
Abstract
Objective:
The objective is to reduce the rates of misdiagnosis and inappropriate treatment of laryngeal tuberculosis (LTB).
Study Design:
Retrospective case series.
Materials and Methods:
Medical records of 3 histopathology-confirmed cases at a tertiary medical center from 2000 to 2018.
Results:
Seventeen patients with LTB included in this study. Of the 17 patients, 16 patients were male and 1 was female; 11 patients had a history of smoking. Odynophagia was the chief complaint in 6 cases, and 11 patients complained of hoarseness. The appearance of the affected larynx was ranged from diffuse swelling (n = 7, 41.2%), mucosa white lesion (n = 5,29.4%), and granulomatous tumors (n = 2, 11.76%), and these features presented together (n = 2, 11.76%). Seventeen patients with LTB were misdiagnosed as acute epiglottitis in 4 (23.5%) patients, acute laryngitis in 1 (5.9%) patient, leukoplakia in 5 (29.4%) patients, laryngopharyngeal reflux (LPR) in 6 (35.3%) patients, and laryngocarcinoma in 1 (5.9%) patient. Chest computed tomography reported old pulmonary tuberculosis in 2 (11.7%) patients, active pulmonary tuberculosis in 7 (41.2%) patients, and normal lung status in 8 (47.1%) patients. Histopathological examination reported Mycobacterium tuberculosis infection by revealing epithelioid cell granulomas with Langhans-type giant cells in 14 (82.4%) patients and epithelioid cell granulomas with caseous necrosis and Langhans-type giant cells in 3 (17.6%) patients.
Conclusions:
Laryngeal tuberculosis was easily misdiagnosed as acute epiglottitis or leukoplakia because of diffuse swelling of the epiglottis or white lesions over the true vocal cord, especially patients with increasing LTB were misdiagnosed as LPR with the enhancement of LPR awareness among otolaryngologist. Clinicians should be aware of the possibility of LTB for chronic intractable laryngitis with failure treatment of proton pump inhibitor and recurrent acute epiglottitis with foreign body injury.
Introduction
Laryngeal tuberculosis (LTB) is rarely suspected in recent years. However, sporadic cases of LTB still occur in outpatient clinics. In addition, the clinical manifestations of LTB have changed due to the extensive use of antibiotics and corticosteroids. 1 -3 Previously, the most frequent chief complaint of LTB was odynophagia accompanied by systemic symptoms such as fever, weight loss, and night sweats, as well as ulceration of the larynx. However, the most frequent chief complaint of LTB is currently hoarseness, and the most common lesion site is the true vocal cords. The most frequent lesions are edema and hyperplastic lesions. 1 -5 Laryngeal tuberculosis is frequently misdiagnosed because it manifests nontypical symptoms and signs. 6 -9 Some patients with LTB were misdiagnosed as laryngopharyngeal reflux (LPR) with the enhancement of LPR awareness among otolaryngologist. In this study, we propose to show the value of considering the possibility of this disease in the presence of varied clinical and laryngoscopy features.
Materials and Methods
The study was approved by the institutional review board of Yiwu Central Hospital. Informed consent was obtained from the 17 patients.
The records of all patients admitted to our institution between February 2000 and November 2018 with the diagnosis of LTB were reviewed and 17 cases were identified. The evaluation of the patients consisted of a thorough history and videostroboscopy examination, chest computed tomography (CT), laryngeal CT or magnetic resonance imaging (MRI), sputum culture, purified protein derivative (PPD) testing, biopsy, routine blood, and HIV serum testing. The diagnosis of LTB was based on the histological examination and Ziehl-Neelsen staining. The criterion for diagnosis was the presence of acid–fast bacilli in biopsy specimens or the histopathologic change of well-defined, confluent, epithelioid cell granulomas with or without caseous necrosis and response to antituberculosis therapy.
Results
The patients ranged in age from 42 to 68 years, with an average of 51.11 ± 17.23 years. There were 16 males and 1 female in this study. Three patients had hyperglycemia (17.6%), 2 patients (11.76%) had previous pulmonary tuberculosis history, 11 patients (64.7%) in this series had a history of smoking, and only 2 (11.8%) patients had a cough, fever, weight loss, chills, night sweats, hemoptysis, or other chest symptoms in this study. Thirteen patients received antibiotic and corticosteroids treatment, atomization inhalation, and traditional Chinese medicine therapy, while 4 patients received rabeprazole in clinic prior to definitive diagnosis.
Of the 17 patients, odynophagia was the chief complaint in 6 cases, and 11 patients complained of hoarseness. Of the 6 patients with odynophagia, 2 patients had the history of fishbone injury in the throat. The duration of symptoms ranged from 1 to 7 months, with an average of 2.39 ± 1.81 months.
The appearance of the affected larynx in laryngoscopy was variable and ranged from diffuse swelling (n = 7, 41.2%), mucosa white lesion (n = 5, 29.4%; Figure 1), and granulomatous lesion (n = 2, 11.76%), and these features presented together (n = 2, 11.76%). Fourteen patients (82.4%) had a single lesion involving only one subsite of the airway at first hospital visit. The order of frequency was true vocal fold (n = 9, 64.3%), epiglottis (n = 4, 28.6%), and false vocal fold (n = 1, 7.1%). The other 3 patients (17.6%) had lesions involving more than one subsite of the airway; the number of subsites involved ranged from 2 to 3, mainly involving the true vocal fold (3/3,100%), epiglottis (2/3, 66.7%), false vocal fold (n = 1/3, 7.1%), and arytenoid cartilage (n = 1/3, 7.1%). All the patients were misdiagnosed at first hospital visit. Seventeen patients with LTB were misdiagnosed as acute epiglottitis in 4 (23.5%) patients, acute laryngitis in 1 (5.9%) patient, leukoplakia in 5 (29.4%) patients, LPR in 6 (35.3%) patients, and laryngocarcinoma in 1 (5.9%) patient.
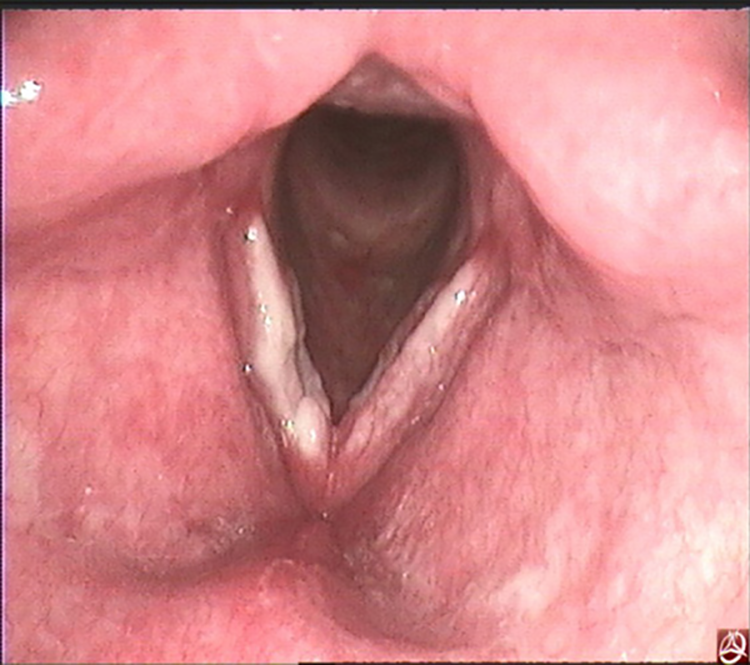
Video laryngoscope revealed white lesions over the bilateral thickening true vocal fold before treatment.
Chest CT reported old pulmonary tuberculosis in 2 (11.7%) patients, active pulmonary tuberculosis in 7 (41.2%) patients (Figure 2), and normal lung status in 8 (47.1%) patients. Laryngeal CT or MRI reported the focal regular thickening and rough surface without bone destruction in 17 patients (Figure 3).
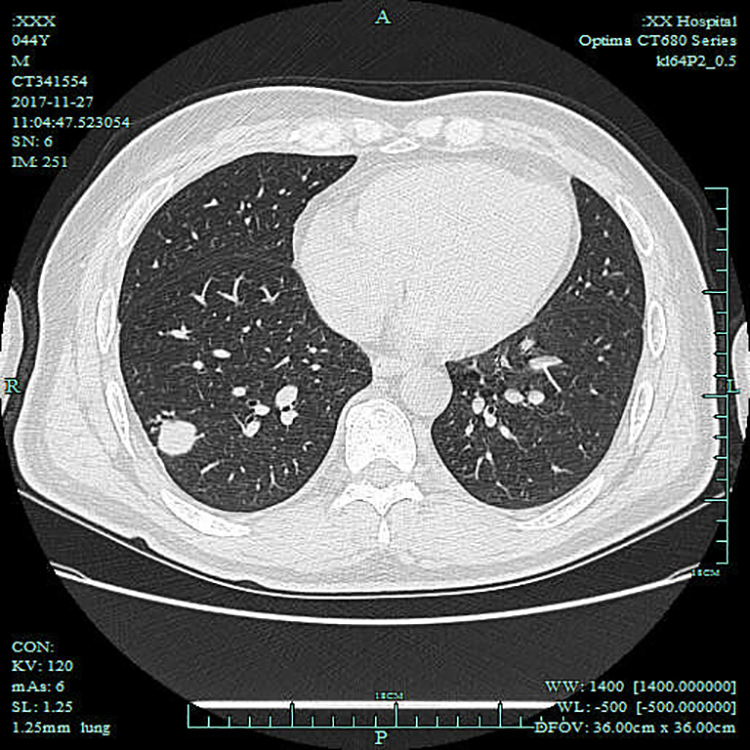
Chest computed tomography found mass under the pleural membrane in the inferior lobe of the right lung, with surrounding satellite lesions before treatment.

Laryngeal magnetic resonance imaging found regular thickening and rough surface of bilateral vocal fold with intermediate signal intensity in coronal scan CE-FS-T1WI.
Only 3 (17.6%) patients had positive PPD tests in this study. Results of the sputum culture were available for 15 patients, all of whom showed positive results. Biopsy was performed under general anesthesia in all the patients. All the patients had negative HIV serum testing. Histopathological examination reported M tuberculosis infection by revealing epithelioid cell granulomas with Langhans-type giant cells in 14 (82.4%) patients (Figure 4) and epithelioid cell granulomas with caseous necrosis and Langhans-type giant cells in 3 (17.6%) patients. Six patients (35.3%) showed positive tuberculosis bacilli and 11 (64.7%) patients showed negative tuberculosis bacilli in acid–fast stain. Twelve patients had available sputum culture record, and 9 patients (75.0%) showed positive result.
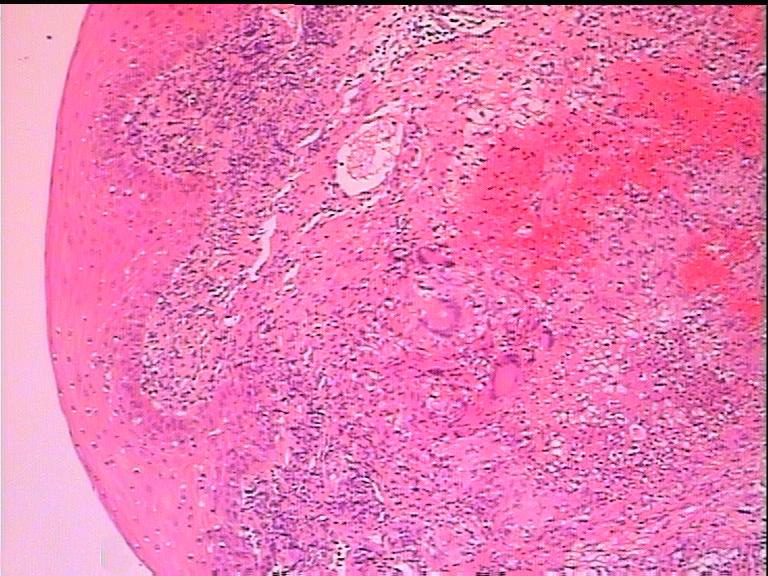
Histopathological examination confirmed Mycobacterium tuberculosis infection by showing epithelioid cell granulomas and granulomas with Langhans-type giant cells.
All the patients were referred to the Communicable Diseases Department in our hospital and received the free treatment of 3 combinations of isoniazid, rifampin, and ethambutol for 9 to 12 months. Only 11 (64.7%) patients had recorded results for antituberculosis treatment. They usually had good response to chemotherapy; the lesions and symptoms improved within 3 months and completely recovered within 9 months of treatment (Figure 5).
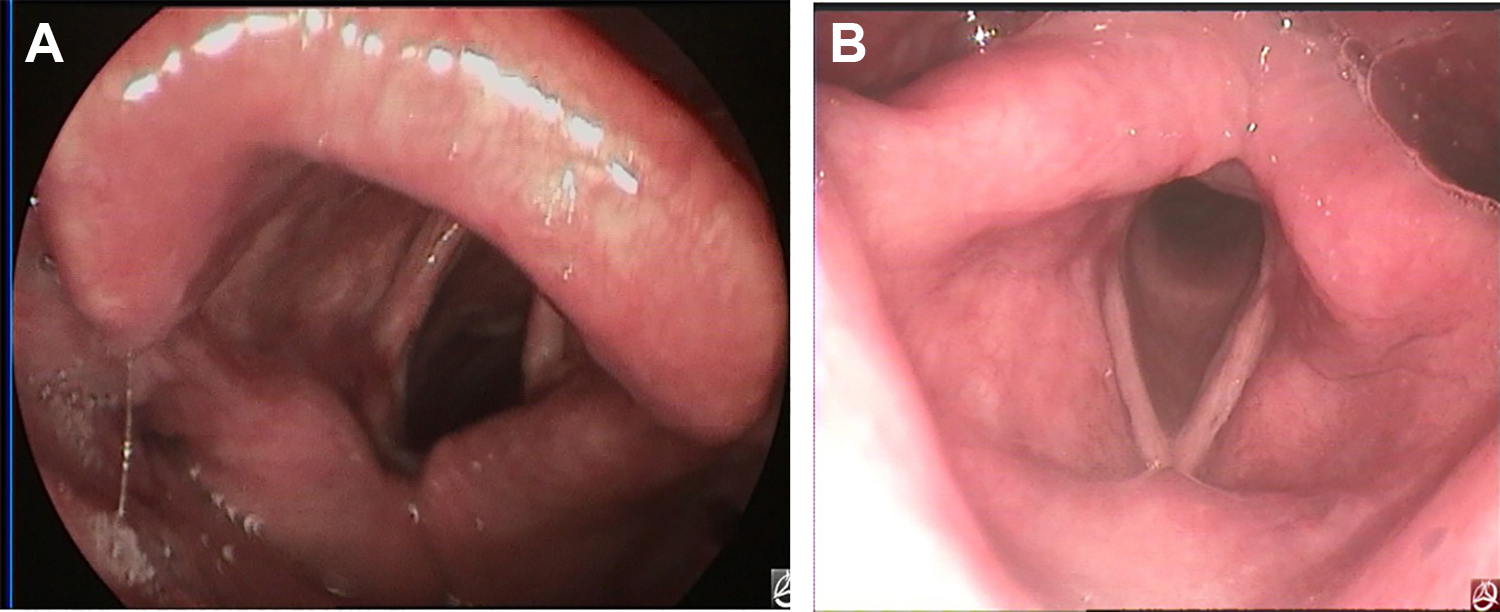
Video laryngoscope revealed white lesions nearly disappeared and the true vocal fold was close to normal morphology at 3 months after treatment (A) and the true vocal fold completely recovered normal at 9 months after treatment (B).
Discussion
Laryngeal tuberculosis is increasingly rare in China, while sporadic cases of LTB occur in outpatient clinics. The age of onset of LTB was typically 20 to 30 years prior to the 1980s, 10 but in the 1990s and after, the age of onset has been 40 to 60 years, 11,12 in agreement with our cases. Some scholars 13 reported that smoking is the risk factor associated with the LTB 13,14 ; 64.7% of patients had a history of smoking in this study. Kurokawa et al 14 showed that 52.9% of patients with LTB had a history of smoking. In addition, most of the patients with LTB had systemic symptoms such as a cough, fever, weight loss, and night sweats in the past, 3,6,9,14 -16 and only 2 (11.8%) patients had systemic symptoms in this study. In this study, 11(64.7%) patients complained of hoarseness and odynophagia in 6 (35.3%) cases. The larynx showed the diffuse swelling in 41.2% of patients and mucosa white lesion in 29.4% of patients; only 4 patients showed the granulomatous tumors and these features presented together. The most commonly involved site is true vocal fold in 64.3% of patients and epiglottis in 28.6% of patients. Auerbach 10 reported that 92.3% of autopsied cases of LTB had advanced pulmonary tuberculosis. However, only 52.9% patients reported old or active pulmonary tuberculosis by chest CT in this study.
Previous studies suggested that LTB was easily misdiagnosed as acute laryngitis or laryngocarcinoma. 3,6,8 In this study, all the patients were misdiagnosed at first visit, and 5 patients were misdiagnosed at least 3 times because of the application of large-dose corticosteroids; LTB was considered until ulceration of the epiglottis occurred and a biopsy was performed at the third visit because of the history of fishbone injury in 2 patients. It’s worth noting that patients with increasing LTB were misdiagnosed as LPR and leukoplakia with the enhancement of LPR awareness among otolaryngologist and white lesions over the true vocal fold; 64.7% of patients were misdiagnosed as LPR or leukoplakia in this study. Other scholars also reported similar findings. 8 Of the 5 patients with LTB who were misdiagnosed as leukoplakia, 3 patients with normal chest CT were definitely diagnosed after partial vocal mucosa stripping surgery. However, only 1 patient was considered as laryngocarcinoma because laryngeal CT or MRI was performed in all patients.
Some routine examinations should be performed for the diagnosis and excluding of LTB, such as chest CT, sputum smear, sputum culture, biopsy, and acid–fast bacilli and PPD tests. 13,16 The definitive diagnosis of LTB was dependent on the presence of an epithelioid granuloma with Langhans-type giant cells, granulomatous inflammation, and caseating granulomas in the histological examination. However, previous studies showed that caseating granulomas were absent in most of patients with LTB. 2,17 El Ayoubi et al 2 by histology found a giant cell granuloma in 100% of cases of LTB and caseous necrosis in 20%. Only 17.6% patients had the presence of caseous necrosis in this study. Also, acid–fast bacilli are not found in most of patients because of abuse of corticosteroids and antibiotics. 6 Only 6 patients (35.3%) showed positive tuberculosis bacilli and 11 (64.7%) patients negative tuberculosis bacilli in acid–fast stain. Thus, LTB should be considered if granulomas with Langhans-type giant cells are identified. In addition, clinicians should be aware of the possibility of LTB for chronic intractable laryngitis with failure treatment of proton pump inhibitor and recurrent acute epiglottitis with foreign body injury. Diagnostic antituberculosis therapy may be administered to patients with no definitive diagnosis but who are highly suspected to have LTB. An organized diagnostic algorithm is summarized in Figure 6 in this study. The LTB should be suspected when laryngeal symptoms and signs didn’t significantly improve for 1 to 2 weeks by routine medicine treatment. The chest CT may be first recommended because the imaging result was quickly reported by radiologist. Sputum culture and PPD testing were performed if screening was negative along with high suspicion. However, tissue biopsy was required to make a diagnosis of LTB in all the patients. In addition, the epidemiological situation of tuberculosis is regionally diverse and dynamically changing. The actions taken by the World Health Organization (WHO) since the 90s have been effective, and from 2005, a decrease in the prevalence has been noted and even earlier a decrease in mortality was observed. The highest number of tuberculosis cases are observed in Southeast Asia, and the highest incidence index is in sub-Saharan Africa 18 However, WHO publishes Global Tuberculosis Report which showed that two-third of tuberculosis cases around the world were from India (27%), China (9%), Indonesia (8%), Philippines (6%), Pakistan (5%), Nigeria (4%), Bangladesh (4%), and South Africa (3%). 19 Thus, these countries of high prevalence of tuberculosis around the world are more likely to encounter this diagnosis of LTB, and physicians must keep LTB in their differential diagnosis list.
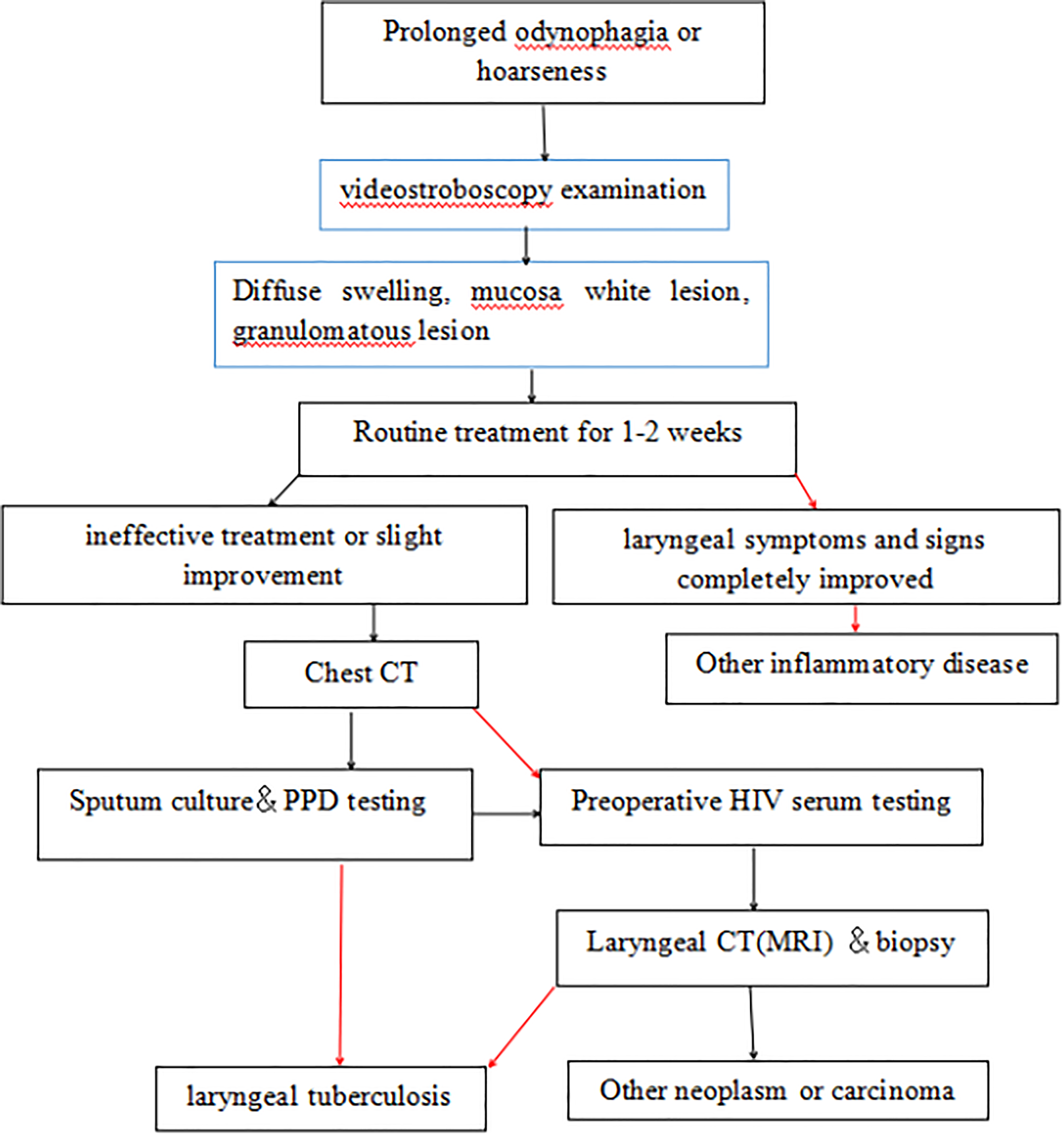
The diagnostic algorithm of laryngeal tuberculosis. Red arrow: positive findings; black arrow: negative findings.
Conclusion
Patients with LTB were easily misdiagnosed as acute epiglottitis or leukoplakia because of diffuse swelling of epiglottis or white lesions over the true vocal fold. In addition, patients with increasing LTB were misdiagnosed as LPR with the enhancement of LPR awareness among otolaryngologist. Clinicians should be aware of the possibility of LTB for chronic intractable laryngitis with failure treatment of proton pump inhibitor and recurrent acute epiglottitis with foreign body injury.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.