
Abstract
Introduction:
In squamous cell carcinomas of the oral cavity, factors that can predict prognosis are being studied. However, new prognostic factors are needed to provide information on the biological properties of tumors. Galectin-3 is known to be involved in many biological events such as cell adhesion and differentiation, angiogenesis, apoptosis, tumorigenesis, and metastasis. In our study, the prognostic role of galectin-3 expression in squamous cell carcinomas of the oral cavity was investigated.
Materials and Methods:
The study included 60 patients with a diagnosis of squamous cell carcinoma of the oral cavity. The demographic characteristics of the patients were compiled from the patient files. Galectin-3 expression was studied immunohistochemically. Cytoplasmic and nuclear expressions of galectin-3 were evaluated separately. In addition, the total expression score was calculated by multiplying the percentage and intensity scores for each cases. The critical expression score was determined according to the median value of the total scores.
Results:
Among 60 cases, 28 tumors were located on the lip, 21 on the tongue, 4 on the floor of the mouth, 3 on the orobuccal mucosa, 3 on the retromolar trigone, and 1 on the gingivobuccal junction. There was no statistically significant relationship between prognosis and nuclear or cytoplasmic galectin-3 expression. Tumor grade and invasion pattern were found to be associated with the galectin-3 total expression score.
Conclusion:
Although galectin-3 total expression score was correlated with the tumor grade and invasion pattern, it is not associated with overall survival or recurrence rates. However, there is a need for a large series of cases in which methods are standardized in order to clarify the prognostic role of galectin-3 expression in oral squamous cell carcinomas.
Introduction
Oral squamous cell carcinoma accounts for 90% of oral malignancies and is the sixth most common cancer worldwide. 1 Despite the improvements in treatment modalities in recent years, 5-year survival rate, is around 50% to 55%, has not increased significantly. 2
Prediction of prognosis in oral cavity cancers is crucial in determining the optimal treatment. Many factors such as stage, size of lesion, depth of invasion, pattern of invasion, perineural, lymphatic and vascular invasion, surgical margin status, nodal involvement, microvessel density, and lymphocytic response have been demonstrated as potential prognostic factors. 3 -5 Since patients with similar clinicopathological features may differ significantly in their clinical course, new prognostic factors are needed to predict the biological behavior of these tumors.
In recent years, the search for new prognostic factors that can help predict the biological behavior of tumors more reliably is focused on the role of various molecular markers. The prognostic role of galectin-3, one of these markers, is being investigated in various types of cancer. 6 -9 Galectin-3 is known to play a role in many biological events such as cell adhesion, differentiation, angiogenesis, apoptosis, tumorigenesis, and metastasis. 10 Galectin-3 is often overexpressed in cancer cells and cancer-related stromal cells. Galectin-3 is suggested to be a target protein in the treatment of cancer. It is predicted that the efficiency of chemotherapy can be increased in various types of cancer by inactivation of this protein. 11 There are few studies in the literature investigating the prognostic significance of galectin-3 expression in squamous cell carcinoma of the oral cavity. The aim of this study is to investigate the prognostic role of galectin-3 expression in squamous cell carcinomas of the oral cavity.
Materials and Methods
A total of 60 cases diagnosed as squamous cell carcinoma of the oral cavity between 2001 and 2012 at our department were included in the study. Of these tumors, 28 were located on the lip, 21 on the tongue, 4 on the floor of the mouth, 3 on the orobuccal mucosa, 3 on the retromolar trigone, and 1 on the gingivobuccal junction. Information such as age of the patients, tumor dimension, presence of metastasis, tumor-node-metastasis (TNM) stage, chemotherapy or radiotherapy, tumor localization, the time after the first diagnosis in case of recurrence, and the duration of survival was obtained from the files of otorhinolaryngology department.
The histological sections stained with hematoxylin and eosin of the tumors, which were prepared previously were re-evaluated. Microscopic features such as tumor grade, depth of invasion, pattern of invasion, presence of perineural and/or vascular invasion, presence of lymph node involvement, extracapsular tumoral extension in metastatic lymph nodes, and status of surgical borders were evaluated again.
The paraffin blocks of the resection materials that best reflect tumor morphology were studied via immunohistochemical staining for galectin-3 antibody (9C4; Novocastra, Newcastle, United Kingdom). The paraffin blocks were cut into 4 μm-thick sections, and the slides were deparaffinized. Then, immunoperoxidase staining was completed using an automatic staining machine (Ventana BenchMark XT Automated IHC/ISH slide staining system, Tucson, AZ, USA) in accordance with the manufacturer’s instructions. Chromogeneous diaminobenzidine was used for signal detection, and the cells were counterstained with Harris hematoxylin. The negative controls were incubated with the same concentration of immunoglobulin (IgG1; Dako, Ely, United Kingdom) instead of the primary antibody. The positive controls were papillary carcinoma of the thyroid gland.
Immunohistochemical staining assessment was performed according to the following 3 different methods reported in the literature
8,9,12,13
: Cases with nuclear staining for galectin-3 in tumor cells were considered to be positive, regardless of the percentage of staining, and cases with no nuclear staining were considered negative. Cases with cytoplasmic galectin-3 expression in more than 5% of tumor cells were considered as high and less than 5% as low cytoplasmic expression. Cytoplasmic galectin-3 expression level was evaluated using the following scale: 0 (less than 1% of tumor cells stain), 1+ (1%-10% of tumor cells), 2+ (11%-50% of tumor cells), and 3+ (>50% of tumor cells). The staining intensity was also evaluated as 1+ (mild), 2+ (moderate), or 3+ (intense). The total expression score was obtained by multiplying the percentage and intensity scores for each cases. The critical expression score was determined according to the median value of the total scores.
In statistical analysis, the chi-square tests (Fisher exact and Yates) were used to compare various clinicopathological parameters with galectin-3 expression groups. Cox regression analysis was used to evaluate the relationship between recurrence and death with various clinicopathological parameters and galectin-3 expression.
Results
Of the 60 patients included in the study, 39 (65%) were male and 21 (35%) were female, with a mean age of 64.1 (range, 34-93). Twenty-one (35%) of the cases were younger than 60 years and 39 (65%) were older than 60 years. The majority of tumors (31/60 cases, 51.7%) were clinical stage I. Clinical stage IV tumors were found in 11 (18.3%) patients. The follow-up period of the cases ranged between 5 and 136 months (mean, 57.4 months). Of 60 patients, 51 were treated with surgery, and 9 patients who refused surgical treatment were treated with chemoradiotherapy. Adjuvant radiotherapy was performed in 36 of 51 patients who were treated with surgery. During the follow-up period, 15 (25%) patients had recurrence. In the follow-up period, 14 cases (23.3%) died due to disease-related causes. The clinicopathological features of the cases are shown in Table 1.
Clinicopathological Features of the Patients.
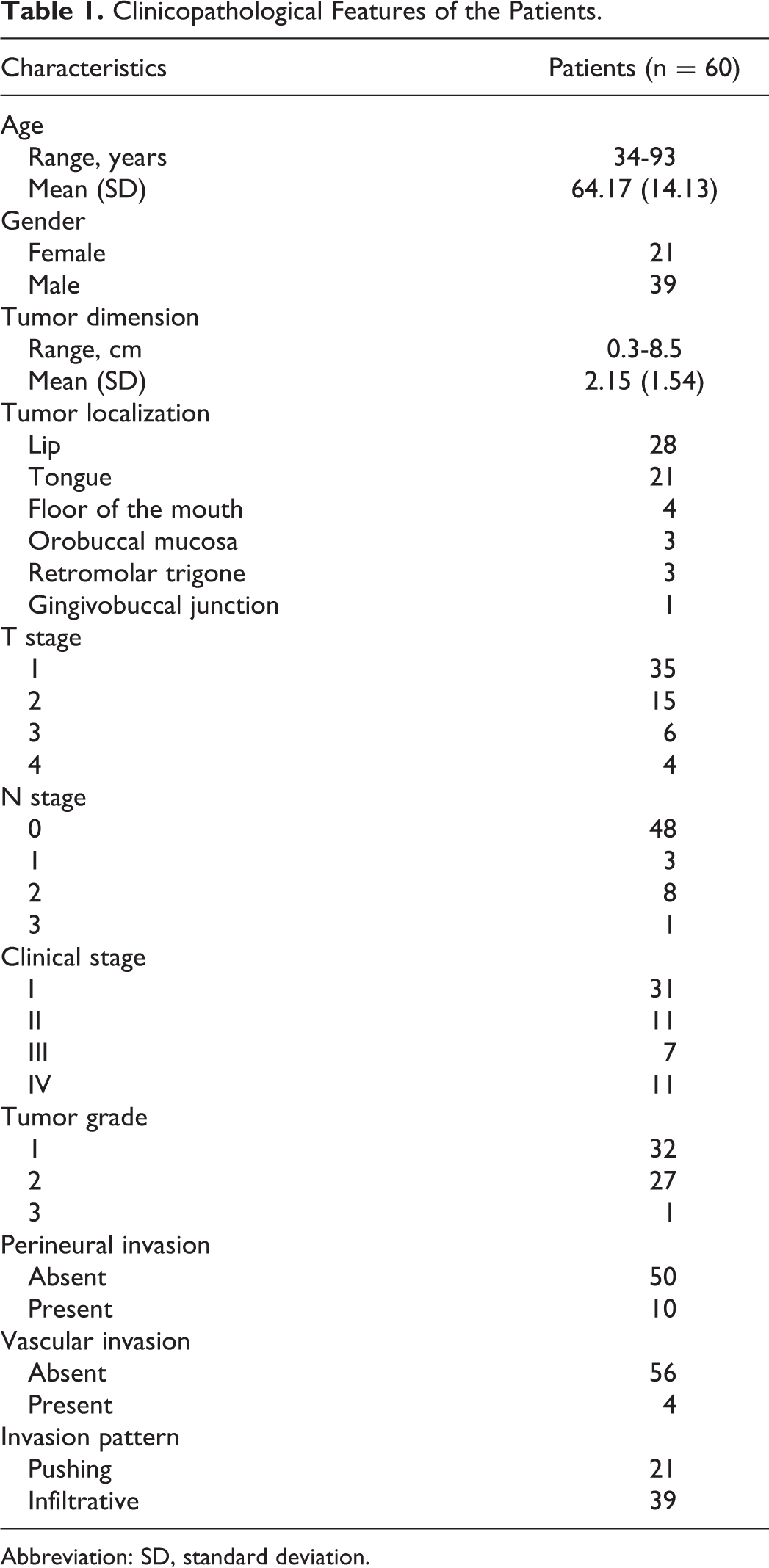
Abbreviation: SD, standard deviation.
Nuclear staining with galectin-3 was observed in 21 (35%) of the cases. No statistically significant association was found between the nuclear staining and clinicopathologic parameters.
Cytoplasmic galectin-3 expression was high in 26 (43.3%) and low in 34 (56.7%) of the cases according to the second evaluation method described in Materials and Methods section. There was no statistically significant relationship between the clinicopathological parameters and the level of cytoplasmic galectin-3 expression.
According to the third evaluation method, the median value of the total expression score (critical expression score) was 1. Cases with an expression score of “0” and “1” were evaluated as “low,” and higher than 1 were evaluated as “high” expression score. High and low expression scores were found in 23 (38.3%) and 37 (61.7%) cases, respectively. High-grade tumors have statistically higher total expression scores than low-grade tumors (P = .011). Also, tumors with infiltrative invasion pattern have higher total expression score than tumors with pushing invasion pattern (P = .002).
Representative examples of the immunohistochemical staining of galectin-3 are shown in Figures 1 and 2. The immunohistochemical staining results of the cases and their association with the clinicopathological parameters are shown in Table 2.
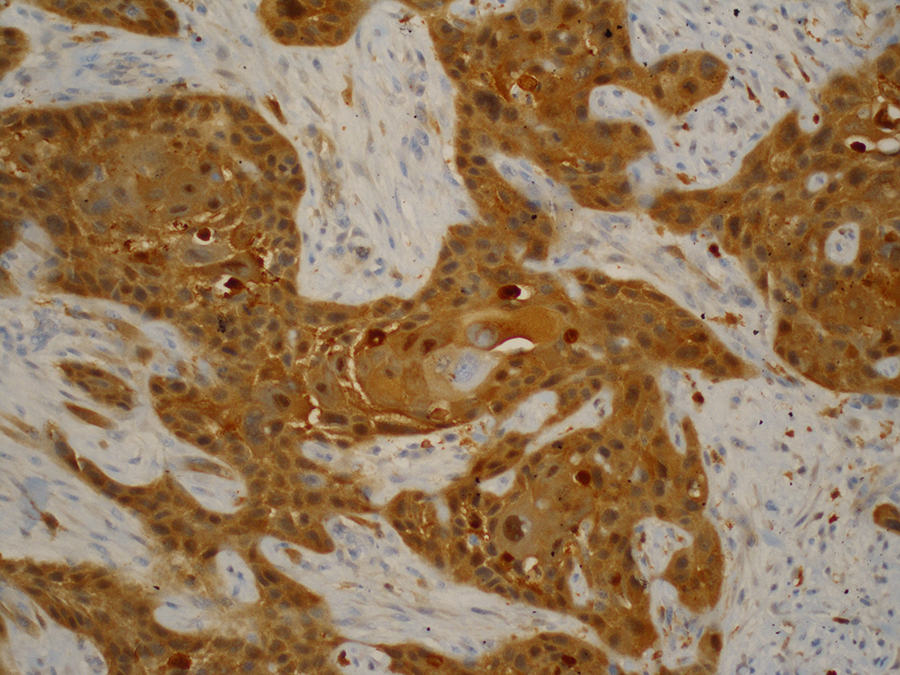
Intense nuclear and cytoplasmic positivity of the tumor (9C4 × 100).
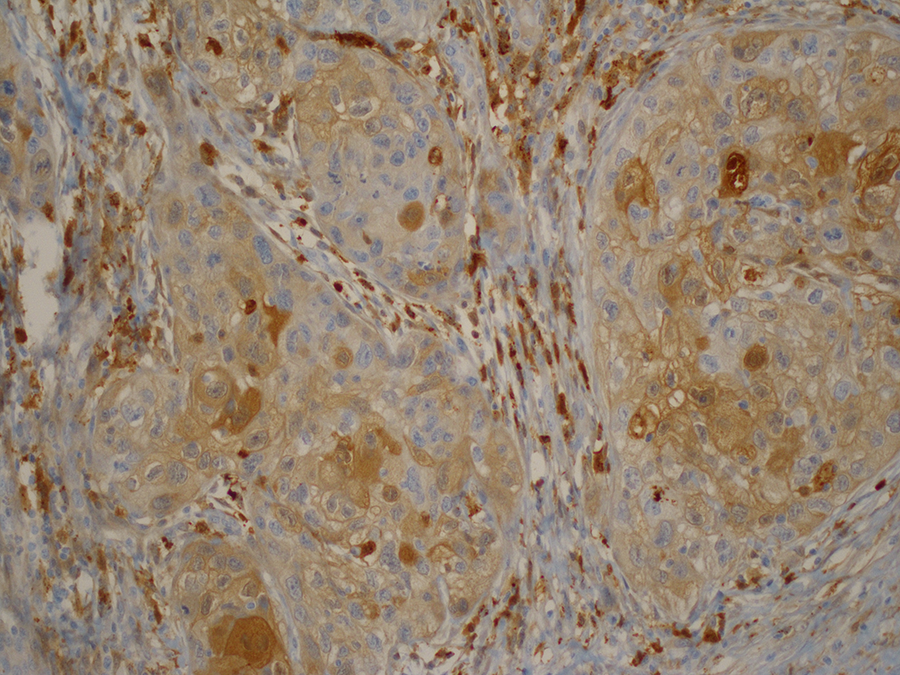
Light cytoplasmic and sparse nuclear staining (9C4 × 100).
Galectin-3 Expression and Clinicopathological Parameters.a
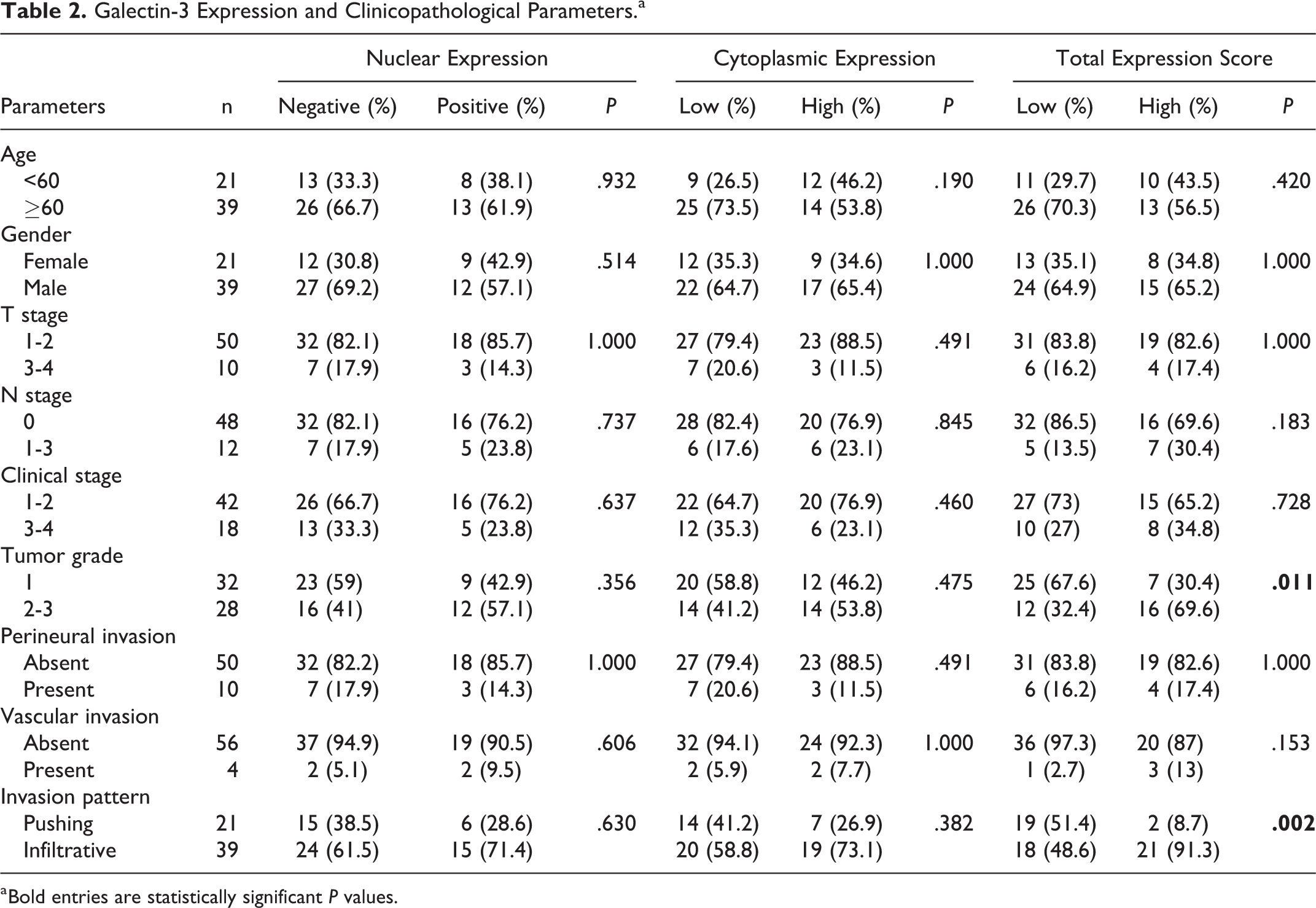
a Bold entries are statistically significant P values.
None of the 3 different assessment methods of galectin-3 expression were associated with survival or recurrence rates. In the multivariate Cox proportional hazard regression (backward stepwise-Wald) analysis, TNM stage, tumor grade, and vascular invasion were found to be of independent significance for death (P < .05; Table 3).
Univariate and Multivariate Cox Proportional Hazard Regression Analysis Results for Death.a
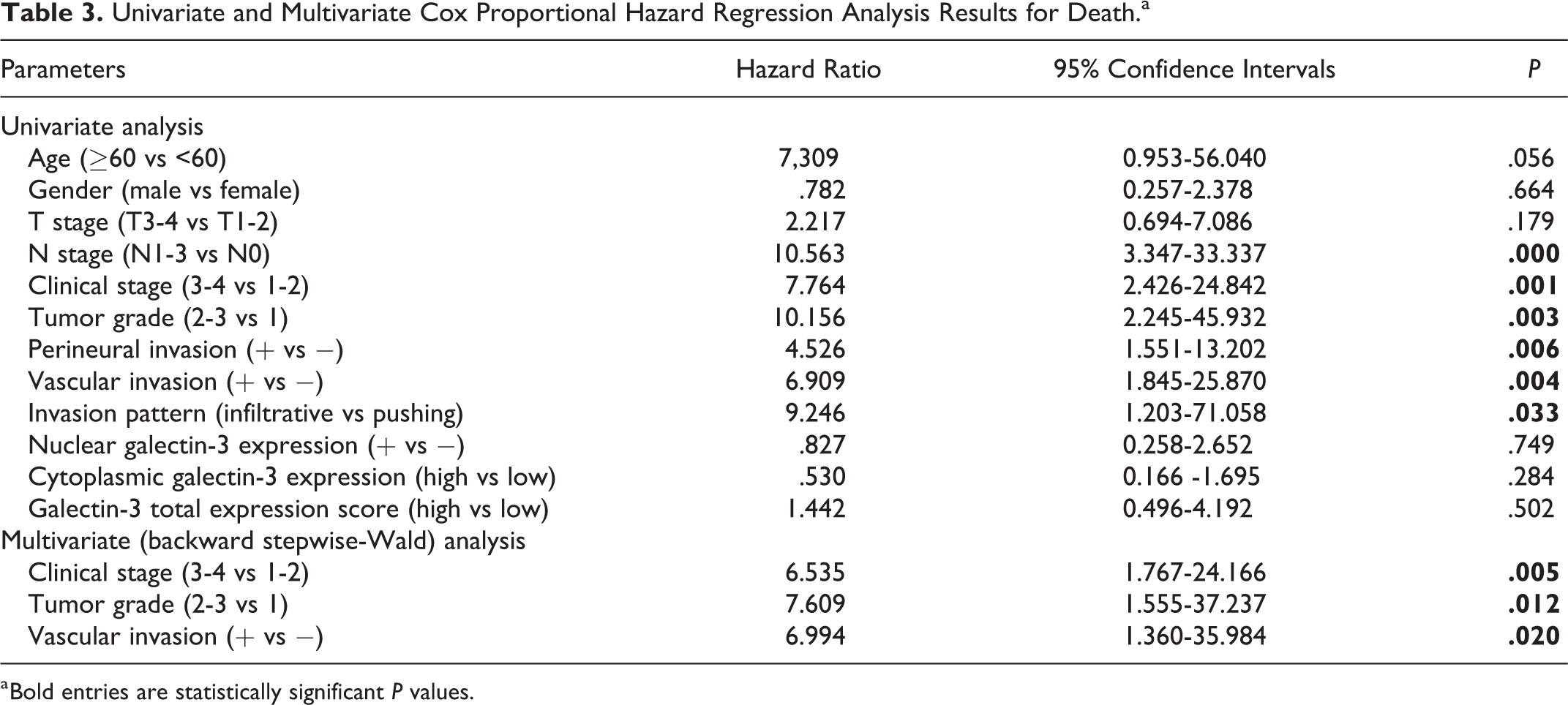
a Bold entries are statistically significant P values.
Discussion
Prediction of prognosis in oral cavity cancers is important in determining optimal treatment. Many factors such as stage, size of the tumor, depth of invasion, invasion pattern, perineural, lymphatic or vascular invasion, surgical margin status, lymphocytic response, microvessel density, and nodal involvement have been demonstrated as potential prognostic determinants. 6,7 However, these factors have limited role in predicting prognosis and determining the treatment modality. With similar clinicopathological features, there are significant differences in the clinical course of patients. New prognostic factors are needed to reliably predict the biological behavior of these tumors.
Recently, the search for molecular biomarkers has accelerated in identifying patients who have high recurrence and mortality risks and therefore may benefit from early aggressive treatments. The prognostic role of galectin-3, one of these determinants, is being investigated in various types of cancer. 6 -9,14 -19 There are few studies in the literature about the prognostic significance of galectin-3 expression in oral squamous cell carcinomas. In these studies, there are conflicting results about the prognostic role of the galectin-3 expression. Alves et al 19 reported a statistically significant relationship between galectin-3 expression and tumor grade and the presence of metastasis in squamous cell carcinoma of the tongue. In this study, galectin-3 expression was also associated with metastasis rate but not with clinical stage. Wang et al 14 demonstrated that galectin-3 expression in squamous cell carcinomas of the tongue strongly correlated with tumor grade, pathological stage, and lymph node involvement. They emphasized that galectin-3 plays an important role in the progression of squamous cell carcinomas of the tongue through activation of the Wnt/β-catenin signaling pathway. In another study, the authors investigated the prognostic significance of galectin-3 expression in patients with advanced head and neck carcinoma and they found a significant relationship between galectin-3 reactivity and histological grade, tumor keratinization, and N stage. 12 However, there was no statistically significant relationship between galectin-3 reactivity and age, primary tumor localization, and T stage or clinical stage. 12 Weber et al 15 reported that high galectin-3 expression correlated with tumor size, lymph vessel infiltration, histological grade, and the presence of lymph node metastasis. The authors emphasized that galectin-3 has a possible tumor-promoting role on oral squamous cell carcinoma. 15 In contrast, in individuals younger than 45 years, galectin-3 expression is not associated with clinical stage or histological malignancy grading systems of oral squamous cell carcinoma. 16 Similarly, Honjo et al 20 did not find any significant correlation between the degree of histological differentiation and cytoplasmic galectin-3 expression in squamous cell carcinomas of the tongue. In this study, no significant relationship was found between cytoplasmic galectin-3 expression and clinicopathological parameters such as age, gender, tumor size, nodal status, and tumor stage. They reported a decrease in the expression of nuclear galectin-3 in the epithelial cells of the tongue from the normal to the cancerous state, while the cytoplasmic expression increased. These findings suggest that galectin-3 promotes tumor progression when it is expressed in the cytoplasm, while the antitumor functions in the nucleus.
In our study, the expression of galectin-3 was evaluated on the basis of nuclear and cytoplasmic staining, separately. And as a third method, total expression score was determined by multiplying the cytoplasmic staining percentage and intensity. Statistically, nuclear galectin-3 staining was not found to be associated with clinicopathological parameters. Similarly, there was no statistically significant relationship between cytoplasmic staining evaluated according to 5% threshold value and clinicopathological features. Differently, total expression score of galectin-3 was found to be significantly higher in high-grade tumors than low-grade ones. Also, tumors with infiltrative invasion pattern have higher expression scores than tumors with pushing invasion pattern. These findings appear to be compatible with the potential role of galectin-3 in the growth and progression of these tumors.
In uni- and multivariate survival analyzes, we found that there is no relationship between galectin-3 expression and recurrence or death in oral squamous cell carcinoma, in all 3 methods of immunohistochemical evaluation. Similarly, Alves et al 19 found no correlation between galectin-3 expression and disease progression in squamous cell carcinomas of the tongue. In another study involving 54 cases of squamous cell carcinomas of the tongue, 20 the investigators identified enhanced expression of cytoplasmic galectin-3 as an independent predictor of disease recurrence. In the high-galectin-3 expression group, the risk of recurrence was found to be 3.514 times higher than in the low-expression group. In our study, multivariate analysis showed that the clinical stage, tumor grade, and vascular invasion were independent prognostic factors in patients with oral squamous cell carcinoma (P < .05).
The main treatment modalities for oral cancers are surgery, radiotherapy, and chemotherapy. Surgery is a common treatment for all stages of oral cancer. Adjuvant radiotherapy with or without chemotherapy is applied after surgical treatment in advanced stage tumors. 21,22 Patients with head and neck cancer are followed-up periodically for at least 5 years after treatment. 23 However, there are many clinicians who follow-up patients for longer periods or even lifelong to detect their final status and possible new primary tumors. 24 The practice of our clinic is to follow up the patients with head and neck cancer as long as possible. Despite the treatment modalities, significant progress has not been achieved in the clinical course of patients with oral cancer. Recently, it has been found that drugs targeting biological molecules can significantly increase the survival of patients with cancer. Galectins have emerged as promising molecular targets for cancer treatment. Galectin inhibitors have the potential to be used as antitumor and antimetastatic agents. By targeting galectin-3 in breast cancer and non-small-cell lung carcinoma, it may increase the efficacy of anticancer drug chemotherapy and reduce the unnecessary treatment exposures and social costs. 25,26 Similarly, drugs targeting galectin-3 can be applied to oral cavity cancers. The contribution of these drugs to standard treatments needs to be demonstrated in larger series with long follow-up.
In conclusion, although galectin-3 total expression score was correlated with the tumor grade and invasion pattern, it is not associated with overall survival or recurrence rates. There are different results in the literature about the relation of galectin-3 expression with prognostic parameters and survival. These different results may be due to different study groups and threshold values with different immunohistochemical methods. For these reasons, there is a need for a large series of cases in which methods are standardized in order to clarify the prognostic role of galectin-3.
Our study has some limitations. First, it was retrospective. Second, our study population was heterogenous. Cancers with different stages arising from the different sites of the oral cavity were included. Further investigations, in a larger scale, aiming to directly investigate the contribution of galectin-3 to the treatment is needed. A scale with the same localization with the same cancer stages may help us to have more reliable information.
Footnotes
Authors’ Note
All authors have been involved in conception, analysis and interpretation of data, and drafting the article. Guarantor for the article is Dr Deniz Arık and he accepts full responsibility for the work. Our study was approved by the Non-Drug Clinical Research Ethics Board of Medicine Faculty of Eskişehir Osmangazi University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.