and TD of the glottis were 22.8 (±3.7) and 11.3 (±1.8) mm, respectively. The airway was narrowest at the level of the glottis, with a mean CSA of 170 (±48.6) mm 2 . The mean TD was the least at the level of the glottis in men and women.
Descriptive Statistics for Various Upper Airway Measurements in Adults.
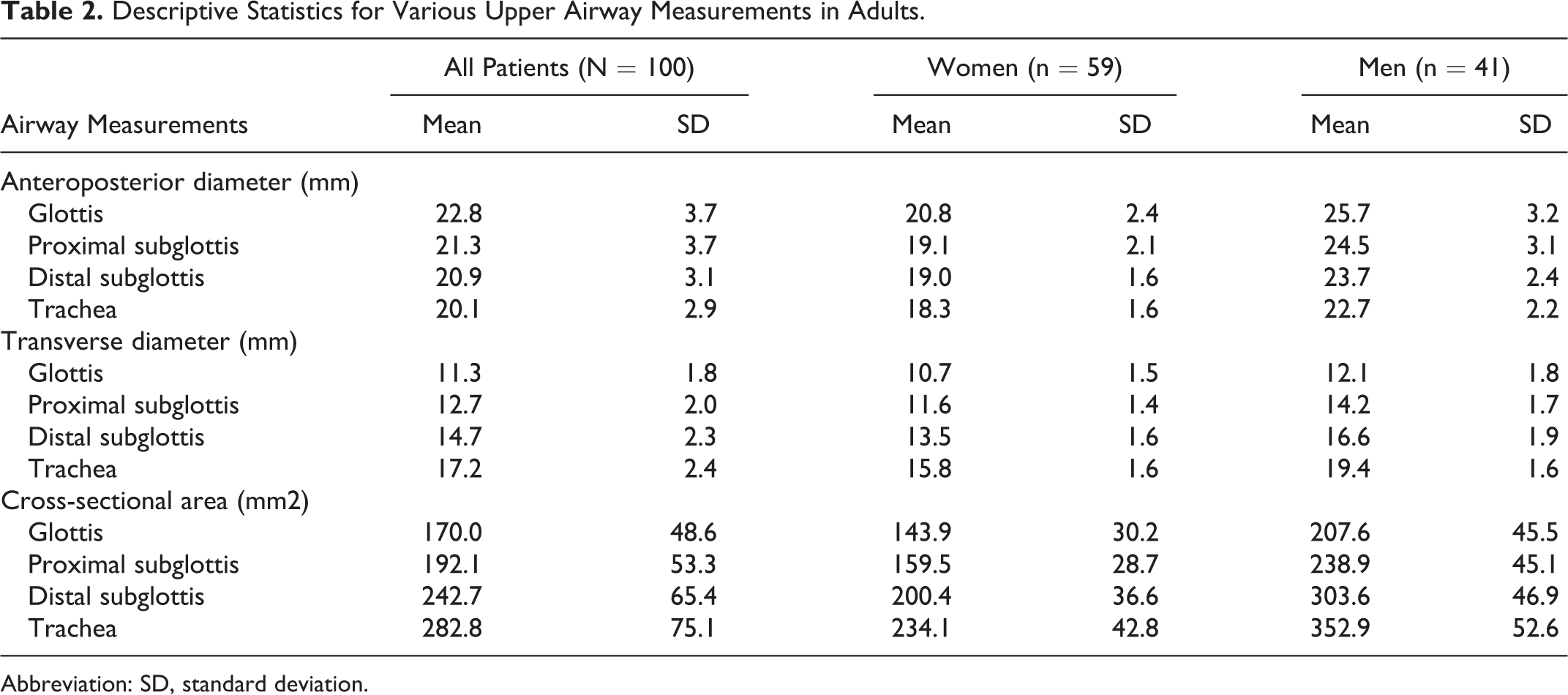
Abbreviation: SD, standard deviation.
Table 3 provides the robust parameter estimates, SEs, and P values for the linear associations between each patient characteristic and airway measurement. Because of a strong correlation (Spearman ρ = 0.85, P < .0001) between weight and BMI, weight was not considered in the multivariate regression models, leaving age, height, and sex as independent variables. We found that the sex and height of the patients were significantly associated with all the airway measurements (P < .05), except for the TD of the glottis, which was significantly associated only with height (P = .0084). In addition, the age of the patients was a significant positive predictor of the TD of the distal subglottis (P = .0202) and the CSA of the trachea (P = .0134). Body mass index had a significant negative influence on the TD of the trachea (P = .0146). The associations between the height and sex of the patients and the APDs of all the segments were highly significant (P ≤ .0001).
Multivariate Robust Regression Estimates and Standard Errors for the Association Between Patient Characteristics and Various Upper Airway Measurements in Adults.
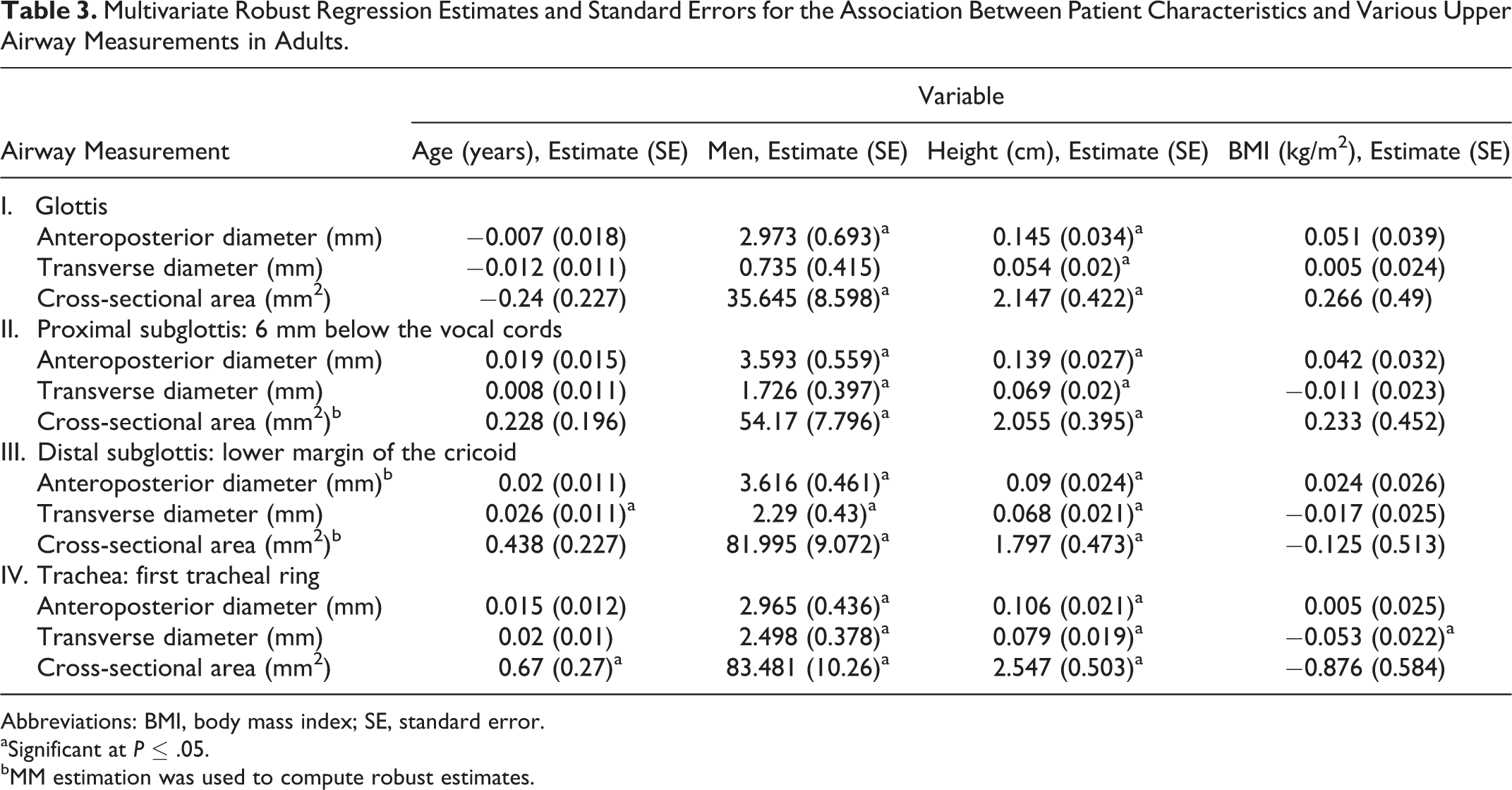
Abbreviations: BMI, body mass index; SE, standard error.
aSignificant at P ≤ .05.
bMM estimation was used to compute robust estimates.
Table 4 presents the final equations for predicting the measurements of the different segments. Incidentally, a 1-cm increase in height predicted 0.08 mm and 2.28 mm2 increases in the TD and CSA of the glottis, respectively. In addition, the CSA of the glottis was larger in men than in women by 33.35 mm2.
Final Equations for the Prediction of Upper Airway Measurements in Adults.
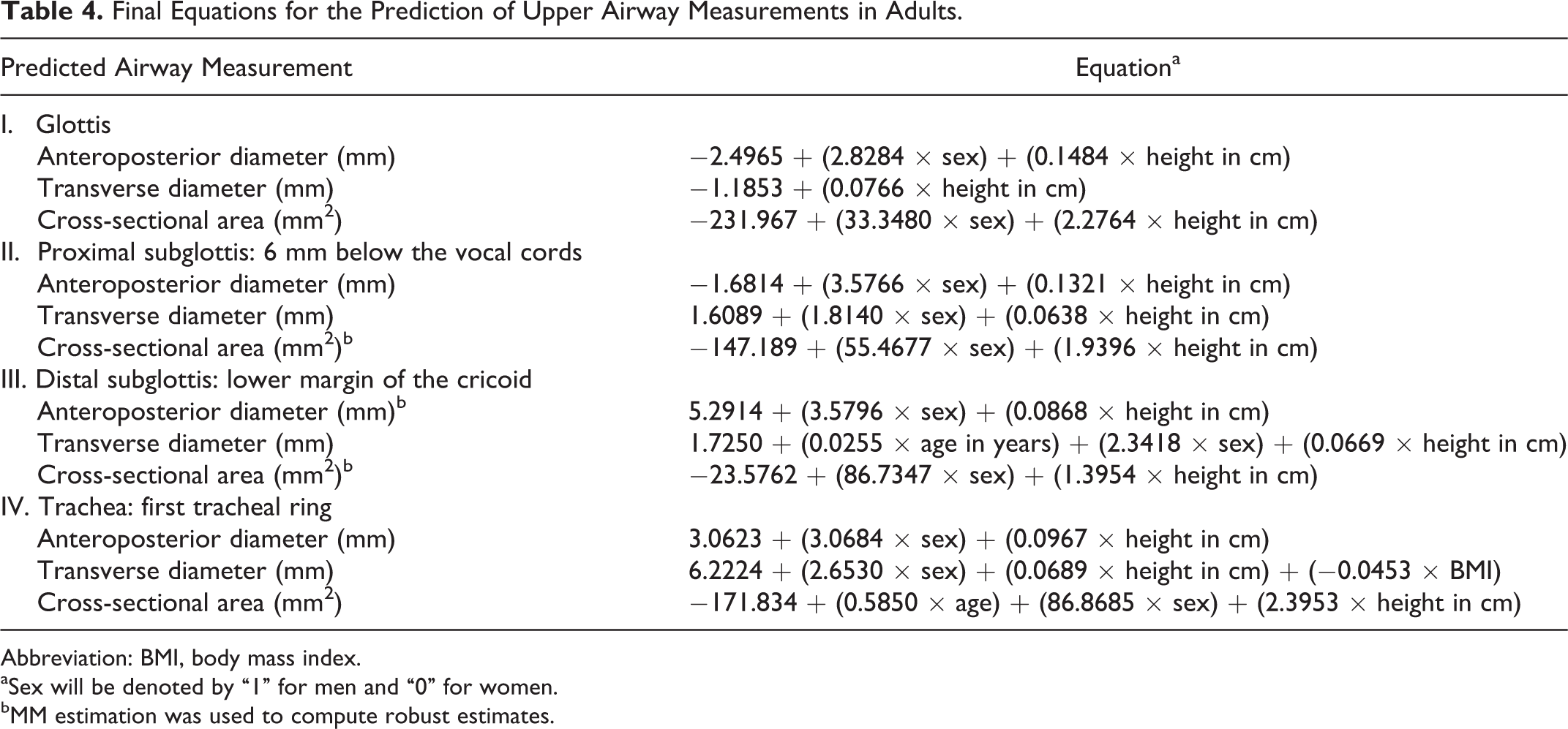
Abbreviation: BMI, body mass index.
aSex will be denoted by “1” for men and “0” for women.
bMM estimation was used to compute robust estimates.
The measurements for the proximal subglottis could be predicted by the sex and height of the patients. A 1-cm increase in height predicted a 0.06 mm increase in TD, and the predicted TD was larger in men than in women by 1.81 mm. Notably, BMI was negatively correlated with the tracheal TD, with an increase of 1 kg/m2 predicting a decrease of 0.05 mm. Utilizing our final equations, we proposed an ETT size chart based on the TD of the proximal subglottis according to the sex and height of the patients utilizing the Smiths Medical Portex Cuffed Endotracheal Tube 30 (Table 5).
ETT Size According to Sex and Height, Derived From Upper Airway Measurements for Adults.
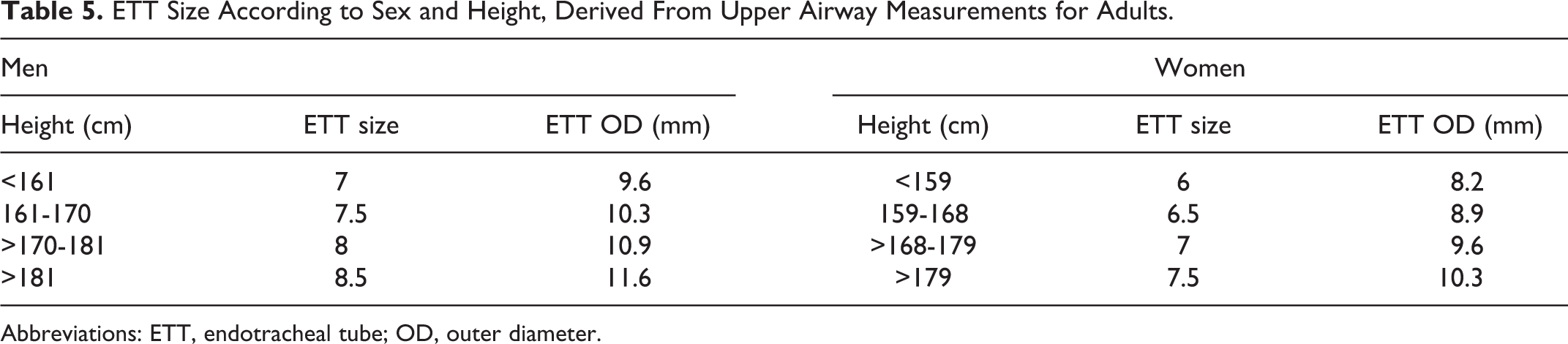
Abbreviations: ETT, endotracheal tube; OD, outer diameter.
Discussion
The present study performed comprehensive upper airway measurements in adults using CT images. Compared with pathologic studies, autopsies, magnetic resonance imaging, and radiography, CT imaging is currently considered the best modality for the evaluation and measurement of the upper airway dimensions. 24,34 -36 The different levels of upper airway constrictions measured using CT images have been reported in the literature. 7,21,22,26 This variability in reporting motivated us to select 4 specific segments for the measurement of narrowing in the present study.
Airway measurements at the level of the glottis on CT images are associated with 2 difficulties. First, the glottis is highly dynamic in nature, and the vocal cords may appear completely adducted during the examination. Besides, the irregular shape of the glottis may hinder the acquisition of appropriate measurements, particularly for CSA, using routine mathematical calculations. At our center, the neck CT protocol warrants the acquisition of images during the quiet breathing phase, which allows for vocal cord abduction. Advancements in technology and the availability of sophisticated inbuilt software facilitate accurate diameter and CSA calculations, even for irregular shapes.
In our analysis, TD was consistently smaller than APD at each level in all but 6 patients, 3 of whom exhibited equal TDs and APDs and 3 of whom exhibited a smaller APD at the tracheal level. Notably, the mean APD steadily decreased, whereas the mean TD and CSA increased from the glottis to the trachea. On the basis of these findings, we strongly suggest that the narrowest upper airway segment may be found at the level of the glottis or the proximal subglottis, not at the level of the distal subglottis and trachea as shown in previous studies. 7,21,22 The sex and height of the patients represented the most important predictors of the airway size. These findings are in agreement with those of Coordes et al and D’Anza et al, who reported that height had a consistent significant association with the airway size, while Karmakar et al confirmed that only height in males was significantly associated with the airway size. 7,21,22 Women were found to have a smaller airway size 21,22 ; however, one study has denied any association between sex and the airway size. 7 Age was not shown to be significant in previous studies as opposed to our findings which were significantly associated with TD of the distal subglottis and CSA of the trachea. Interestingly, BMI showed a negative association with the TD of the trachea in our study, with an increase of 1 kg/m2 predicting a decrease of 0.05 mm. This supports the finding of D’Anza et al. 21 Accordingly, we recommend against the use of a larger ETT for obese patients.
The risk of the oversized ETT may include minor complications, such as nonobstructive edema, granulation tissue formation, simple ulcerations, and sore throat, while serious complications include excessive granulation tissue formation, obstructing edema, posterior glottic or subglottic stenosis, arytenoid dislocation, and vocal cord immobility. 10 -12,27 An editorial published in 2012 recommended an ETT size 9.0 for men and 8.0 for women. 29 The application of this recommendation to our sample would inevitably result in laryngotracheal trauma in 20% of our patients who exhibited a proximal subglottic TD that was smaller than the OD of the ETT suggested.
The airway diameter is suggested to be the basis for ETT size selection. 28 The OD of ETT should be smaller than the smallest airway diameter; however, the precise difference between the 2 diameters remains unclear. While some studies have proposed a fixed difference of 2 to 6 mm, others have selected the lower limit of the confidence interval of the airway diameter to predict the OD of the ETT. 6,7,22 To protect patients from postintubation trauma and ensure adequate ETT function for ventilation and airway management procedures, such as flexible bronchoscopy, we recommended a cutoff value for the OD of ETT to be 2 gender-specific standard deviations below the predicted TD of the proximal subglottis. If a normal distribution is assumed, then using 2 standard deviations may statistically minimize the risk of postintubation injuries to 2.5% of patients who lie in the positive direction of the curve compared with 16% possible risk if 1 standard deviation is employed. The size chart (Table 5) may provide practical guidance regarding ETT selection to health-care practitioners.
In our study, TD was the smallest airway dimension, while the smallest segments were the glottis and/or proximal subglottis. Therefore, the TD of the glottis or proximal subglottis should be the reference for appropriate ETT size selection. Several convincing reasons may justify the use of the proximal subglottis instead of the glottis as the reference for ETT selection. First, the proximal subglottis was equal to or smaller than the glottis in at least one-third of our study participants. This percentage may even be higher if a prospective study design with proper control of breathing pattern is employed to ensure complete vocal cord abduction. Second, the subglottic area includes the cricoid cartilage, which is the only complete, fixed, and nondistensible ring when compared with the highly dynamic vocal cords. Third, as shown in histopathological studies, the cricoid area, followed by the vocal process of the arytenoid cartilages, is at the highest risk of injury secondary to endotracheal intubation. 37,38 Fourth, if we use our equation for the prediction of the glottic TD and apply our method for appropriate ETT selection, then we would end up with an extremely small ETT (eg, size 5.5 for a patient with a height of 160 cm, regardless of his/her sex).
This study has limitations inherent to its retrospective design. First, the adherence to the quiet breathing protocol may not have been strong in such a design that may induce artefacts in some images. A prospective study with images obtained during deep breathing could assure full abduction and accurate results at the level of the glottis. This limitation may nevertheless have had little impact on the subglottic and tracheal measurements. Second, finding normal imaging for the patients was difficult, as they had undergone CT imaging for a suspected pathology. This limitation was overcome by the strict inclusion and exclusion criteria, which can be reflected by the large number of screened and excluded patients. In addition, the reader should exercise caution in interpreting the results owing to the issue of multiple comparisons. The results, however, would have been the same if the study has been restricted to one single factor. Therefore, our results are less likely to be influenced by this issue of multiple comparisons. 39,40
Conclusion
In conclusion, the findings of the present study suggest that the glottis and/or proximal subglottis represent the narrowest airway segments. The significant predictors of the TD are height and sex. The predictive models of the TD can be used to estimate the best ETT size which will need to be validated in future studies.
Footnotes
Authors’ Note
Presented orally at the ALA (American Laryngological Association) Meeting during the Combined Otolaryngology Spring Meeting in Austin, Texas, on May 1, 2019.
Acknowledgments
This study was supported by the College of Medicine Research Center, Deanship of Scientific Research, King Saud University, Riyadh, Kingdom of Saudi Arabia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.