
Abstract
Objective:
Type 1 thyroplasty is an established procedure for the treatment of vocal fold paralysis to improve voice and swallowing outcomes. At our institution, we commonly perform this procedure on an outpatient basis in medically stable patients. With this study, we assess the safety of outpatient thyroplasty by examining complication and readmission rates, need for revision surgery, and predictors of these outcome measures.
Methods:
We performed a retrospective review of patients undergoing outpatient type 1 thyroplasty for vocal fold paralysis between 2013 and 2018 at our institution. We documented the etiology of paralysis, comorbidities, and demographic data. Our primary outcome measures were complications, need for readmission, and need for revision surgery.
Results:
During the study period, 160 patients met our inclusion criteria. Mean age at time of surgery was 62.1 ± 13.9 years; there were 82 (51%) males and 78 (49%) females. Nine (5.6%) patients experienced major complications after surgery and 7 (4.4%) patients required unplanned readmission. Mean time to complication was 6.9 ± 9.7 days. There were no instances of postoperative airway compromise requiring intervention. There were no mortalities. Of those who underwent primary surgery, 22 (14%) patients required revision surgery.
Conclusion:
Given that complications tend to occur in a delayed fashion rather than in the acute postoperative period, same-day discharge seems reasonable as compared to overnight observation in medically stable patients undergoing type 1 thyroplasty.
Level of Evidence:
IV
Introduction
Glottic insufficiency can have a significant impact on a patient’s quality of life and is a commonly encountered complaint in otolaryngology. It is characterized by the incomplete closure of the vocal folds when phonating or swallowing, potentially resulting in weak voice, weak cough, and an increased risk of dysphagia and aspiration. Glottic insufficiency due to vocal fold paralysis is most commonly caused by iatrogenic damage to the recurrent laryngeal nerve (RLN) during surgery. However, it can also occur secondary to intubation, direct compression or invasion of the RLN by malignancy, or due to idiopathic causes. 1,2 Glottic insufficiency can also result from vocal fold atrophy. This is seen as a common change with age and a sequela of neuromuscular disease.
A variety of treatment options are available for glottic insufficiency, ranging from voice therapy to surgical intervention. Surgical options include injection laryngoplasty, laryngeal reinnervation, and laryngeal framework surgery, such as unilateral or bilateral type 1 thyroplasty. 3 Type 1 thyroplasty, first described by Isshiki et al in 1975, is an established procedure for the treatment of vocal fold paralysis to improve voice and swallowing outcomes. 4 -8 This technique is particularly advantageous, as it can be performed under sedative anesthesia, allowing simultaneous laryngoscopy and voice assessment. The degree of medialization can be adjusted in the operating room (OR) as well as assessing for any airway complaints. The implant is inserted through a window in the thyroid cartilage lateral to the thyroarytenoid muscle ipsilateral to the side of weakness or atrophy. The procedure most commonly involves the placement of Silastic (Bentec Medical, Inc, Woodland, California) or Gore-Tex (W.L. Gore & Associates, Inc, Flagstaff, Arizona) implants, with no reported difference in outcomes based on implant type. 9
Although thyroplasty was originally described as an outpatient procedure, it is often performed in an inpatient setting due to concerns regarding acute airway complications. 10,11 Various studies have discussed procedure-related complications after surgical treatment for glottic insufficiency. Major complications reported include airway compromise requiring intubation or tracheostomy, hematoma requiring wound evacuation, pharyngocutaneous fistula formation, or implant extrusion. 10,12 -14 Despite reports of these complications, most patients do well and do not require overnight admission. At our institution, we commonly perform type 1 thyroplasty on an outpatient basis and discharge patients on the same day as surgery. Intraoperatively, patients are given antibiotics and steroids, and they are discharged home on a prednisone taper. We present our experience with type 1 thyroplasty performed on an outpatient basis in patients whose other medical conditions would not preclude ambulatory surgery. This study reviews the safety and efficacy of outpatient thyroplasty by examining incidence and timing of postoperative complications, the need for revision surgery, and predictors of these outcome measures to determine which patients may benefit from inpatient observation and close follow-up.
Materials and Methods
Following institutional review board approval, we compiled clinical information on all patients aged 18 years and older undergoing type 1 thyroplasty as an outpatient procedure from 2013 to 2018 in the Department of Otolaryngology—Head and Neck Surgery, Thomas Jefferson University Hospital. Institutional review board approval by the Thomas Jefferson University Division of Human Subjects Protection was obtained to create a database with both demographic and clinical data. Variables evaluated included the following: etiology of vocal cord paralysis, demographics (age, body mass index [BMI], gender), medical comorbidities, history of previous neck surgery or radiation, history of previous cordectomy, and need for revision procedures. History of prior treatments such as vocal cord injection was also recorded. Procedure characteristics evaluated included laterality of the procedure (left, right, bilateral), new or revision case, type of implant (Silastic or Gore-Tex), operative time, and length of hospital stay. Information regarding both intraoperative and postoperative complications within 3 months of surgery and unplanned readmission were also collected.
Descriptive statistics were computed for the entire study cohort, and quantitative data are presented in mean ± standard deviation. Student t tests were used to analyze continuous variables; Fisher exact test was used to compare qualitative data where appropriate. Univariate and multivariate analyses were performed to evaluate predictive factors associated with major postoperative complications and need for revision surgery. A significance level of P < .05 was used. All analyses were performed using SPSS software, version 26 (IBM, Armonk, New York).
Postoperative Management
No drains are placed during surgery. Postoperatively, all patients are placed a short course of oral steroids and are evaluated in the office 1 week after surgery.
Results
Demographics and Operative Characteristics
A total of 160 patients underwent outpatient type 1 thyroplasty and met criteria for inclusion in this study. Mean age at time of outpatient surgery was 62.1 ± 13.9 years (range, 19-92 years); there were 82 (51%) males and 78 (49%) females. Overall demographic data are shown in Table 1.
Patient Demographic Data.a
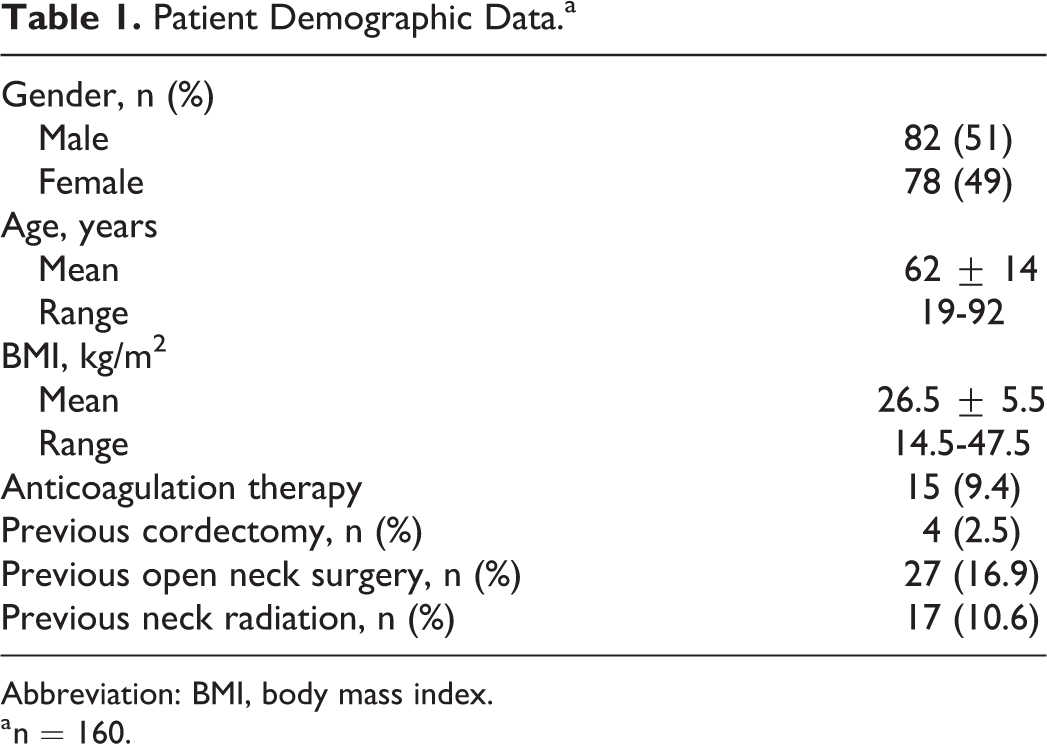
Abbreviation: BMI, body mass index.
a n = 160.
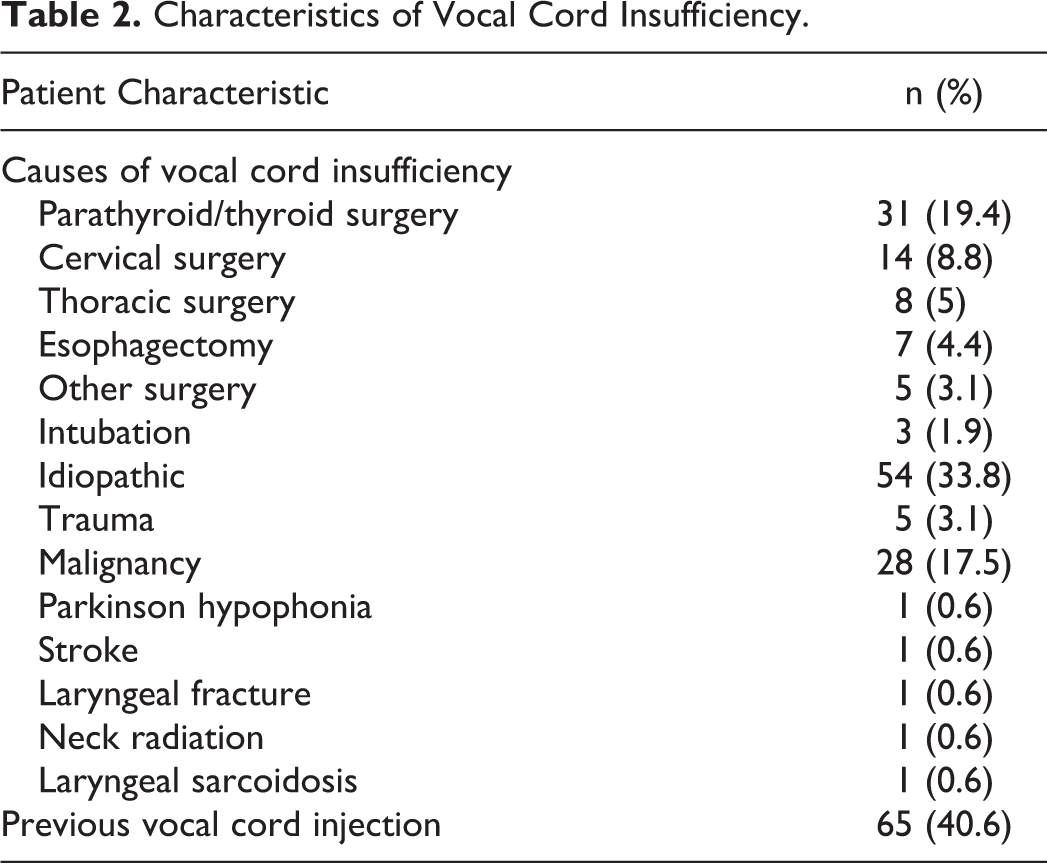
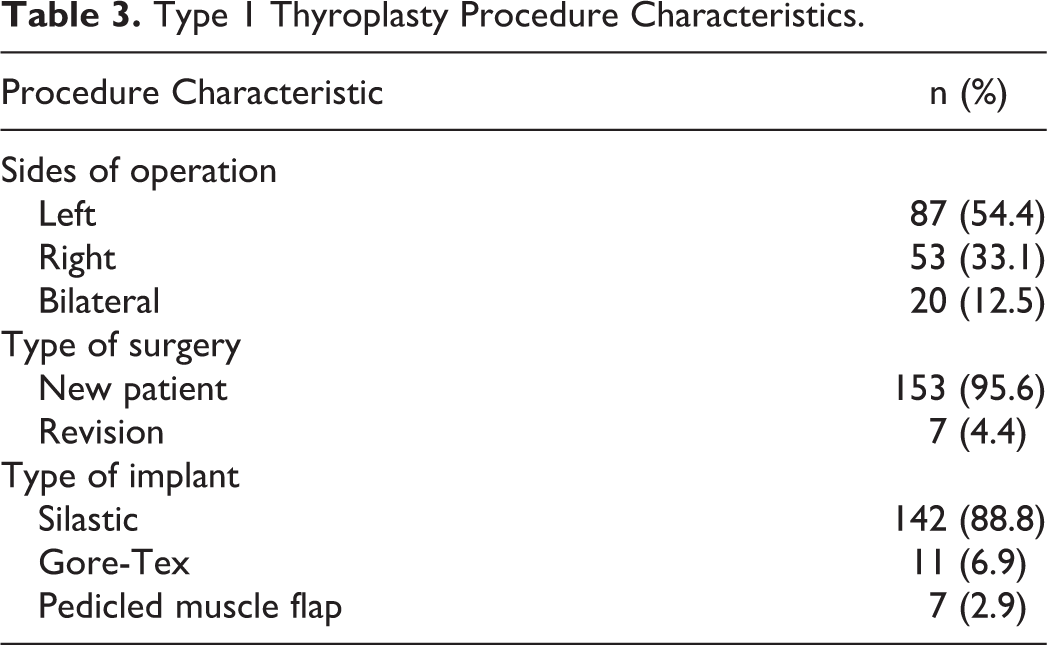
The etiology of glottic insufficiency is shown in Table 2. The most common causes of glottic insufficiency were iatrogenic operative injury (56%), followed by idiopathic etiologies (33%) and malignancy (18%). Thyroid surgery (18%) and anterior cervical spine surgery (9%) were the leading operative causes for vocal cord dysfunction and paralysis. Procedure characteristics are summarized in Table 3. In our cohort, 65 (41%) patients underwent prior treatment with vocal cord injection and 7 (4%) patients had a previous type 1 thyroplasty. Fifty-three (33%) patients underwent right sided surgery, 87 (54%) had left-sided surgery, and 20 (13%) had bilateral surgery.
Characteristics of Vocal Cord Insufficiency.
Type 1 Thyroplasty Procedure Characteristics.
Complications
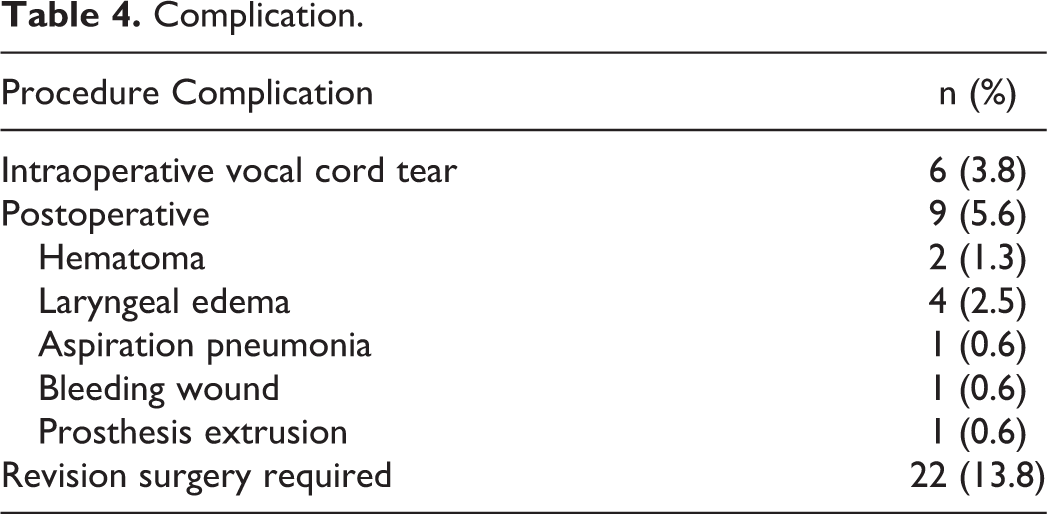
Surgical complications (Table 4) were classified as either intraoperative or postoperative. Major postoperative complications were classified as complications that resulted in prolonged hospitalization or readmission, higher acuity of care, or necessitated a return to the OR. Minor complications were defined as complications observed during routine office visit or reported by patient phone call requiring medical treatment or outpatient observation. Nine (5.6%) cases involved major complications: hematoma (2), hemorrhage (1), prosthesis extrusion (1), laryngeal edema (4), and aspiration pneumonia (1). Overall mean time to postoperative complication was 6.9 ± 9.7 days (range, 0-32 days). Intraoperative vocal cord tears occurred in 6 (3.8%) cases. All cases were repaired using a transposition muscle flap with sternohyoid or sternothyroid muscle; all patients were discharged the same day as surgery and recovered with no further complications. Eight (5.0%) cases involved minor complications: wound complications treated in-office (3), mild laryngeal edema treated with short-term steroids (4), and low-volume hemoptysis (1).
Complication.
Only 2 cases of hematoma and 1 case of postoperative hemorrhage were observed. One case occurred in a patient after restarting anticoagulation therapy with apixaban due to underlying atrial fibrillation; bedside evacuation was performed under local anesthesia. Another patient had a hematoma and bleeding from the incision site on postoperative day 1 (POD1) requiring operative neck exploration to control the bleeding. A third patient had postoperative wound hemorrhage and severe ecchymosis over the neck and chest in the setting of prior warfarin use; the patient was observed in the hospital for 2 days and his symptoms resolved without further complication.
Laryngeal edema was observed in 4 patients following surgery. All 4 patients presented with moderate-to-severe dyspnea within 1 week of surgery and were admitted overnight for treatment with steroids and antibiotics. One patient presented with symptoms during planned clinical follow-up visits and 3 presented to the emergency department; 2 patients presented on POD1 and 2 presented on POD6. There were no instances of postoperative airway compromise requiring intubation or tracheostomy placement. One patient had an aspiration pneumonia of the right lower lobe confirmed on chest X-ray. He was treated with moxifloxacin and discharged on POD1. There was one case of implant extrusion at 4 weeks after initial surgery that presented as persistent dysphagia, inflammation, and vocal cord swelling; the patient was taken to the OR for revision surgery at which time an extruded implant was observed and replaced.
A total of 7 (4.4%) patients required readmission for management of postoperative complications; 3 (1.9%) patients were taken back to the OR. Inpatient stay after readmission was 1 to 2 days for all patients. Of the 20 patients who underwent bilateral thyroplasty, there was one case of mild laryngeal edema treated with oral antibiotics and steroids. In the 7 patients who underwent revision thyroplasty, there was one case of a minor wound infection treated with oral antibiotics. There were no predictors for postoperative complication found on univariate analysis (Table 5). There were no mortalities.
Logistic Regression Analysis of Factors Affecting Overall Complication Compared to Noncomplication Group.
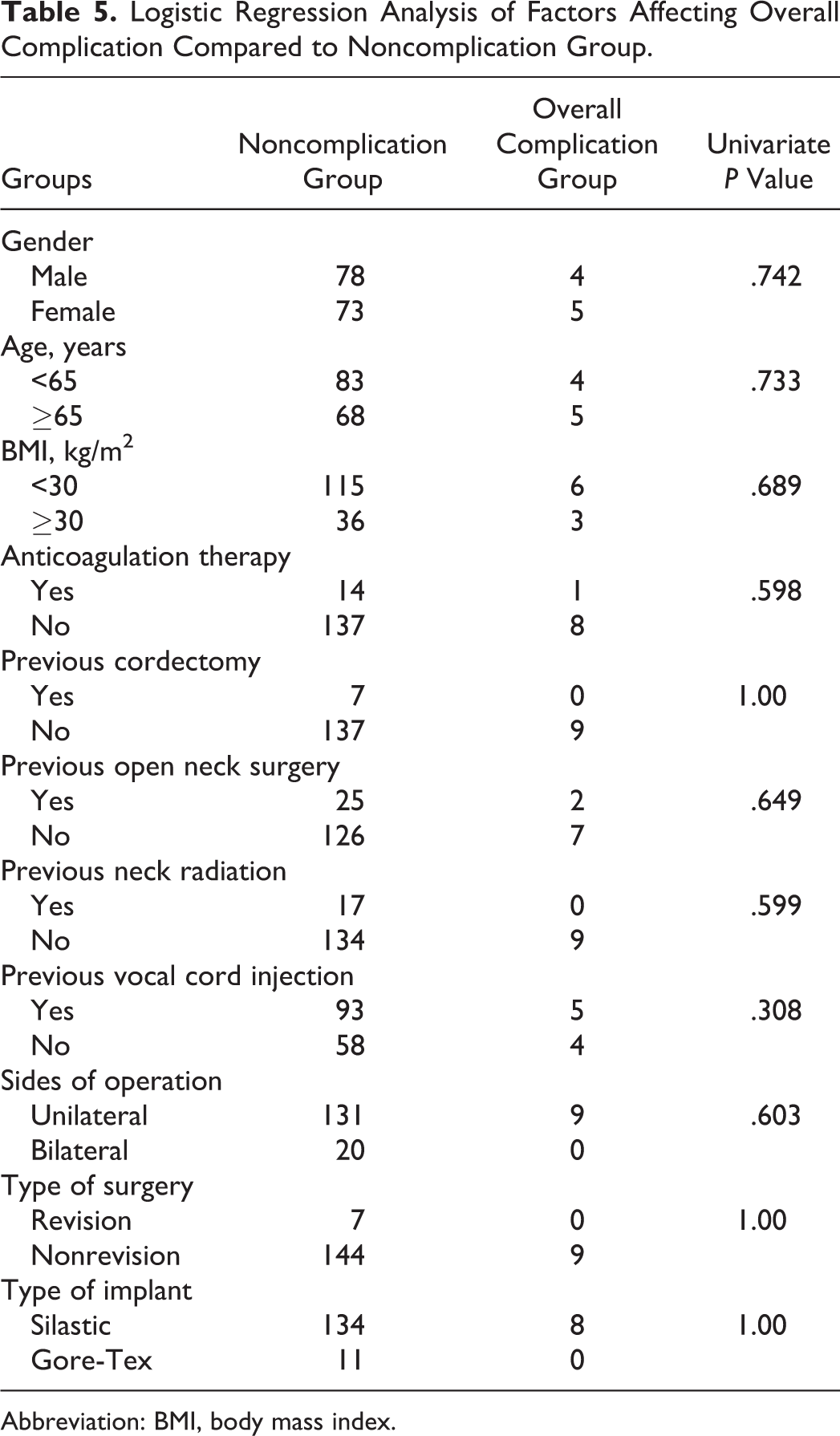
Abbreviation: BMI, body mass index.
Revision Thyroplasty
Of the 152 patients who underwent primary type 1 thyroplasty, 22 (14%) patients required revision surgery. Mean time to revision surgery was 7.5 ± 6.0 months (range, 1.4-20.7 months). Seventeen (77%) patients required resizing of the implant due to overmedialization or incomplete glottic closure, 4 (18%) patients needed replacement of the implant due to implant migration, and 1 (5%) patient had implant extrusion. Three patients experienced minor postoperative complications; there was only 1 case of mild laryngeal edema and 2 cases of wound complications that resolved with outpatient treatment. To predict the odds of the need for revision surgery, binary logistic regression analysis was performed between the nonrevision surgery group and revision surgery group, as shown in Table 6. Variables included in the multivariate analysis were chosen from those with a P value < .2 from the univariate analysis. The only demographics or comorbidities found predictive of the need for revision surgery on univariate analysis were prior history of cordectomy and BMI <30 kg/m2 (P = .099, P = .016, respectively). On multivariate analysis, both variables fell out of significance and there were no overall predictors for revision surgery.
Logistic Regression Analysis of Factors Affecting Need for Revision Surgery Compared to Nonrevision Group.a
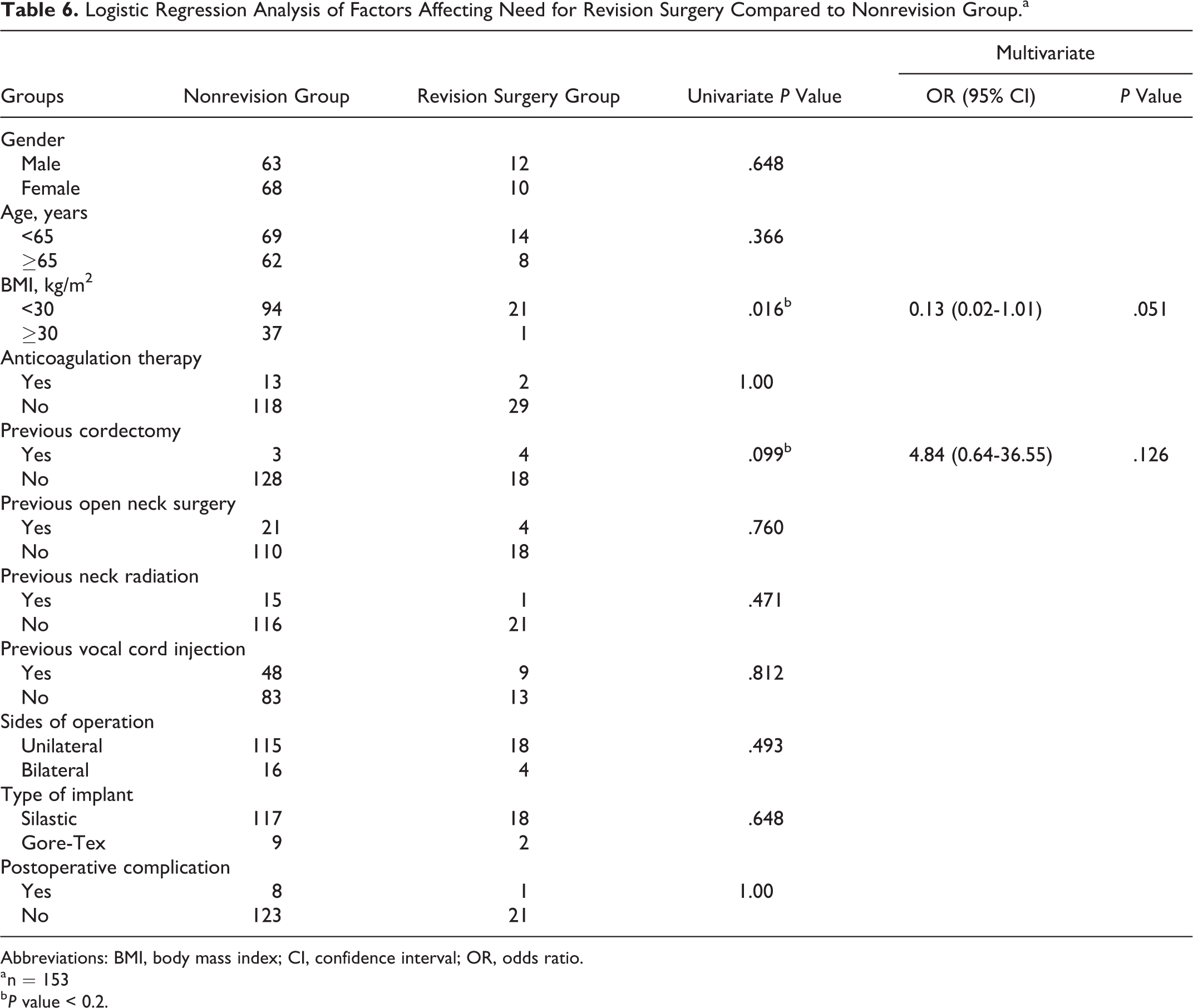
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio.
a n = 153
b P value < 0.2.
Discussion
Glottic insufficiency can have a significant impact on patients’ quality of life. In this study, iatrogenic operative injury was the most common cause of glottic insufficiency, which is higher than previously reported series. 1,15 The majority of these were patients who had undergone previous thyroid surgery. Idiopathic vocal cord paralysis was the second most common etiology of insufficiency. Medialization thyroplasty is the most widely used technique for surgically treating vocal cord weakness. 16 Previous studies have reported major complications associated with type 1 thyroplasty, including airway compromise necessitating intubation or tracheostomy placement, obstructive hematomas, fistula formation, wound infection, or implant extrusion. Thus, some institutions continue to admit patients for overnight observation after surgery.
As health-care costs continue to grow and an emphasis is placed on quality improvement and patient safety, many practices have started performing type 1 thyroplasty in an outpatient setting. In a recent study looking at national claims data, outpatient same-day discharge represented 62.0% (1142/1843) of total patients undergoing type 1 thyroplasty, with the number steadily increasing over the past 10 years. 17 Many studies advocate for risk stratification based on patient comorbidities to determine whether a patient may require postoperative observation to prevent major complications, specifically airway compromise. 15,18 -20 The 2 operating surgeons (M.B. and J.S.) had similar discharge criteria; patients were sent home if there were no significant medical comorbidities, no intraoperative complications, and no clinical suspicion of postoperative hemorrhage or airway obstruction after surgery. Our study, by identifying all patients within a specified time period who underwent the same procedure in an ambulatory setting, affords the opportunity to objectively evaluate outcomes after outpatient type 1 thyroplasty.
The reported complication rate for patients undergoing type 1 thyroplasty is between 7% and 20%. 12,13,15,17,18,19 - 22 However, our study found a major complication rate of 5.6% with no long-term morbidity or mortalities. There were 4 cases of airway complications that were considered major; however, none of the patients required intubation or tracheostomy. Airway complications resulted from laryngeal mucosal edema, which was confirmed by endoscopic examination, and all occurrences improved after 1 to 2 days with systemic corticosteroid and antibiotic administration. These data fit well with other published reports. Of the 214 patients who underwent outpatient type 1 thyroplasty in studies published by Chau et al, 19 Junlapan et al, 15 Cotter et al, 13 Zhao et al, 20 and Bray et al, 18 there were no obstructive hematomas or need for intubation or surgical airway intervention in the acute postoperative period. The only complications of nonobstructive hematoma and implant extrusion occurred in patients on anticoagulation and in patients with poor implant placement or prior radiation therapy, respectively. 13,15 In our series, there was a one case of implant extrusion due to persistent infection and granulation tissue deposition at the site of primary surgery.
Univariate and multivariate logistic regression analysis did not show any predictors for overall complications. Specifically, discontinuing anticoagulation therapy prior to surgery did not increase the risk of intraoperative or postoperative complications, including myocardial infarction or thrombotic event. This study confirms that it is safe to continue to recommend that patients stop anticoagulation therapy prior to surgery, as directed by their cardiologist or other treating physician, and that it is safe to resume therapy in the early postoperative period without significant risk of bleeding. Additionally, drains are not routinely placed at our institution after surgery; this study reinforces that drain placement is not required. Finally, logistic regression analysis showed that previous neck radiation did not increase risk of overall complications or need for revision surgery, suggesting that outpatient type 1 thyroplasty may be considered in this patient population. This finding is consistent with studies by Rosow et al 23 and White et al, 24 demonstrating that patients who had undergone previous radiation therapy to the head and neck did not have an increased complication rate when compared with nonirradiated patients.
The rate for revision thyroplasty achieved in this study was 14%, which was slightly higher than that seen in previous studies. 15,25,26 Multivariate analysis did not show any overall predictors for revision surgery. Specifically, patients with a history of prior cordectomy for the treatment of early-stage laryngeal cancer had good outcomes after primary thyroplasty and were not at increased risk of undergoing secondary procedures. This finding is in accordance with the current literature, which has found thyroplasty to be a safe and effective method for closing glottic gaps after extended or total cordectomy. 26 -28
This study has several limitations. It is difficult to generalize these experiences to other institutions, given the variability in patient populations and surgeon experience. By demonstrating comparably low complication rates that correlate well with previously published data, the external validity of these results is increased.
Conclusion
Major complications, which included transient airway compromise and hematoma, occurred in 5.6% of patients. Given that complications tend to occur in a delayed fashion rather than in the acute postoperative period, same-day discharge seems reasonable as compared to overnight observation in medically stable patients undergoing type 1 thyroplasty; in both cases, patients need to be aware of potential for hemorrhage, hematoma, and laryngeal edema.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.