
Abstract
Objective:
This study describes a surgical approach wherein a lobulated pedicled nasal mucosa flap technique was employed for endoscopic dacryocystorhinostomy (EDCR) as a means of treating nasolacrimal duct obstructions. This study also assessed the long-term outcomes of this EDCR approach when implemented without stenting.
Methods:
This was a retrospective study of a total of 63 patients (67 eyes) treated for nasolacrimal duct obstructions between January 2011 and November 2016. All patients had undergone ophthalmic diagnosis followed by EDCR treatment using a lobulated pedicled nasal mucosa flap without stenting. Patients were then monitored for both anatomical patency and sustained symptom relief during the follow-up period in order to assess objective and subjective study outcomes.
Results:
Patients were followed for a mean of 25.3 ± 1.2 months (range: 24-28 months), with a 100% anatomical patency success rate (67/67) and a 94.03% symptomatic cure rate (63/67). There were no instances of complications.
Conclusions:
The use of a lobulated pedicled nasal mucosa flap technique for EDCR without stenting is a straightforward, effective, and safe approach that keeps bone exposure to a minimum while offering a high rate of satisfactory outcomes, making it a procedure worthy of consideration as a means of treating patients suffering from nasolacrimal duct obstructions.
Introduction
Dacryocystorhinostomy (DCR) is a surgical approach commonly used for treating obstructions of the nasolacrimal duct (NLD), with the primary DCR strategies including external DCR, endoscopic DCR (EDCR), and laser-assisted EDCR. As sinonasal surgical techniques have become increasingly advanced, the utility of the endonasal EDCR approach has been increasingly explored, as this procedure offers advantages including a reduced need for any external incisions, an associated reduction in the risk of damage to the orbicularis oculi pump mechanism, and the potential for surgeons to simultaneously treat other concomitant intranasal pathologies. 1,2
Despite these advantages, EDCR does have certain challenges and drawbacks as a surgical approach, with the most prominent challenge associated with this procedure being the difficulty of accurately locating the lacrimal sac and avoiding neo-ostium restenosis. 3,4 Dacryocyst localization is typically achieved based on anatomical landmarks including the maxillary line and axils of the middle turbinate. However, such landmarks can vary markedly in appearance between individuals, and this can lead surgeons to conduct excessive mucosal incisions, to conduct osteotomy in the wrong location, or to remove the bone over the lacrimal sac. 5 These challenges are the leading causes of surgical failures for the EDCR approach. 6,7
Some surgeons routinely employ a stent after EDCR, 8 whereas others prefer to use a stent only for revision surgeries. There are differing viewpoints regarding the benefits and outcomes of stenting. Some surgeons have reported that stenting increases the success rate of this procedure; however, many studies have shown that there are no significant differences in outcomes as a result of stenting. 9,10
In the present report, we describe a lobulated pedicled nasal mucosal EDCR technique that allowed for temporary exposure of the maxillary bone above the lacrimal sac and NLD. Following operative completion, these flaps can be replaced, covering exposed bone and thus minimizing the risk of cicatricle stenosis. We further describe the long-term outcomes of patients treated via EDCR without stenting.
Materials and Methods
Patient Data
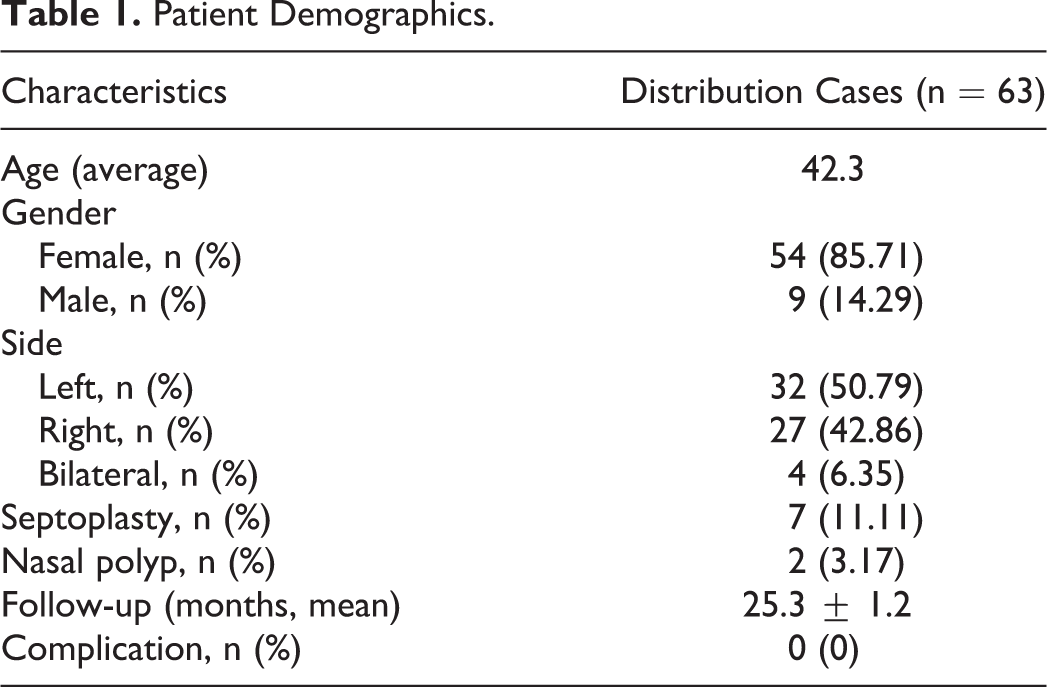
The institutional review board of the First Affiliated Hospital of Anhui Medical University, Hefei, China, approved this study, with all patients providing informed consent. In this retrospective analysis, medical information from 63 total patients (67 eyes) treated via EDCR between January 2011 and November 2016 was reviewed to assess clinical and long-term outcomes. Patient demographic information is compiled in Table 1.
Patient Demographics.
Preoperative Evaluation
Prior to surgery, an ophthalmologist conducted a comprehensive assessment of the extraocular area and nasolacrimal system of every patient, with lacrimal sac or NLD obstructions being evaluated via lacrimal irrigation and dacryocystography. Dacryocystography can allow for the direct visualization of lacrimal sac atrophy, occupying lesions, and/or foreign bodies in the lacrimal drainage system, and it also allows for accurate preoperative obstruction localization in patients with NLD obstructions. Patients then underwent preoperative counseling in an otolaryngology department, and their paranasal sinuses were analyzed via both endoscopy and computed tomography (CT). Nasal endoscopy provided information pertaining to any structural abnormalities of the nasal cavity and nasal landmarks, including the middle turbinate axilla, the uncinate process, and other anatomical indicators. Axial and coronal images from high-resolution CT imaging provided precise information regarding the anatomy of the NLD.
Patients underwent external and nasolacrimal system examinations, and those diagnosed with NLD obstructions were included in this study. Patients were excluded from this study if they had a history of lacrimal surgery, suspected malignancies, serious post-traumatic bone deformities, or previous facial fractures or nasal neoplasms. The same surgeon conducted all surgical operations in this study using either general or regional anesthesia.
Surgical Technique
A 0° rigid endoscope was used for the entirety of the surgical operation in this study. The nasal cavity was first packed using neurosurgical platelets that had been soaked in 4‰ adrenaline and/or tetracaine (4‰ adrenaline was used in patients undergoing general anesthesia; 4‰ adrenaline and tetracaine were used in patients undergoing regional anesthesia) in order to induce sufficient vasoconstriction and topical decongestion, after which a solution of 3% lidocaine and 1:200 000 adrenaline was injected submucosally over the rhinostomy site. Initially, septoplasty was conducted as needed. Next, the maxillary line, uncinated process, and axilla of the middle turbinate were identified as anatomical landmarks to guide the surgery. An initial semicircular incision roughly 20 mm in diameter was then made beginning 8 mm above the axilla of the middle turbinate and stopping at the level of the superior aspect of the inferior turbinate (Figures 1A and 2A). The mucosa and periosteum were then stripped away from the underlying bone using a freer periosteal elevator, yielding a pedicled nasal mucosa flap. This mucosa was protected using neurosurgical pledgets, producing space to facilitate bone removal. This approach exposed the maxillary bone above the lacrimal sac and NLD. Both this bone and the lacrimal bone segments which were over the lacrimal sac were then removed in their entirety using a Kerrison rongeur, beginning at the site of the lacrimal bone suture and the anterior section of the uncinate process (Figure 2B). Once the entirety of the lacrimal sac mucosa had been exposed, a lachrymal probe was passed into the lacrimal sac through the inferior or superior canaliculus, tenting the medial sac wall so as to confirm its surgical position. Next, an incision in the lacrimal sac mucosa was made, extending from the most superior position with a bias toward the anterior border, then straight down, ending at the level of the sac–duct junction, thus generating a large posterior lacrimal flap. Next, 2 horizontal relaxing incisions were created at either end of this flap to yield a “]”-shaped mucosal flap (Figure 2C). The pedicled nasal mucosa flap was then reset using the axilla of the middle turbinate as a landmark, cutting the flap into a superior and an inferior lobulated section based on the size of the dacryocyst flap and the exposed bone (Figures 1B and 2D). The superior flap was then used to cover the exposed anterior ostium bone, whereas the inferior flap was covered using the lacrimal mucosal flap (Figure 1C and E). This eliminated any exposed bone and avoided the risk of postoperative cicatricial stenosis of the neo-ostium. The flaps were then stabilized using an inferiorly directed freer elevator, an appropriate NasoPore was applied to the ostomy site, and the mucosal flaps were fixed. No stenting was conducted in any patients.
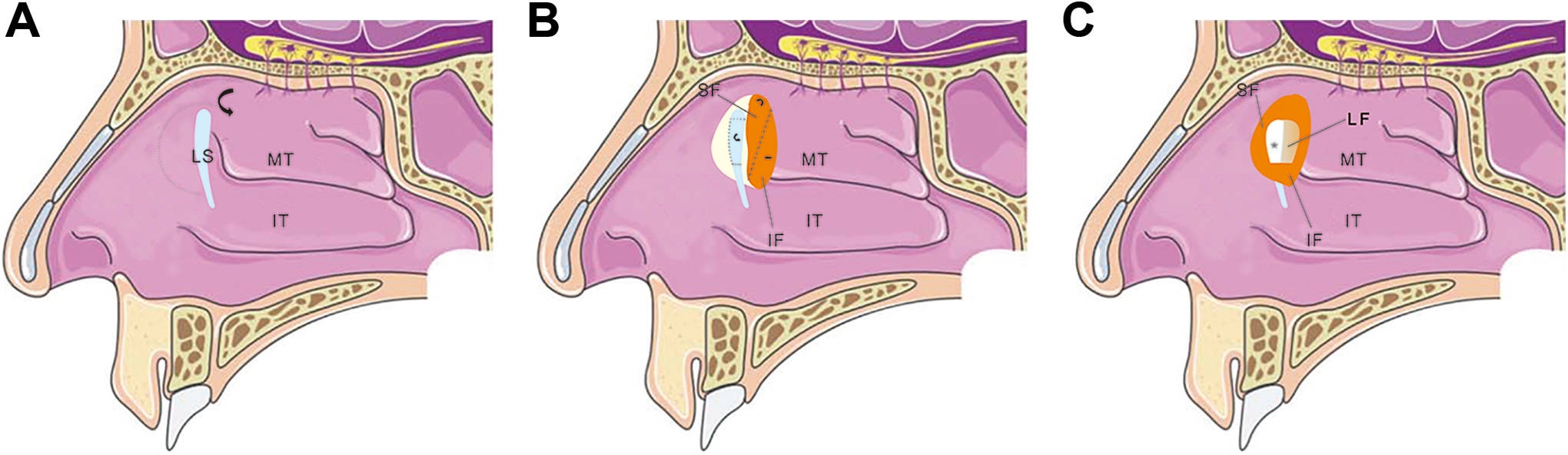
A, Incision of the lateral nasal wall. B, Incision sequence for the lobulated pedicled nasal mucosa flap and the lacrimal flap. C, Postoperative interlaced flap positioning.
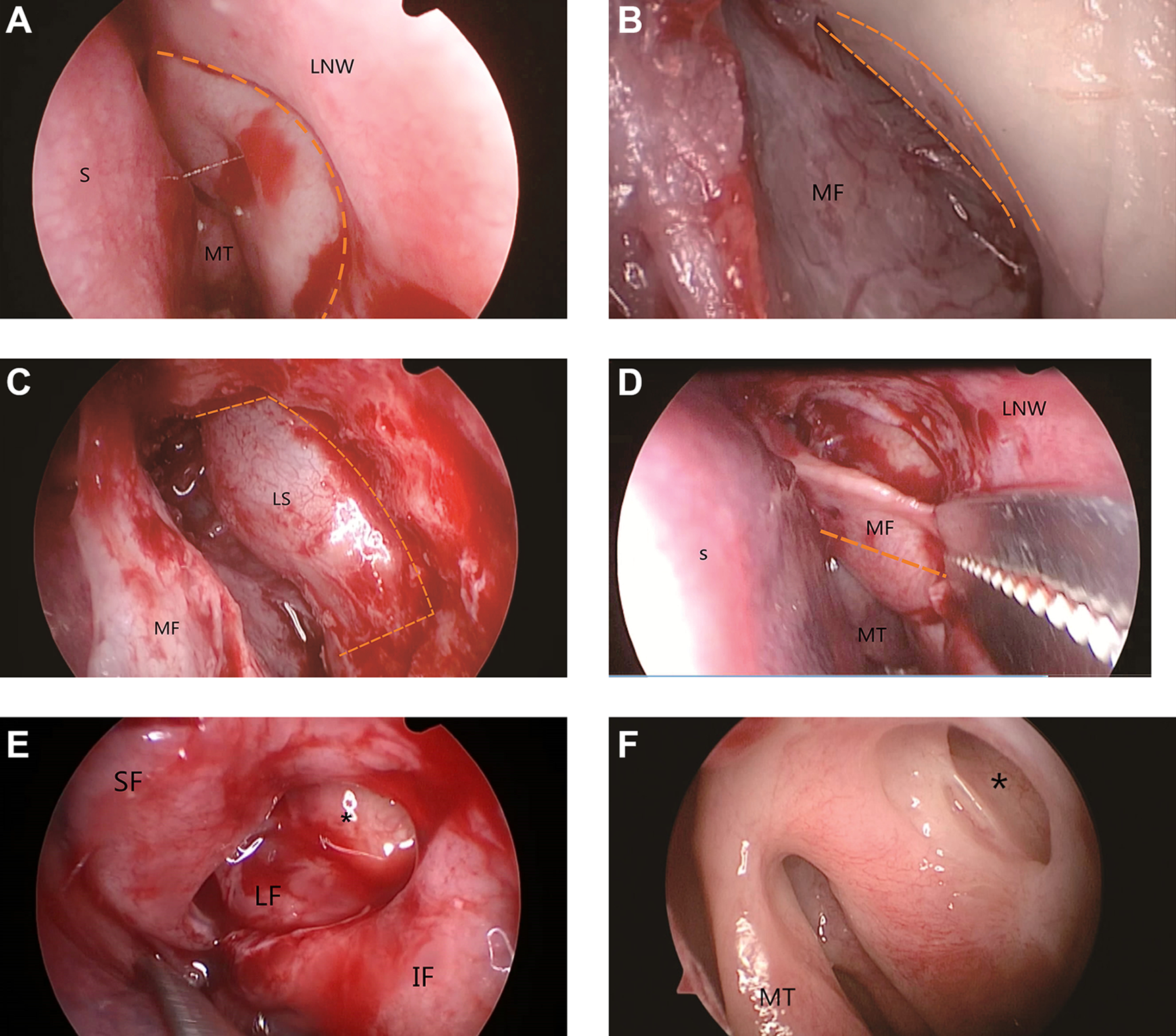
A, Incision of the lateral nasal wall. B, Suturing of the lacrimal bone with the anterior uncinate process and the maxillary bone. C, Lacrimal flap incision. D, Incision to generate the lobulated pedicled nasal mucosa flap. E, Final positioning of the interlaced mucosal flaps above and beneath the lacrimal sac. F, Successful lacrimal sac marsupialization. *Lacrimal sac marsupialization. IF indicates inferior flap; IT, inferior turbinate; LF, lacrimal flap; LNW, lateral nasal wall; LS, lacrimal sac; MF, mucosa flap; MT, middle turbinate; S, septum; SF, superior flap.
Postsurgical Care
Two weeks after completion of the surgical operation, the NasoPore was removed. For 4 weeks postoperatively, patients were treated using topical antibiotics and steroid drops together with a steroid-based nasal spray that was administered once daily along with normal saline in order to prevent the formation of crusts within the nasal passages.
Patients underwent follow-up assessments at 3, 6, 12, 18, and 24 months postoperatively. Follow-up consisted of an anatomical patency assessment and a symptomatic cure assessment. Anatomical patency was evaluated using objective methods, with anatomical patency success being defined as the presence of a patent lateral nasal wall bone window and the lack of any obstruction to the intranasal flow of saline or fluorescein during syringing via the lacrimal puncta under endoscopic evaluation. Symptomatic cures were evaluated using subjective methods and defined by the lack of epiphora, with no further episodes of dacryocystitis and the ability to irrigate the lacrimal system postoperatively.
Results
A total of 63 patients were treated via this approach, with 4 patients being treated in both eyes for 67 total surgeries. Patients were an average of 42.3 years old (range: 9-62 years), and the mean follow-up period was 25.3 ± 1.2 months. Patients were considered as unsuccessful cases if they still experienced epiphora during postoperative follow-up. Over the long-term follow-up period, patients had a 100% rate of anatomical patency (67/67) and a 94.03% symptomatic cure rate (63/67). Only 3 patients (4 eyes) still suffered from epiphora following EDCR, with 1 patient having undergone bilateral EDCR. In these 4 eyes, postoperative symptoms were significantly improved in 3 eyes and slightly improved in 1 eye, with no postoperative symptoms having been aggravated. In 3 of the 4 failed eyes, the epiphora symptoms disappeared upon bicanalicular silicone stent intubation. One eye still exhibited epiphora following this intubation, although symptoms had improved. No lacrimal sump syndrome occurred in any of our patients. No patients suffered from any complications during surgery. One patient exhibited granulation tissue formation at the surgical site within 1 month postoperatively, and this was removed endoscopically. No scars or any other complications developed in any patients during long-term follow-up.
Discussion
Endoscopic DCR is commonly used for treating NLD obstructions as it has a low risk of complications and offers advantages over other techniques. Recent advances in endoscopic surgery have led to increased EDCR success rates, even in individuals suffering from nasal diseases. 11,12 Indeed, among patients in the present report, 7 suffered from a deviated nasal septum and 2 from nasal polyps who underwent simultaneous surgical treatment. Many mucosal flap techniques have been used to improve the success rate of EDCR. At a mean follow-up of 21.8 months, Ali et al reported anatomic success rates of 97.7% and functional success rates of 95.5% in 90 primary powered EDCR procedures. 13 Coumou et al reported an anatomical success rate of 90.1% and a functional success rate of 91% for EDCR in 577 adult cases, with a mean patient follow-up of 5.7 months (range: 3-21 months). 14 One recent study of a modified mucosal flap technique reported an anatomical success rate of 100% and a functional success rate of 92.6%, 8 while another reported an anatomical success rate of 100% and a functional success rate of 96.4%. 4 In these studies, mucosal flaps were made with more than one incision and the follow-up was relatively short term. Trimarchi et al reported on 498 primary EDCR procedures with a mean follow-up duration of 38.07 months, an anatomical success rate of 91.54%, and a functional success rate of 90.4%. 15 In our primary EDCR cases, we observed anatomical success rates of 100% and functional success rates of 94.03% after a mean 25.3-month follow-up period, which is comparable to the long-term success rates reported for other EDCR techniques. In addition to its high success rate, EDCR is well tolerated by patients. Miyake et al evaluated the impact of EDCR on sinonasal quality of life and reported that nasal symptom scores returned to baseline levels within 30 to 90 days following EDCR surgery. 16
Although many novel surgical techniques have been applied to bolster EDCR success rates, a number of factors can influence these rates. One challenge that can hamper EDCR procedures is the accurate localization of the lacrimal sac. While locating the intraosseous region of the NLD may represent an ideal strategy given its fixed localization relative to the lacrimal sac, doing so requires the removal of substantial amounts of bone and mucosal tissue. 4 We therefore sought to develop an approach to safely and reliably identifying the location of the lacrimal sac. To do so, we created a semicircular mucosal flap roughly 20 mm in diameter in a single incision, with a distance of approximately one-third the diameter of the flap being above the axils of the middle turbinate. Given that the frontal process of the maxilla, the lacrimal bone, and the anterior section of the uncinate process are closely associated with one another and near to the lacrimal bone, we were able to reliably use the suture line with the lacrimal bone as a landmark for locating the lacrimal sac. This allowed us to effectively locate and expose the lacrimal sac and NLD without the need for extensive mucosal resection during osteotomy.
The creation of a large bony ostium is another factor that can ensure positive outcomes for DCR surgeries, but doing so using a laser-based approach for external DCR operations can be challenging, resulting in higher rates of failure. Multiple approaches can be used to expose the bone and lacrimal sac in its entirety, including the use of high-speed drills or Kerrison rongeurs, with the latter instruments chosen in the present study as drills have the potential to damage the mucosal flaps and to generate bone powder. Indeed, some reports have observed higher success rates when a Kerrison rongeur is used as compared with a high-speed drill, 17 justifying our approach to use the latter tool and/or an osteotome for bone removal in this study.
Marsupialization is an essential approach to ensuring successful EDCR outcomes, as cicatricial closure and restenosis are the most common causes of EDCR failure, and the use of mucosal flaps to cover the edges of the ostomy offers an opportunity to minimize the risk of such outcomes. 4,8,18,19 Although a recent study reported that EDCR without mucosal flap preservation can yield highly successful outcomes, 20 instances of failure studies have found that the application of mucosal flap preservation can improve the success rate of subsequent revision surgeries. 6,21 As such, we prefer to employ mucosal flap preservation in EDCR, given the high success rates that have been reported in the literature. 4,8,17 Multiple approaches to producing such mucosal flaps have been reported, although mucosal flaps represent a suboptimal approach as they are often torn or lost when many incisions are made, particularly for less experienced surgeons. Such approaches can also be limited by the fact that mucous flaps are prepared prior to bone removal and as such they are not designed based upon the size of the dacryocyst flap or the region of bone exposure. 4,8 In the present report, we generated a lobulated pedicled nasal mucosa flap by initially generating a single large incision to expose the lacrimal sac and then lobulating this flap based on the sizes of the dacryocyst flap and exposed region of bone. We used the superior portion of this flap to cover the upper and anterior edges of the ostium, while the inferior portion was interlaced with and covered the ‘]’-shaped lacrimal mucosal flap and the lower edges of the ostium. This strategy allowed us to fully cover exposed bone using these mucosal flaps, thus facilitating primary lacrimal sac and nasal mucosa healing, marsupializing the lacrimal sac within the lateral nasal wall. Coverage of the bone with these mucosal flaps also has the potential to reduce rates of cicatricial closure and restenosis.
Multiple studies have sought to determine whether the intraoperative use of a silicone stent is warranted for EDCR operations, with several determining that long-term outcomes do not differ significantly when comparing patients with and without stenting. 9,10,22 Indeed, in one previous report, Pseudomonas infections were found to arise more often in patients treated via the extended deployment of stents within the lacrimal sac, leading to higher rates of DCR failure. 23 The appropriate amount of time for stenting is not universally agreed upon, and silicone tubes have the potential to drive granulation and to thereby elevate failure rates. 12 In the present report, we obtained high success rates without the need for the intraoperative deployment of silicone stents.
All patients included in this retrospective study were first diagnosed by an ophthalmologist prior to transfer to our department, and as a consequence, this study was limited by various factors including small sample size and the lack of a control group (EDCR with stenting). Such factors would have better allowed us to statistically validate the outcomes of the present study.
Conclusion
The lobulated pedicled nasal mucosa flap technique described herein is a safe and simple approach to conducting EDCR. As such it warrants utilization as a surgical approach to such operations, yielding satisfactory rates of positive subjective and objective clinical outcomes without the need for stenting.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.