
Abstract

A full-term male had at birth a lingual cyst protruding from the ventral surface of his tongue into the floor of mouth. It was aspirated at birth with return of 3 ml serous fluid and resolved. It reaccumulated 2 months later, causing posterosuperior protrusion of the tongue and difficulty feeding. A magnetic resonance imaging was performed, demonstrating a cyst within the right tongue musculature extending into the floor of mouth (Figure 1).
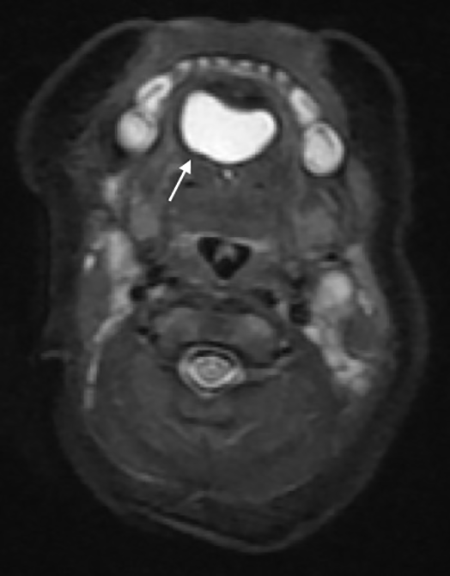
Axial short-TI inversion recovery magnetic resonance imaging demonstrates a cyst (white arrow) within the right tongue extending into the floor of mouth.
The patient underwent intraoral surgical excision, which identified a 3.0 cm × 4.0 cm cystic mass within the right body of the tongue contiguous with the floor of mouth. A tract was noted approaching and abutting the inner table of the midline mandible. The lesion was resected and the tract ligated at the mandible. On follow-up, the patient healed well with no evidence of a palpable mass.
Histologic examination of the original fluctuant pink-tan mass revealed that the largest cyst was lined by a mixture of endodermal epithelia, including respiratory type, cuboidal, and intestinal type with goblet cells. Contrary to this, the adjacent smaller cystic component was lined by keratinizing stratified squamous epithelium associated with underlying adnexal structures, including sebaceous glands and hair follicles, all of ectodermal origin. Scattered displaced aggregates of skeletal muscle were also noted, suggesting a mesodermal component. The presence of all 3 germ cell layers best classifies this as a congenital germline fusion cyst (CGFc)-teratoid variant (Figure 2).
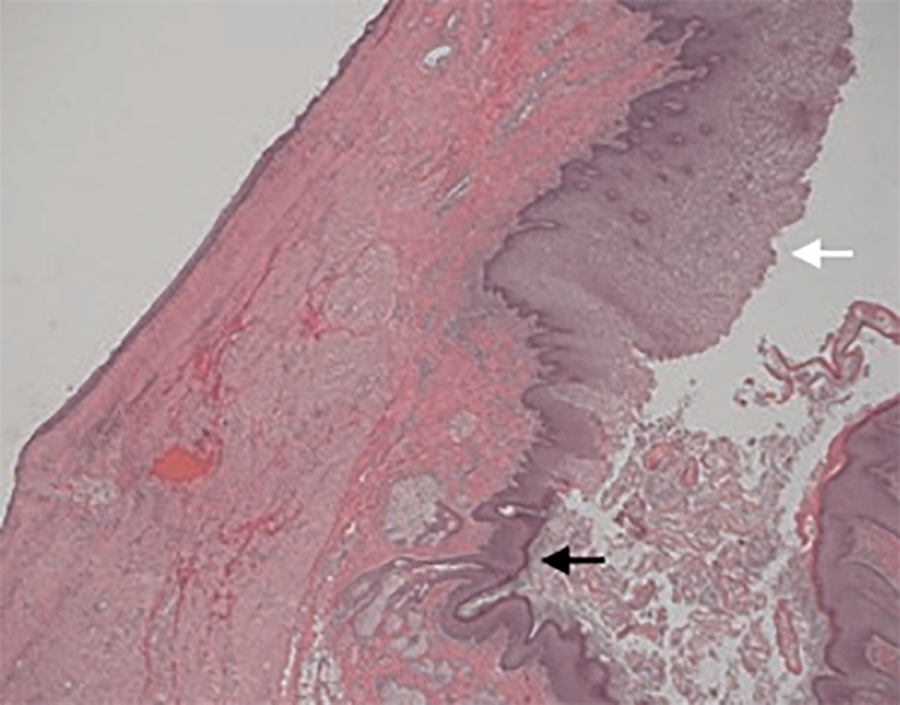
Teratoid cyst pathology is demonstrated by a multiloculated cystic mass lined by both respiratory-type (black arrow) and intestinal-type epithelium (white arrow). Hematoxylin and eosin, low power ×2.
The patient returned 6 months later with a submental abscess requiring antibiotics and multiple incision and drainages. After the infection resolved, the patient underwent surgical excision of the submental mass via circumferential dissection which demonstrated a 1.0 cm × 2.0 cm cystic lesion. A tract was found entering the floor of mouth through the digastric and mylohyoid muscles deep to the mandible. The patient had no further recurrence or infections as of 18 months after the second surgery. Histology of the cystic mass demonstrated monodermal lining of keratinizing stratified squamous epithelium associated with adnexal structures. No other epithelial types were identified, which is consistent with a CGFc-dermoid variant (Figure 3).
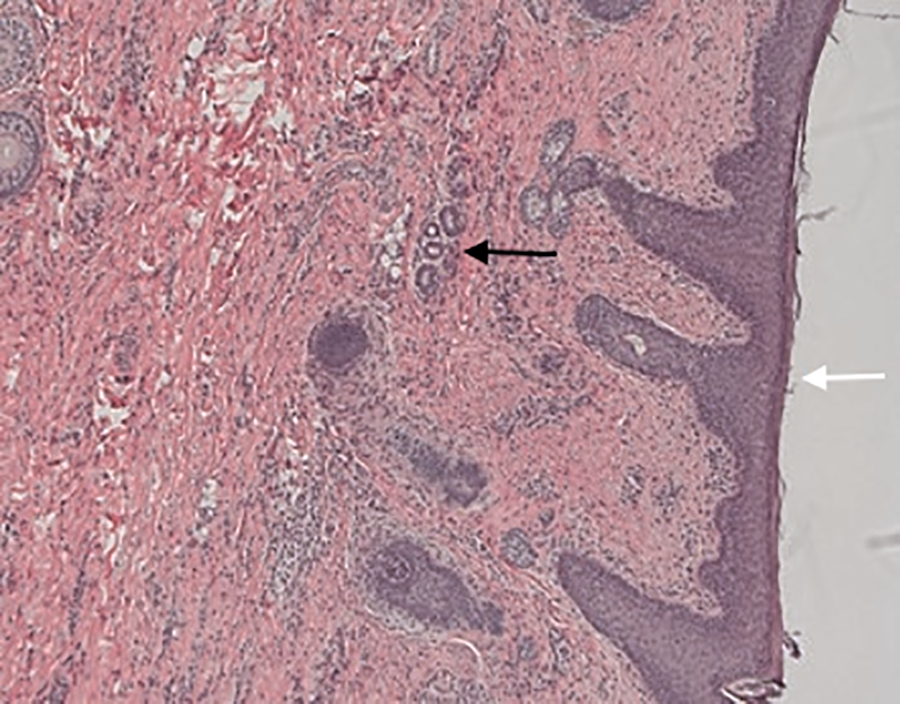
Pathology of the second, recurrent cyst shows keratinized stratified squamous epithelium (white arrow) with adnexal structures (black arrow). Hematoxylin and eosin, high power ×20.
While the pathogenesis is not firmly established, it is hypothesized that these cysts are derived from the epithelial remains from the closure process of the first and second branchial arches. 1,2 Involvement of the tongue is rare, with fewer than 24 cases reported in the literature. 3
Clinically, CGFc presents as a slow-growing, painless, soft, and well-encapsulated mass without lymphadenopathy. 4 They can cause dysphagia, dyspnea, or dysphonia. 5 The majority of teratoid cysts are seen in younger children, with many seen in the first days of life. 6 Magnetic resonance imaging of a teratoid cyst typically depicts a T1-hypointense, T2-hyperintense, well-defined, and lobulated cystic mass with hypoattenuation similar to that of fluid on a computed tomography scan. 7 Magnetic resonance imaging is preferred for floor of mouth cysts, due to its superior soft tissue delineation, and should be included in preoperative assessment.
The majority of cysts can be removed via an intraoral midline sagittal glossotomy approach. 3,8 King demonstrated that the majority (58%) of cases are removed intraorally, with 31% removed extraorally and 11% removed utilizing both approaches. 4 The approach for resection depends on the location and size of the cysts, with large or multiple cysts requiring both intraoral and extraoral incisions. 5 Nasotracheal intubation is recommended as it provides a clearer operative field and is useful in the small oral cavity of the pediatric population. 9 There are generally low recurrence and infection rates when removed either transorally or transcervically 9 ; however, complications include infection, cyst wall disruption resulting in foreign body giant cell reaction, difficulties with articulation, mastication, deglutition, and airway compromise. 10 To prevent recurrence, all tracts and adhesions must be dissected and ligated. 4,5
To our knowledge, there are no other reported cases of a CGFc-teratoid variant recurring as a CGFc-dermoid variant. The teratoid variant is lined by stratified squamous epithelium and partly by gastric or intestinal mucosa, 6 while the dermoid variant is lined with stratified squamous epithelium that contains skin appendages and dermal adnexa such as hair, sweat glands, and sebaceous glands. We hypothesize that the tract extending from the initial teratoid variant contained only epithelium and adnexal structures; resecting the gastric or intestinal mucosa from the initial cyst allowed it to recur as the dermoid variant. However, it is possible that the patient was born with 2 distinct germline fusion cysts as the differing pathology suggests. Cases of multiple cysts in the floor of mouth have also been reported in the literature. 4
Footnotes
Authors’ Note
Presented at the Triological Society Combined Sections Meeting, Scottsdale, AZ, January 18-20, 2018.
Acknowledgments
The authors would like to thank the Department of Otolaryngology at the New York University School of Medicine for their support in the publication of this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.