
Abstract
Introduction:
Posttransplant lymphoproliferative disorder (PTLD) is a serious disease that usually occurs after solid organ transplant and stem cell transplant. Posttransplant lymphoproliferative disorder often involves the head and neck, but it is rare to present as a nasal deformity. Here, we describe a case of external nasal enlargement resulting from PTLD.
Case report:
A 40-year-old man presented with an enlarged external nose half a year ago. The nasal ala thickened, and the external nose was gradually enlarged, accompanied by bilateral nasal obstructions. A biopsy was taken under endoscopy procedure, and the result suggested a diagnosis of PTLD.
Discussion:
Posttransplant lymphoproliferative disorder usually appears in lymphoid tissues that form Waldeyer’s rings or cervical lymph nodes in the head and neck. The early involvement of other head and neck subpoints is considered rare. This case is the first report of PTLD presenting as an external nasal deformity. The symptoms and clinical manifestations of PTLD in otorhinolaryngology are usually diverse and nonspecific but are early symptoms in the clinical course of PTLD.
Introduction
Posttransplant lymphoproliferative disorder (PTLD) is a serious disease that can occur after organ and bone marrow hematopoietic stem cell transplantation; PTLD includes a diverse group of abnormal lymphoid growths. 1 Posttransplant lymphoproliferative disorder often involves the head and neck, but the presentation of PTLD as a nasal deformity is rare. Here, we describe a case of external nasal enlargement resulting from PTLD.
Case Report
A 40-year-old man presented with the gradual enlargement of the external nose over the course of half a year that was accompanied by bilateral nasal obstruction with gradual aggravation, with a stuffy right ear, but no nose bleeds and nasal pain. He had undergone a liver transplant 6 years ago for autoimmune cholangitis and had been taking the anti-rejection drug tacrolimus since the surgery. The physical examination showed enlargement of the external nose (Figure 1). The swollen areas included the tip of the nose, the ala, and the dorsum of the nose. The skin of the external nose was normal, without redness, swelling, or congestion, and there was no tenderness in the external nose. The surface of the nasal vestibule and the anterior part of the proper nasal cavity was smooth, with the obvious swelling of the local soft tissue, leading to the narrowing of the bilateral inner nostrils. A computed tomography scan showed irregular soft tissue density in the anterior part of the nasal septum, nasal vestibule, and bilateral alar region. A magnetic resonance imaging scan (Figure 2) showed multiple abnormal signals in the bilateral inferior turbinate, nasal septum, nasal soft tissue, right nasopharyngeal wall, right temporal bone, and mastoid region. A series of blood examinations indicated positivity for Epstein-Barr virus (EBV) immunoglobulin G, while the test was negative for EBV immunoglobulin M, and no EBV DNA was detected. The routine blood tests were in the normal ranges. To reach a clear diagnosis as soon as possible, we performed a biopsy of the swollen site under endoscopy procedure and general anesthesia. The mucoperiosteum was incised longitudinally through an incision in the nasal septum. During the operation, swelling and proliferation of the submucosal tissue were observed, although the cartilage structure was normal. Cartilage and abnormal submucous tissue samples (3 mm3) were obtained for pathological examination, and then the incision was sutured. The pathological reports (Figure 3) suggested that the fibrous stroma was markedly proliferated with a large amount of lymphocyte plasma cell infiltration, which led to a diagnosis of PTLD.

The physical examination showing enlargement of the external nose.
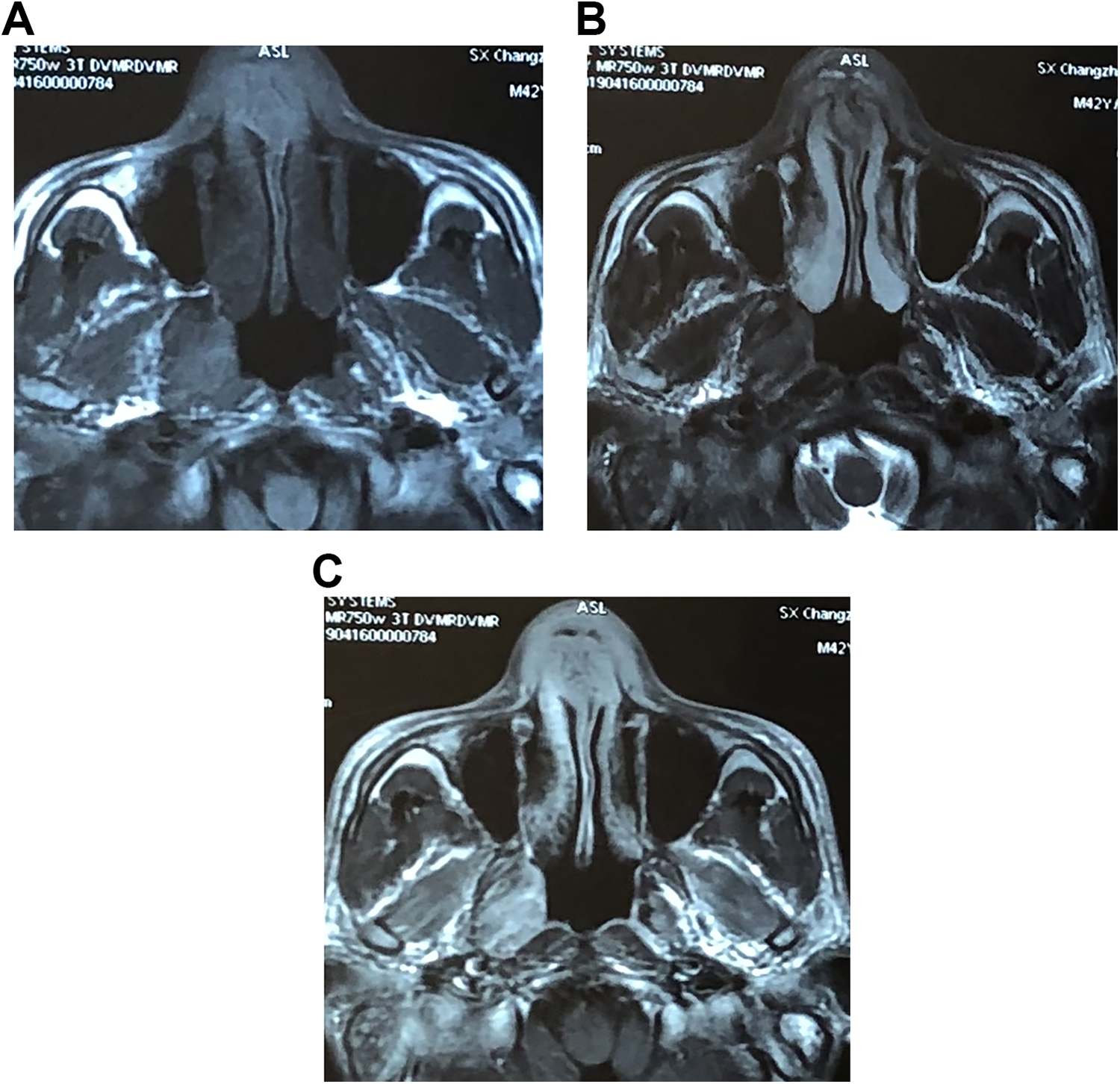
Irregular thickening and an abnormal signal were found in the soft tissue of the anterior part of the nasal septum, the vestibule of the nose, and the bilateral alar of the nose on magnetic resonance imaging, T1 (A) and T2 (B) images, showing a slightly short T1 signal and a slightly long T2 signal, with even and obvious enhancement (C).
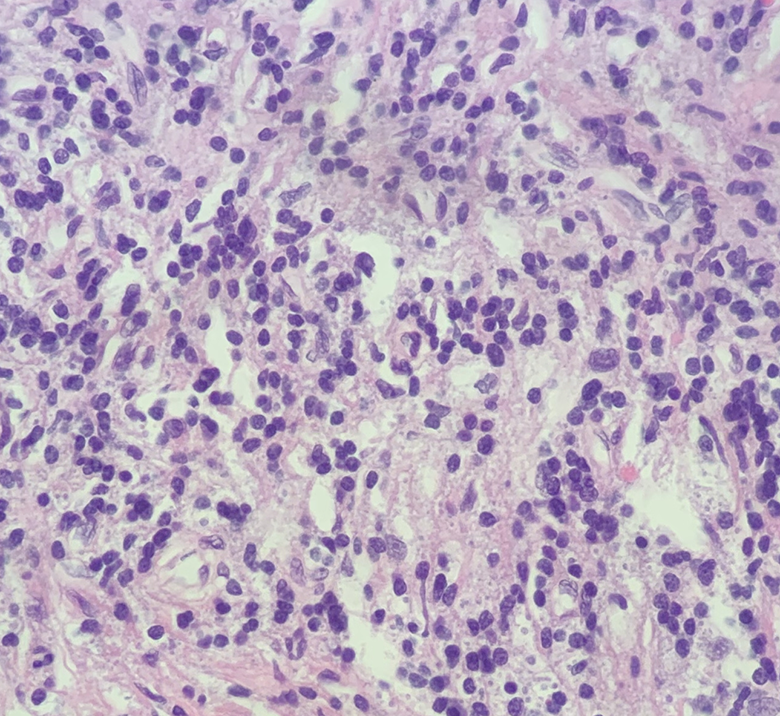
Histological section showing that the fibrous stroma was markedly proliferated with a large amount of lymphocyte plasma cell infiltration (hematoxylin and eosin stain, ×400).
Discussion
After a thorough literature review, this case appears to be the first report of PTLD presenting as an external nasal deformity. Posttransplant lymphoproliferative disorder was first described 30 years ago as a complication in immunosuppressed patients that can arise at any time after transplant, with a mean onset time of 26 months. 2,3 The main risk factors for PTLD are the degree of immunosuppression and an EBV-naive status of the recipient, but the age and race of the recipient, type of transplant, and genetic factors are also related to the incidence. 4 Posttransplant lymphoproliferative disorder has a variety of pathological manifestations, ranging from low-grade lymphoid proliferation to aggressive monomorphic and clonal lesions that are most commonly classified as diffuse large B-cell lymphoma. 5 The prognosis of polymorphic PTLD is better than that of monoclonal PTLD. Only 21% of polymorphic PTLD has clinically aggressive behavior, while the mortality of patients with monoclonal PTLD is 67%. 6 It has been reported that 60% to 80% of PTLD patients are positive for EBV. Posttransplant lymphoproliferative disorder related to EBV infection is most common within the first 2 years after liver transplantation, and non-EBV-related PTLD tends to occur later; non-EBV-related PTLD is usually monoclonal. 7 The patients were negative for EBV DNA in our case, and he developed PTLD 6 years after transplantation; the underlying mechanism is unclear.
This patient began to experience enlargement of the external nose and secretory otitis media 6 months before presenting in our department. The swollen external nose appeared as a frog’s nasal deformity, which is rarely observed in otolaryngology. A frog’s nasal deformity may occur in patients with a midline nasal mass (including a dermoid cyst, nasal glioma, or encephalocele 8 ), chronic sinusitis with nasal polyps, infections, and tumors. However, in this case, the symptoms and signs did not support the diagnosis of infection. In addition, no space-occupying manifestations of the nasal cavity or paranasal sinuses were found on the physical and imaging examinations (Figure 2). The diagnosis of midline space-occupying manifestation was also not supported. First, the majority of midline space-occupying manifestations are seen in children; second, these lesions usually have intracranial communication or expansion to the brain. 8 The unique swelling of the external nose and the anterior part of the nasal septum in this case suggested the involvement of lymphoma or other special diseases. Considering the continuous use of oral tacrolimus anti-rejection therapy after liver transplantation, PTLD was highly likely in our case. However, there has been no report of PTLD occurring at this site.
Posttransplant lymphoproliferative disorder in otolaryngology is relatively common in children and accounting for 25% of all PTLD cases in literature reports. 9 Head and neck PTLD is most commonly observed in the lymphoid tissue that forms Waldeyer’s ring or neck lymph nodes, and the involvement of other sites was previously considered rare. 9,10 Such manifestations commonly include adenotonsillar hypertrophy, tonsillitis, or cervical lymphadenopathy. One case report described epistaxis as the primary presenting complaint in a patient with PTLD of the nasal cavity or postnasal space. 11 Recently, a study of PTLD in the nasal cavity of children after lung transplantation showed that the nasal cavity is the most common site of PTLD in the head and neck after lung transplantation, 12 which suggests that the incidence of sinonasal PTLD may be higher than previously believed. After a thorough search of PubMed, no case of PTLD presenting as an enlargement of the nasus externus has been reported. Therefore, the clinical manifestations of PTLD are nonspecific. A diagnosis of PTLD should be considered for patients with rare clinical manifestations and a history of transplantation. Otolaryngeal symptoms are the early manifestations of PTLD, and early detection and intervention are very important. Patients with PTLD in the head and neck area have higher survival rates than those with PTLD with abdominal and thoracic involvement because the former can be detected earlier than the latter. 10
The current treatment options include a reduction in immunosuppressive therapy, antiviral treatment, immunotherapy, surgery, and chemotherapy. For this patient, a reduction in the immunotherapy medication alone led to remission.
Conclusion
Otolaryngological symptoms and clinical findings are often the early manifestations in the clinical course of PTLD, which are usually diverse and nonspecific. To enable a timely diagnosis, it is necessary to determine the patient’s past medical history when encountering diseases that are difficult to diagnose.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The general work performed in this study was supported by the Beijing Natural Science Foundation (grant number 7162066).