
Abstract
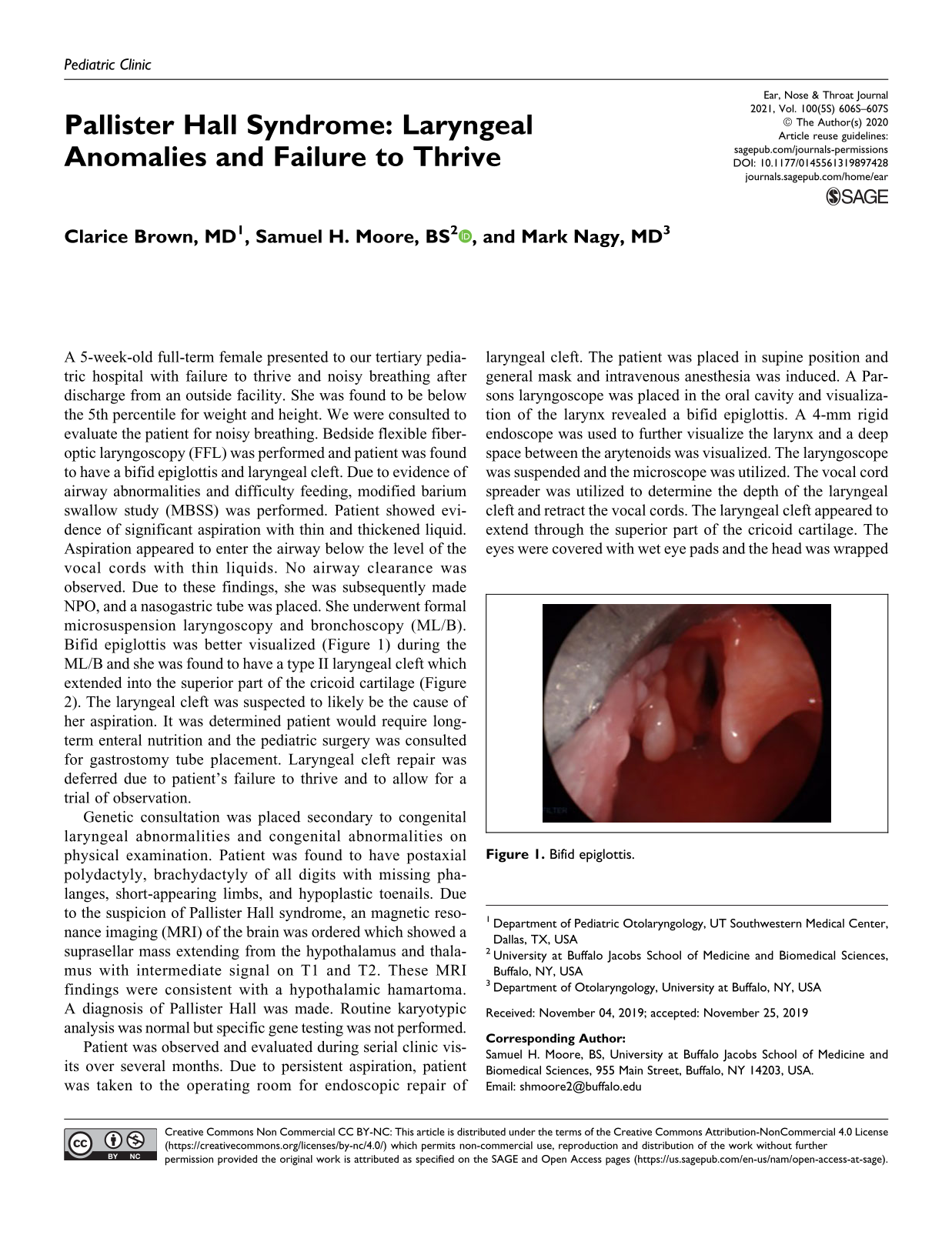
A 5-week-old full-term female presented to our tertiary pediatric hospital with failure to thrive and noisy breathing after discharge from an outside facility. She was found to be below the 5th percentile for weight and height. We were consulted to evaluate the patient for noisy breathing. Bedside flexible fiberoptic laryngoscopy (FFL) was performed and patient was found to have a bifid epiglottis and laryngeal cleft. Due to evidence of airway abnormalities and difficulty feeding, modified barium swallow study (MBSS) was performed. Patient showed evidence of significant aspiration with thin and thickened liquid. Aspiration appeared to enter the airway below the level of the vocal cords with thin liquids. No airway clearance was observed. Due to these findings, she was subsequently made NPO, and a nasogastric tube was placed. She underwent formal microsuspension laryngoscopy and bronchoscopy (ML/B). Bifid epiglottis was better visualized (Figure 1) during the ML/B and she was found to have a type II laryngeal cleft which extended into the superior part of the cricoid cartilage (Figure 2). The laryngeal cleft was suspected to likely be the cause of her aspiration. It was determined patient would require long-term enteral nutrition and the pediatric surgery was consulted for gastrostomy tube placement. Laryngeal cleft repair was deferred due to patient’s failure to thrive and to allow for a trial of observation.

Bifid epiglottis.

Type II laryngeal cleft extending into the superior aspect of the cricoid cartilage. Suction used to retract the right cord to visualize the depth of the cleft.
Genetic consultation was placed secondary to congenital laryngeal abnormalities and congenital abnormalities on physical examination. Patient was found to have postaxial polydactyly, brachydactyly of all digits with missing phalanges, short-appearing limbs, and hypoplastic toenails. Due to the suspicion of Pallister Hall syndrome, an magnetic resonance imaging (MRI) of the brain was ordered which showed a suprasellar mass extending from the hypothalamus and thalamus with intermediate signal on T1 and T2. These MRI findings were consistent with a hypothalamic hamartoma. A diagnosis of Pallister Hall was made. Routine karyotypic analysis was normal but specific gene testing was not performed.
Patient was observed and evaluated during serial clinic visits over several months. Due to persistent aspiration, patient was taken to the operating room for endoscopic repair of laryngeal cleft. The patient was placed in supine position and general mask and intravenous anesthesia was induced. A Parsons laryngoscope was placed in the oral cavity and visualization of the larynx revealed a bifid epiglottis. A 4-mm rigid endoscope was used to further visualize the larynx and a deep space between the arytenoids was visualized. The laryngoscope was suspended and the microscope was utilized. The vocal cord spreader was utilized to determine the depth of the laryngeal cleft and retract the vocal cords. The laryngeal cleft appeared to extend through the superior part of the cricoid cartilage. The eyes were covered with wet eye pads and the head was wrapped with wet towels. All operating personnel had laser safety glasses appropriate for the CO2 laser. Using a curved handpiece and the microscope, the mucosa of the laryngeal cleft was lasered using 6 W with a 0.3 second interval. Between times of intermittent lasering, the patient was intubated orotracheally with a 3.5 endotracheal tube. The endotracheal tube was removed during lasering. After the lasering was completed, 5-0 Vicryl sutures were used to approximate the laryngeal cleft starting from the most distal portion and working proximally (Figure 3). Care was taken to not suture the area adjacent to the arytenoids and this area was also not lasered. At this point, the patient was able to be extubated and was transferred to the postanesthesia recovery room in stable condition.

Superior view of laryngeal cleft repair. Bifid epiglottis in view (black arrow).
She was admitted to the hospital postoperatively and her postoperative course was uncomplicated. She was discharged and seen in clinic where her parents reported no breathing or feeding difficulties. Repeat FFL was performed and continued to show a bifid epiglottis, good healing of laryngeal cleft repair, bilateral vocal cord motion was symmetric and intact, and the remainder of the examination was unremarkable. Repeat MBSS showed no evidence of aspiration. She developed oral aversion secondary to gastrostomy tube dependence, but she was able to tolerate nectar liquid with a spoon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.