
Abstract
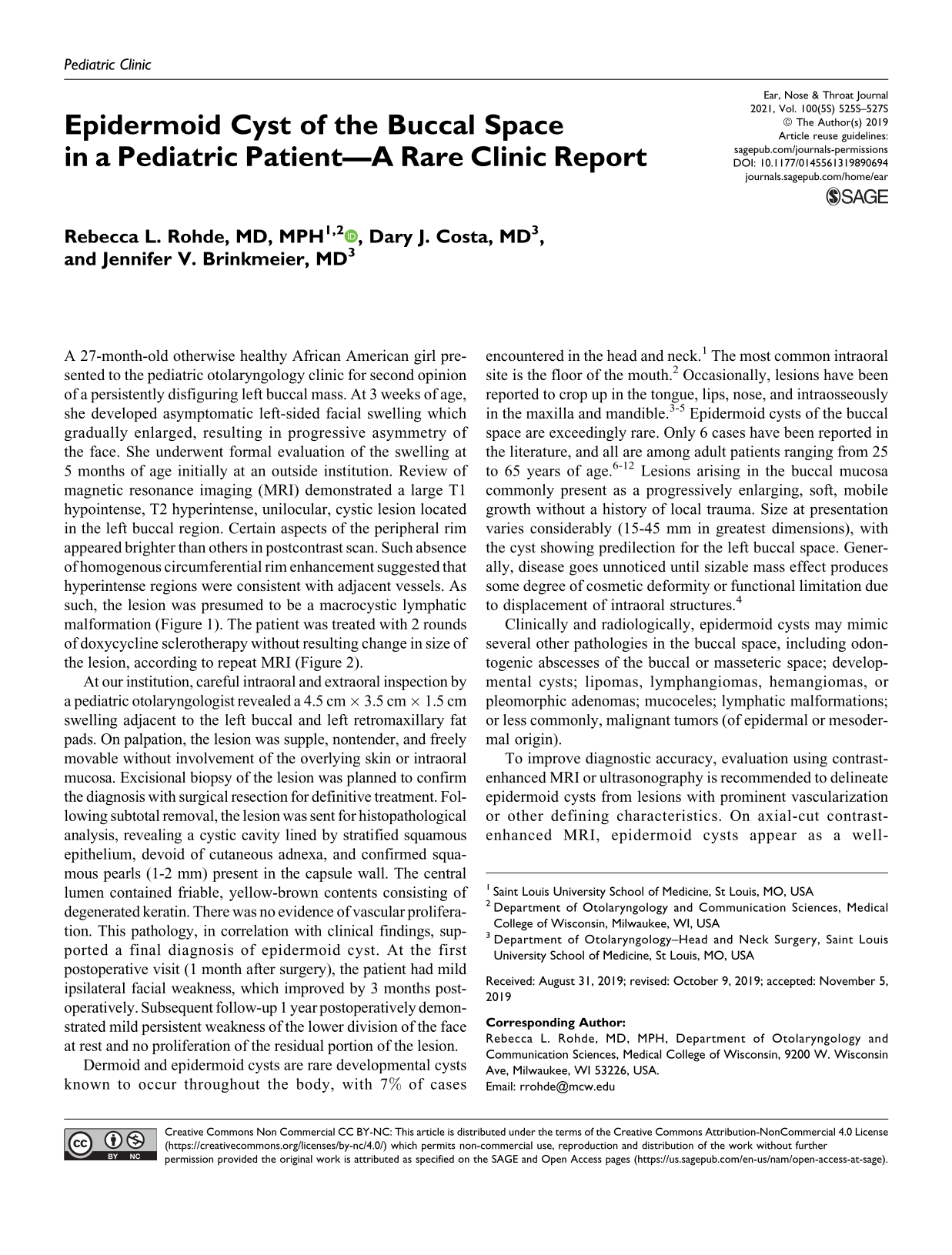
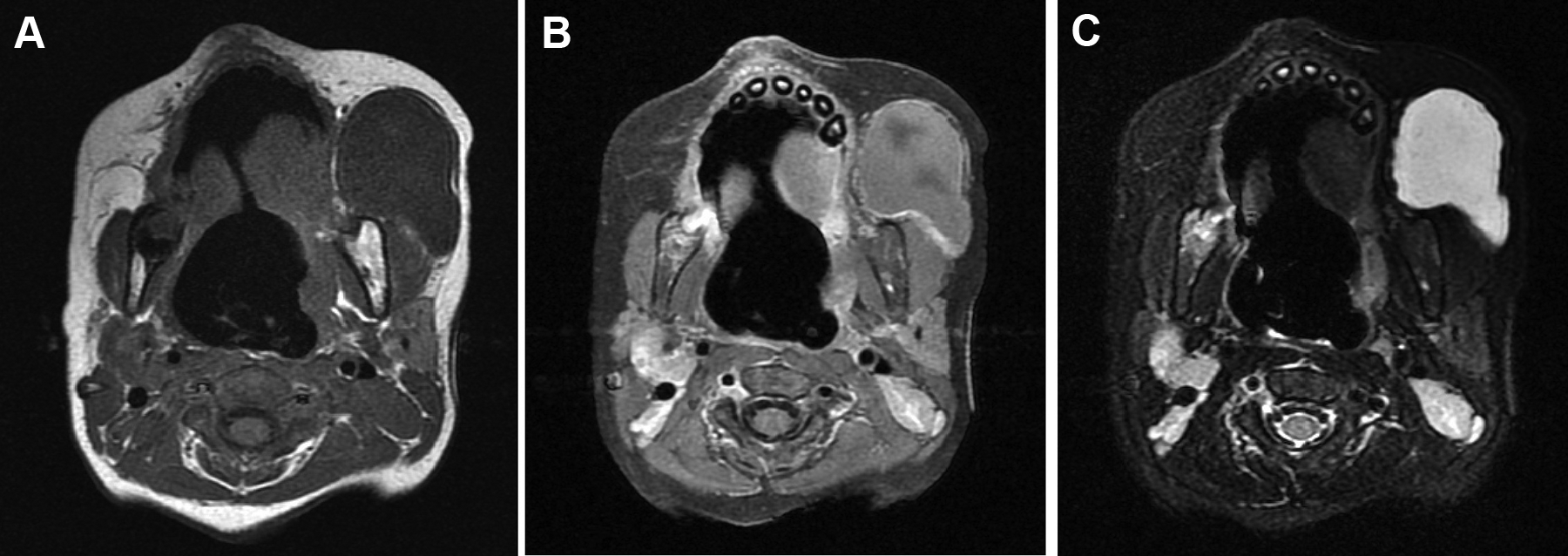
A 27-month-old otherwise healthy African American girl presented to the pediatric otolaryngology clinic for second opinion of a persistently disfiguring left buccal mass. At 3 weeks of age, she developed asymptomatic left-sided facial swelling which gradually enlarged, resulting in progressive asymmetry of the face. She underwent formal evaluation of the swelling at 5 months of age initially at an outside institution. Review of magnetic resonance imaging (MRI) demonstrated a large T1 hypointense, T2 hyperintense, unilocular, cystic lesion located in the left buccal region. Certain aspects of the peripheral rim appeared brighter than others in postcontrast scan. Such absence of homogenous circumferential rim enhancement suggested that hyperintense regions were consistent with adjacent vessels. As such, the lesion was presumed to be a macrocystic lymphatic malformation (Figure 1). The patient was treated with 2 rounds of doxycycline sclerotherapy without resulting change in size of the lesion, according to repeat MRI (Figure 2).
Mass in buccal space shown on axial magnetic resonance imaging before sclerotherapy. (A) Axial T1, (B) Axial T1 postcontrast, and (C) Axial T2.
Mass in buccal space on magnetic resonance imaging after sclerotherapy. (A) Axial T1 and (B) Axial T1 postcontrast.
At our institution, careful intraoral and extraoral inspection by a pediatric otolaryngologist revealed a 4.5 cm × 3.5 cm × 1.5 cm swelling adjacent to the left buccal and left retromaxillary fat pads. On palpation, the lesion was supple, nontender, and freely movable without involvement of the overlying skin or intraoral mucosa. Excisional biopsy of the lesion was planned to confirm the diagnosis with surgical resection for definitive treatment. Following subtotal removal, the lesion was sent for histopathological analysis, revealing a cystic cavity lined by stratified squamous epithelium, devoid of cutaneous adnexa, and confirmed squamous pearls (1-2 mm) present in the capsule wall. The central lumen contained friable, yellow-brown contents consisting of degenerated keratin. There was no evidence of vascular proliferation. This pathology, in correlation with clinical findings, supported a final diagnosis of epidermoid cyst. At the first postoperative visit (1 month after surgery), the patient had mild ipsilateral facial weakness, which improved by 3 months postoperatively. Subsequent follow-up 1 year postoperatively demonstrated mild persistent weakness of the lower division of the face at rest and no proliferation of the residual portion of the lesion.
Dermoid and epidermoid cysts are rare developmental cysts known to occur throughout the body, with 7% of cases encountered in the head and neck. 1 The most common intraoral site is the floor of the mouth. 2 Occasionally, lesions have been reported to crop up in the tongue, lips, nose, and intraosseously in the maxilla and mandible. 3 -5 Epidermoid cysts of the buccal space are exceedingly rare. Only 6 cases have been reported in the literature, and all are among adult patients ranging from 25 to 65 years of age. 6 -12 Lesions arising in the buccal mucosa commonly present as a progressively enlarging, soft, mobile growth without a history of local trauma. Size at presentation varies considerably (15-45 mm in greatest dimensions), with the cyst showing predilection for the left buccal space. Generally, disease goes unnoticed until sizable mass effect produces some degree of cosmetic deformity or functional limitation due to displacement of intraoral structures. 4
Clinically and radiologically, epidermoid cysts may mimic several other pathologies in the buccal space, including odontogenic abscesses of the buccal or masseteric space; developmental cysts; lipomas, lymphangiomas, hemangiomas, or pleomorphic adenomas; mucoceles; lymphatic malformations; or less commonly, malignant tumors (of epidermal or mesodermal origin).
To improve diagnostic accuracy, evaluation using contrast-enhanced MRI or ultrasonography is recommended to delineate epidermoid cysts from lesions with prominent vascularization or other defining characteristics. On axial-cut contrast-enhanced MRI, epidermoid cysts appear as a well-circumscribed mass with low signal intensity in T1-weighted images and high signal intensity in T2-weighted images, similar to many other lesions. 13 Ultrasonography reveals a well-demarcated capsule with a heterogeneous interior due to the presence of keratinized fluid. 14 Thorough review of all imaging planes may be indicated for preoperative planning to determine the extent of the lesion and to facilitate visualization of its relationship to surrounding structures.
A definitive diagnosis is achieved by histopathologic analysis. 13,15 As in this case, the patient’s prior sclerotherapy treatment had complicated interpretation of her posttreatment MRI, and thus, histopathology was required to obtain an accurate preliminary diagnosis. Initial assessment of pathology is important to determine appropriate treatment modality, which is likely adapted to each clinical case. 16,17 If an epidermoid cyst is suspected, incisional or aspiration biopsy may be useful to guide method of intervention.
In general, epidermoid cysts do not undergo malignant transformation. 18 For lesions that are smaller or asymptomatic, watchful waiting may be considered. Total resection usually results in resolution of symptoms without anticipated recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.