
Abstract

Oncologic defects of head and neck often result in complex reconstructive problems. Achieving both aesthetic and functional restoration after tumor resection, 1-stage reconstruction is certainly the best option. However, seeking a reliable and suitable flap for 1-stage reconstruction remains a great challenge for plastic surgeons. 1 In 1963, Converse and Wood-Smith were the first to describe supratrochlear artery forehead island (STAFI) flap for 1-stage reconstruction of nasal dorsum defects. 2 Since then, STAFI flap has been widely utilized to repairing skin soft tissue defects caused by congenital malformation, trauma, and tumor resection. However, STAFI flap has certain drawbacks such as distorted eyebrows, limited reach, and requiring correction in a second stage. To address these issues, we modify a tunneled design for single-stage reconstruction of nasal defects. To distinguish the traditional STAFI flap, this modified supratrochlear artery forehead flap was named modified supratrochlear artery forehead island (MSTAFI) flap. Herein, we share our own clinical experience of using MSTAFI flap as an aid to repair a large nasal defect in a patient with squamous cell carcinoma.
A 49-year-old man was referred to our department for surgical treatment of a squamous cell carcinoma on the nasal dorsum. Physical examination revealed a 2 × 3 cm ill-defined brown patch on a background of photodamaged skin (Figure 1). Surgical excision was performed, with a final defect consisting of an oval, vertically oriented, full-thickness skin defect measuring 4 × 4 cm without involvement of the bilateral alar (Figure 2A). According to the preoperative design, an MSTAFI flap was successively performed. Final pathology studies disclosed squamous cell carcinoma of nasal dorsum. At 5-year follow-up visit after operation, the patient had achieved an excellent color match and a favorable aesthetic restoration without tumor recurrence (Figure 3).

Squamous cell carcinoma measuring 2 × 3 cm on the nasal dorsum in a 49-year-old man.
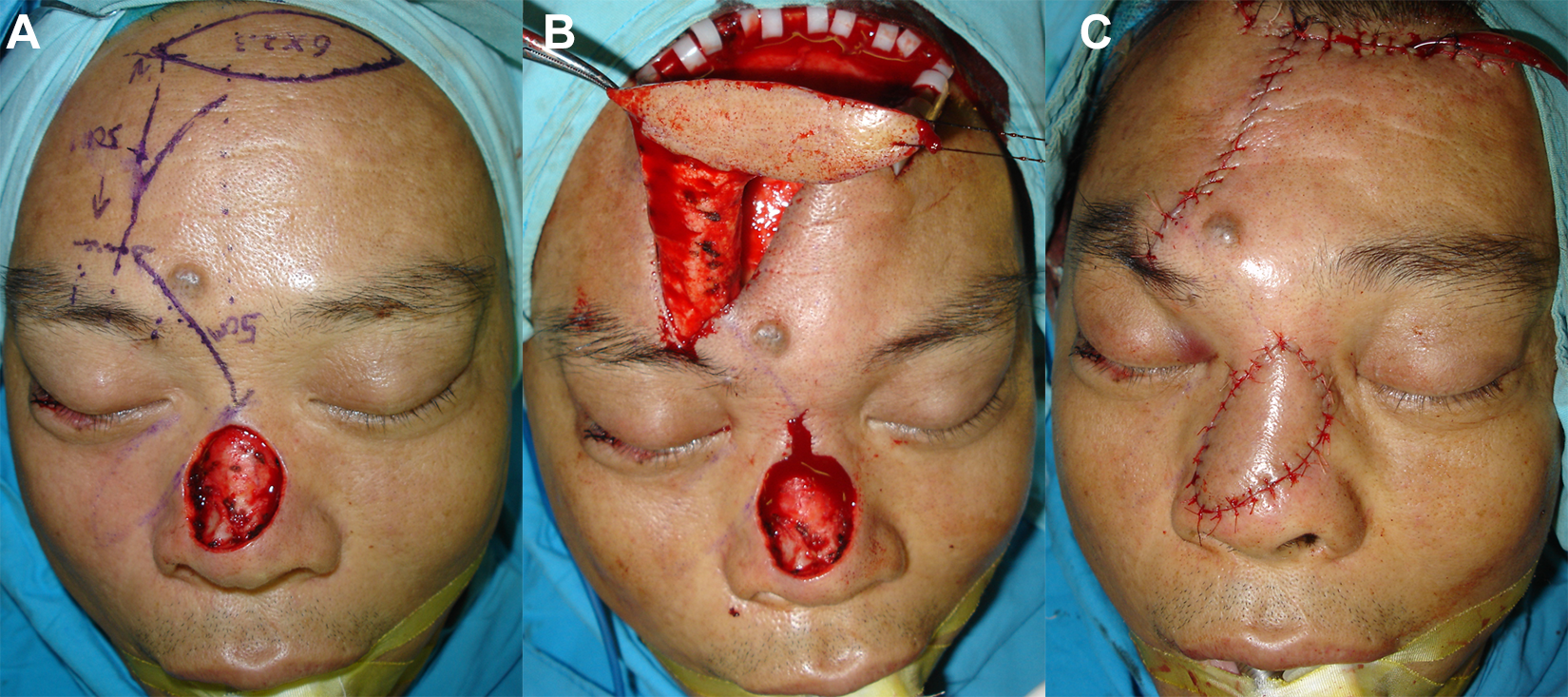
A, Immediate postoperative defect of the dorsal nose measuring 4 × 4 cm. B, Design and implementation of a modified supratrochlear artery forehead island (MSTAFI) flap. C, The defect closed with fine interrupted sutures.

The patient demonstrated an excellent color match and a favorable aesthetic restoration without tumor recurrence at 5 years after surgery.
The surgical technique consists of the following. Once the defect is outlined, the supratrochlear artery is identified by means of a Doppler probe and marked on the skin. Full thickness of skin is incised around the inverted pattern of the defect outlining the skin portion of the island flap. A transverse leaf-shaped island flap is excised superficially from the median forehead area. The skin of the forehead is then undermined downward over the glabella and inner canthus as far as the nasal defect (Figure 2B). The undermining of the skin is extended laterally toward the vascular pedicle in the supratrochlear region on the appropriate side. The island flap and subcutaneous pedicle are now mobilized and rotated 180° through the subcutaneous channel to the defect. The skin edges of the island flap are then sutured to the edges of the defect with fine interrupted sutures (Figure 2C).
This MSTAFI flap offers several advantages. First, the tunneled transverse island flap has advantage of greater mobility and longer turning radius; thus, it is more suitable to cover the further nasal area. Second, due to a median leaf-shaped design, distorted eyebrows were avoided. Third, the island flap is raised and immediately placed into the defect, the secondary defect is closed, and the operative procedure is completed at the one stage.
Our flap also has several limitations that require consideration. The principle disadvantage encountered with the island flap is the protrusion produced in the region of the root of the nose by the subcutaneous pedicle. This protrusion may require secondary excision, although we have noted a marked tendency to regression after about 3 months. Another disadvantage is the marked degree of venous congestion observed in the flap during the first 2 days after transplantation. The clinical changes undergone by the flap resemble in part those displayed by a composite graft.
In our report, MSTAFI flap enables reconstructing a large nasal oncologic defect, with an excellent color match and a favorable aesthetic restoration. This novel flap has shown to be feasible, reliable, and advantageous alternative to the reconstruction of nasal defects. However, due to the certain operating difficulty, the surgeon’s experience and familiarity with this modified flap is especially important.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.