
Abstract
Sinonasal inverted papilloma (IP) is the most common benign epithelial tumor in the nasal cavity and paranasal sinuses, with a worldwide incidence between 0.6 and 1.5/100 000 persons per year. However, only a few studies have investigated patient-dependent factors related to IP recurrence and persistence. According to available evidence, these factors are still debated, and results are contradictory. In this multicenter retrospective study, we analyzed the clinical records of 130 patients who were surgically treated for sinonasal IP to evaluate the factors affecting recurrence and persistence of IP and compared the curative rates of different surgical approaches. Our analysis showed that IP recurrence is strongly related to specific risk factors including incomplete surgical removal, stage of disease, site of the lesion, surgical technique, and malignancy rate. In conclusion, the recurrence of IP may be affected by several risk factors; these factors must be carefully considered during clinical evaluation and especially during the follow-up of patients with IP.
Introduction
Sinonasal inverted papilloma (IP), first described in 1854, is a benign epithelial lesion of the nasal cavity and paranasal sinuses; its incidence ranges between 0.6 and 1.5/100 000 persons per year. 1 -4 IP mainly occurs in adults during the fifth decade of life, with a higher prevalence in males (male to female ratio: 7:1) 5 and in the Caucasian race. 6,7 IP is the most common histological type of nasal papilloma, followed by oncocytic papilloma and fungiform papilloma. 8 IP arises in the Schneiderian epithelium of the nasal cavity and paranasal sinuses, primarily from the lateral nasal wall, and is generally unilateral. 1 -4 Three characteristics make IP different from other sinonasal tumors: the high recurrence rate (up to 70%), strong potential for local bone erosion, and risk of malignant transformation (5%-13%). 3 Etiology of IP remains mostly unknown; an association with human papilloma virus (HPV), especially HPV types 6, 11, 16, and 18, has been reported in up to 40% of cases 9 , but the literature remains contradictory. 10,11 Clinical nonspecific symptoms of IP may include unilateral occlusion, rhinorrhea, sinus infection, and hyposmia/anosmia. Such primary manifestations may be accompanied by headaches and facial pain/pressure, lacrimation, or impaired vision. 5 Endoscopically, the lesion appears as a grayish polypoid mass with a multinodular surface. 3 The treatment of choice is surgical; a purely endoscopic endonasal approach or combined endoscopic and external approach has now become the gold standard for many authors. 12 -17 Chemotherapy and/or radiation therapy may follow surgery in case of malignant transformation; many authors have suggested that radiotherapy could be used for patients whose tumor has not been completely resected or in case of multiple recurrences. 18,19
Several factors with a potential role in the recurrence or persistence of IP have been described, including cigarette smoke, allergy, certain occupational exposures, demographic factors, histology, lesion side, stage, and surgical approach; however, their role is still controversial and a specific cause has yet to be confirmed. 11 The aim of this multicenter retrospective study is to analyze the factors affecting the recurrence and persistence of sinonasal IP.
Patients and Methods
One-hundred thirty patients diagnosed with sinonasal IP at the Policlinico Umberto I of Rome and Ospedale Niguarda “Ca Granda” of Milan, Italy, from December 2004 to January 2016, were included in the study.
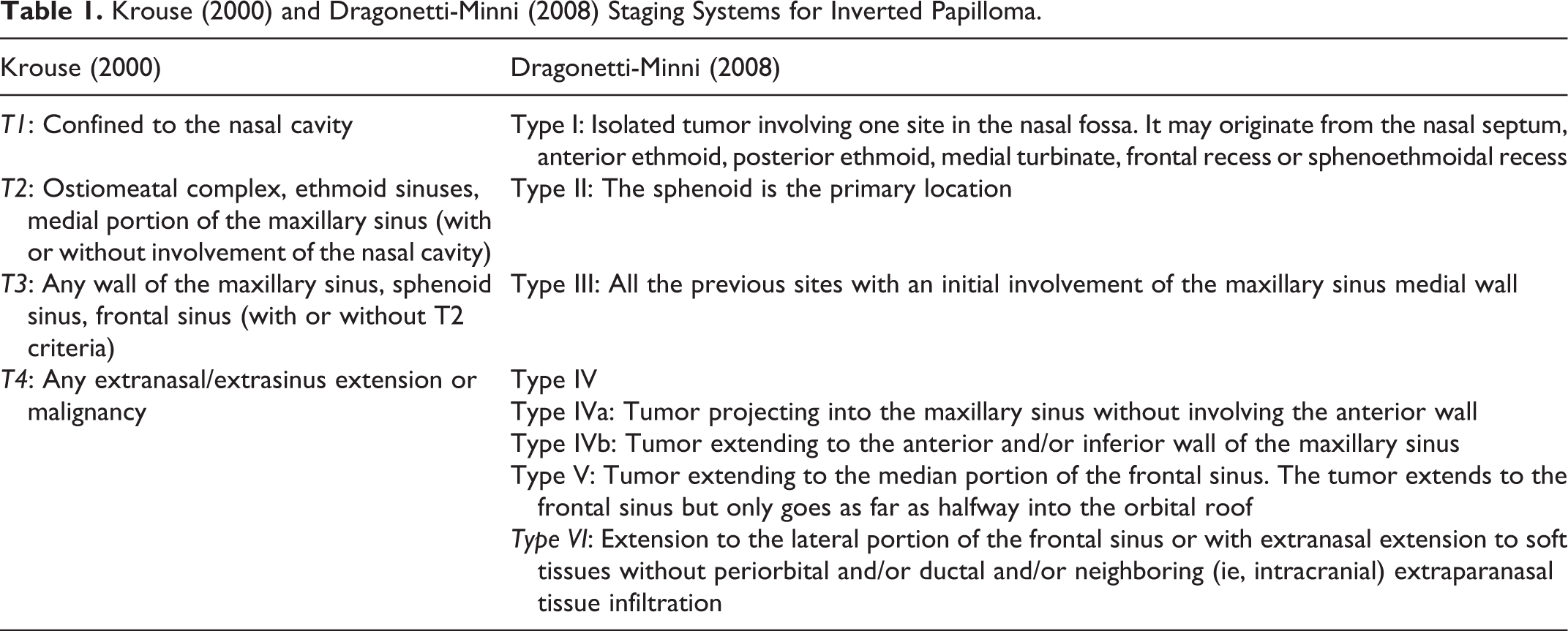
Full clinical information including age and gender, smoking history, comorbidities, endoscopic examination results, follow-up appointments, and computed tomography (CT) or magnetic resonance imaging (MRI) evidence were available for all patients. Preoperative CT scans and MRI were evaluated to identify the localization of the lesion and the involved sinuses and to differentiate between sinus involvement by tumor or by secretion in extensive disease. Using this modality, all patients were classified according to Krouse 6 and Dragonetti-Minni 20 staging (Table 1).
Krouse (2000) and Dragonetti-Minni (2008) Staging Systems for Inverted Papilloma.
All patients were treated with endoscopic approach or combined endoscopic/open approach (midfacial degloving approach, frontal osteoplastic or lateral rhinotomy approach). After debulking of the lesion, the attachment sites of the tumor were identified, removing only the disease mucosae and preserving healthy tissues. Intraoperative biopsy was used to identify resection margins. The surgical approach was tailored to preoperative imaging findings and modified according to intraoperative findings. The goal of surgical resection was tumor debulking followed by complete tumor removal. 3,11
The primary outcome measure was the incidence of persistence or recurrence of IP in our sample; persistence was defined as the presence of disease <6 months from surgery, persistence was defined as the presence of disease >6 months from surgery. Secondary outcome measures were the frequency of negative events, such as surgical complications and death. Recurrence rates and intervals between surgical treatment and first recurrence, according to surgical methods and risk factors, were analyzed. Averaging ± standard deviation, χ2 test, Student t test, Kaplan-Meier estimator, and Cox proportional hazards model to estimate the survival function were used for statistical analysis.
Results
General Findings
One-hundred thirty patients were diagnosed with sinonasal IP; all patients were of Caucasian race. The group was composed of 89 (66.9%) males and 41 (30.8%) females (ratio: 2.17:1); age ranged from 21 to 89 years (average: 60.7 years, standard deviation [SD] = 17.28). The average duration of follow-up was 60 months (36-104 months, SD = 19.28).
Recurrence of the disease was found in 12 (9.2%) patients (7 males and 5 females, average age 58.3 years, range 21-79 years, SD = 15.67); recurrence was found in 6 (4.6%) cases (4 males and 2 females, average age 56.9 years, range 28-75 years, SD = 16.70). No statistically significant effect on recurrence or persistence rates was found for sex (P = .460 and P = .872, respectively) and age (P = .634 and P = .542, respectively).
Fourteen (10.8%) patients died during follow-up; 4 (3.1%) died for IP sequelae and 10 (7.7%) for other causes not related to the sinonasal disease. Patients who died for the sinonasal disease were significantly younger than those who died for other causes (Mann-Whitney test, P = .001).
Risk Factors
Figure 1 shows the prevalence of known risk factors in the study sample. Almost half (46.2%) of the enrolled patients had a history of cigarette smoking. Between the 12 cases with recurrence of disease, 8 (66.7%) were smokers (P = .038, Cox model). Contrarily, no statistically significant differences were found between smokers and nonsmokers who had a persistence of the disease (P = .541, Cox model). Smoking influenced overall survival over time (P = .019, t test); among the patients who died during follow-up, 80% were smokers (P = .015).
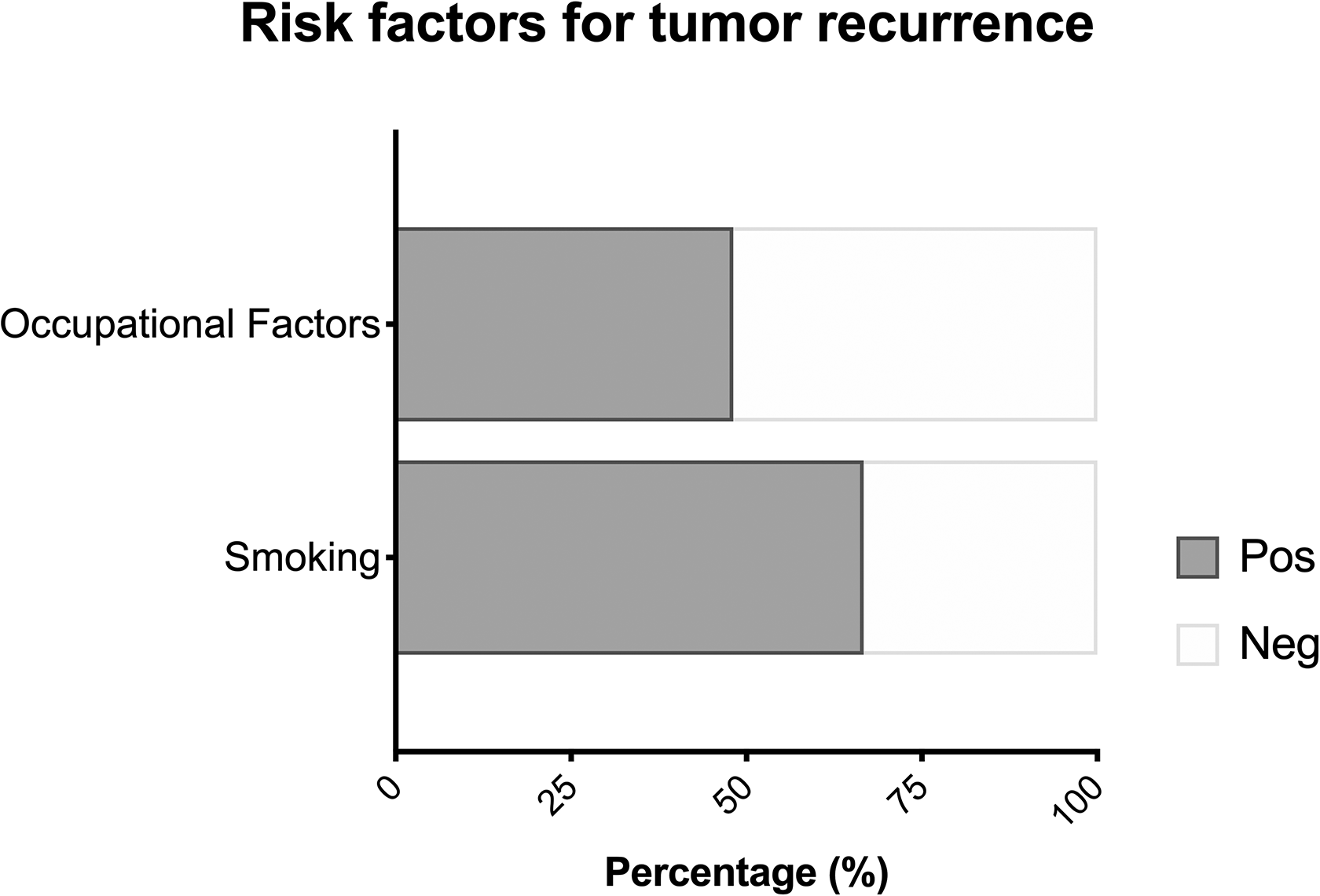
Prevalence of smoking and occupational factors for sinonasal cancer such as wood- and leather-related occupations, textile industry, and metalworking in the study sample.
Twenty-six (20%) patients had a history of exposure to known or suspected occupational factors for sinonasal cancer (wood and leather industry, textile industry, and metalworking). No significant differences were found regarding the frequency of recurrence and persistence among patients with and without exposure to occupational risk factors (P = .632 and P = .119, respectively). Mortality was higher in patients with history of exposure to occupational risk factors (P = .011).
Histology
In the present study, 115 (88.5%) patients had a definitive pathological diagnosis of IP, 4 (3.1%) had a diagnosis of IP associated with severe cellular dysplasia, 7 (5.4%) had a diagnosis of IP associated with moderate dysplasia, while 4 (3.1%) had a diagnosis of squamous cell carcinoma (SCC) in IP (Figure 2). In the latter cases, SCC was already present with the IP (synchronous tumors). During the follow-up, none of the remaining 126 patients developed a malignant tumor (metachronous tumor).
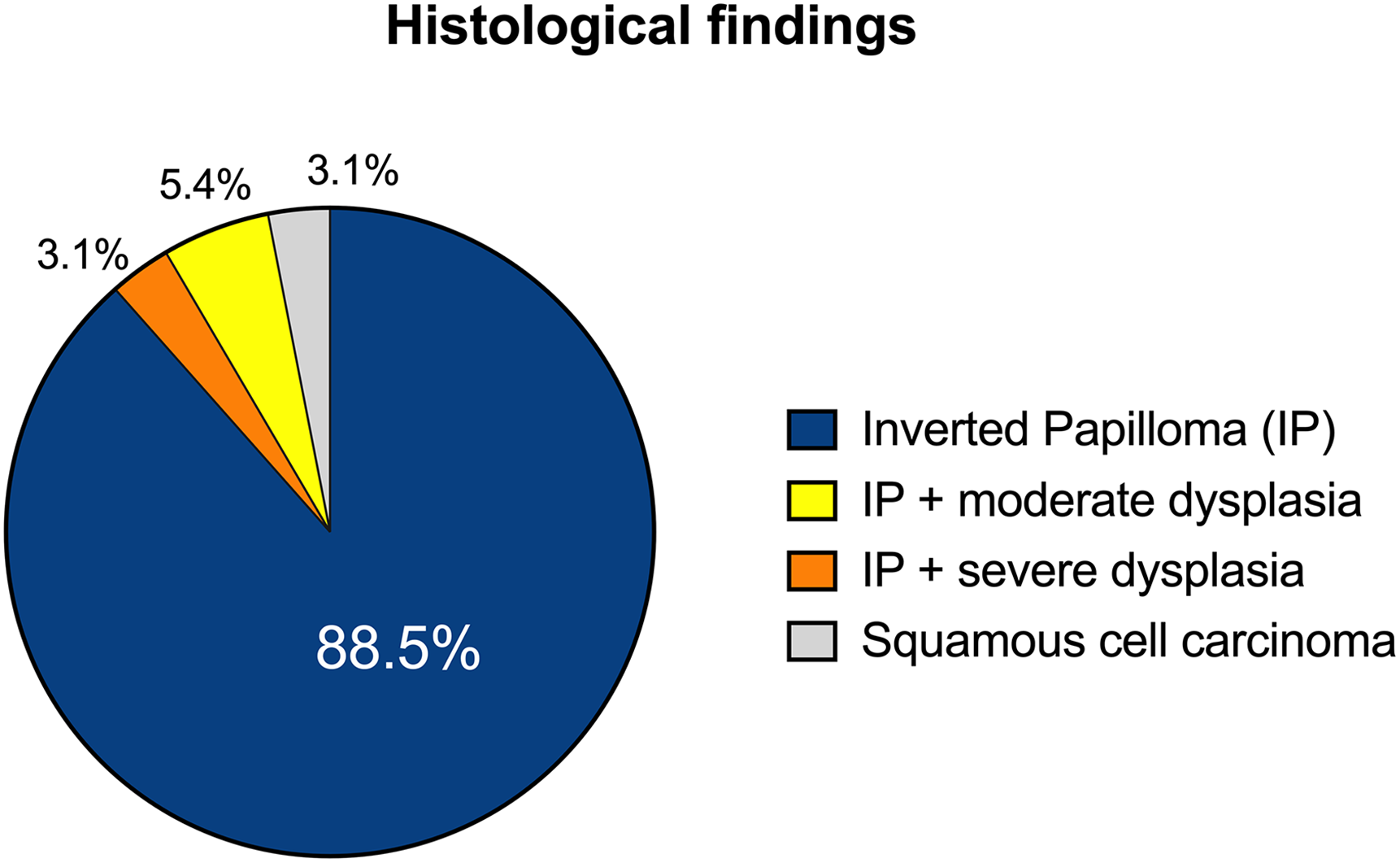
Definitive pathological findings in the patients included in the study.
Cox regression analysis showed a significant correlation between recurrence rate and histology. Patients with IP and dysplasia had a higher recurrence rate compared to those with IP alone (P = .038; hazard ratio = 2.405); no correlation was found between histology (dysplasia) and persistence of disease (P = >.05).
Patients diagnosed with SCC had a lower survival rate (P < .001). The disease-specific survival for IP alone, dysplasia-associated IP, and IP associated with carcinoma was 100%, 100%, and 50%, respectively.
Lesion Side
Sixty-three (48.5%) patients developed sinonasal IP in the right side, 67 (51.5%) in the left side. The lesion site did not show a significant correlation to recurrence (P = .918) nor to persistence (P = .957; Figure 3).
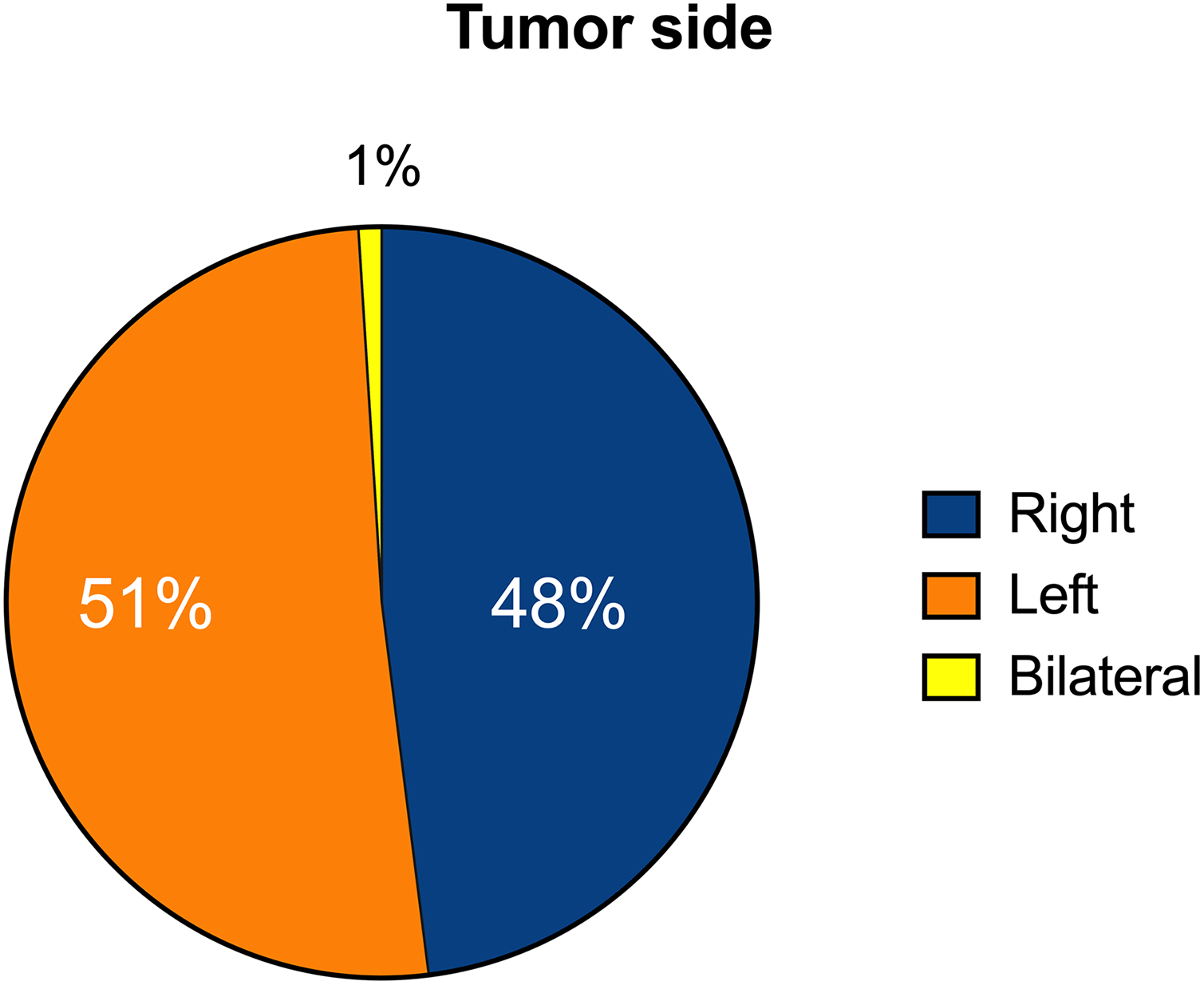
Tumor side in the study sample.
Figure 4 details the tumor location in our sample. The maxillary sinus was involved in 54 (41.5%) cases, the anterior ethmoid sinus in 44 (33.8%) cases, the frontal sinus was involved in 21 (16.2%) cases, and the sphenoid sinus in 11 (8.4%) cases. The origin of IP significantly influenced the frequency of persistence and recurrence of the disease: 7 (58.3%) of the 12 recurrences developed in patients with sinonasal IP located in the anterior wall of the maxillary sinus; 3 (25%) occurred in patients with tumor located in the frontal sinus; 1 (8.3%) in the anterior ethmoid sinus and 1 (8.3%) in the lateral wall of the maxillary sinus. These differences were significant (Cox regression, P = .045). The persistence of the tumor was also related to its origin (P = .009); in 2 (33.3%) of the 6 patients who had disease persistence, the site of origin of the tumor was located at the level of the upper wall of the maxillary sinus. Contrarily, the tumor origin did not influence survival (P = .638 for death in general, P = .554 for death from other causes, P = .461 for death due to the sinonasal condition).
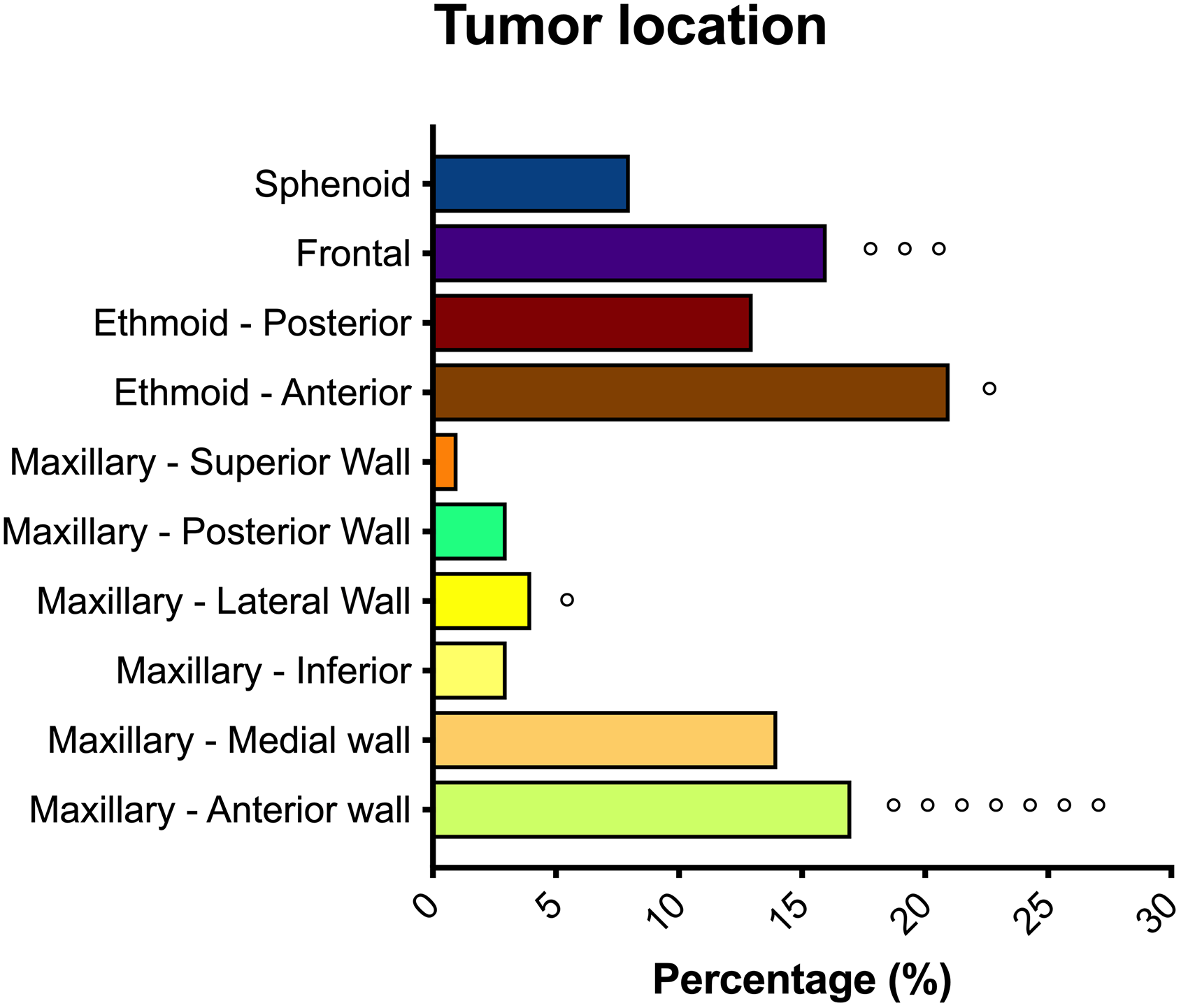
Tumor location in our sample. The maxillary sinus was the most involved, followed by the ethmoid sinus, the frontal sinus, and the sphenoid sinus. Circles (°) indicate the number of recurrences that developed in our sample, sorted by location.
Stage
Patients were classified according to the Krouse and Dragonetti-Minni classifications. Tumor staging according to the Krouse classification was not statistically significant for primary outcome (P = .431 for recurrence, P = .343 for persistence), while staging according to the Dragonetti-Minni classification was significant for the development of recurrence (P = .045), but not for the other outcomes.
Surgical Approach
All patients included in the study were treated with endoscopic approach based on ethmoidal subperiosteal resection (ESR) associated with sphenoidotomy, maxillary antrostomy, and frontal sinus recess opening, with possible dissection of other sinuses according to the extension and the origin of the tumor. Twenty-five (19.2%) cases were treated with ESR; 11 (8.5%) cases with ESR associated with sphenoidectomy with drilling of the anterior and inferior wall of the sphenoid; in 15 (11.5%) patients, an ESR associated with extended medial antrostomy was performed; 11 (8.5%) cases were treated with ESR and endoscopic maxillectomy; 45 (34.6%) cases with ESR associated with anterior maxillectomy with (18.6%) or without (16%) nasolacrimal duct resection; finally, 23 (17.7%) patients were treated with ESR associated with frontal sinusotomy according to Draf type II (9.8%) or Draf type III (7.9%; Figure 5).
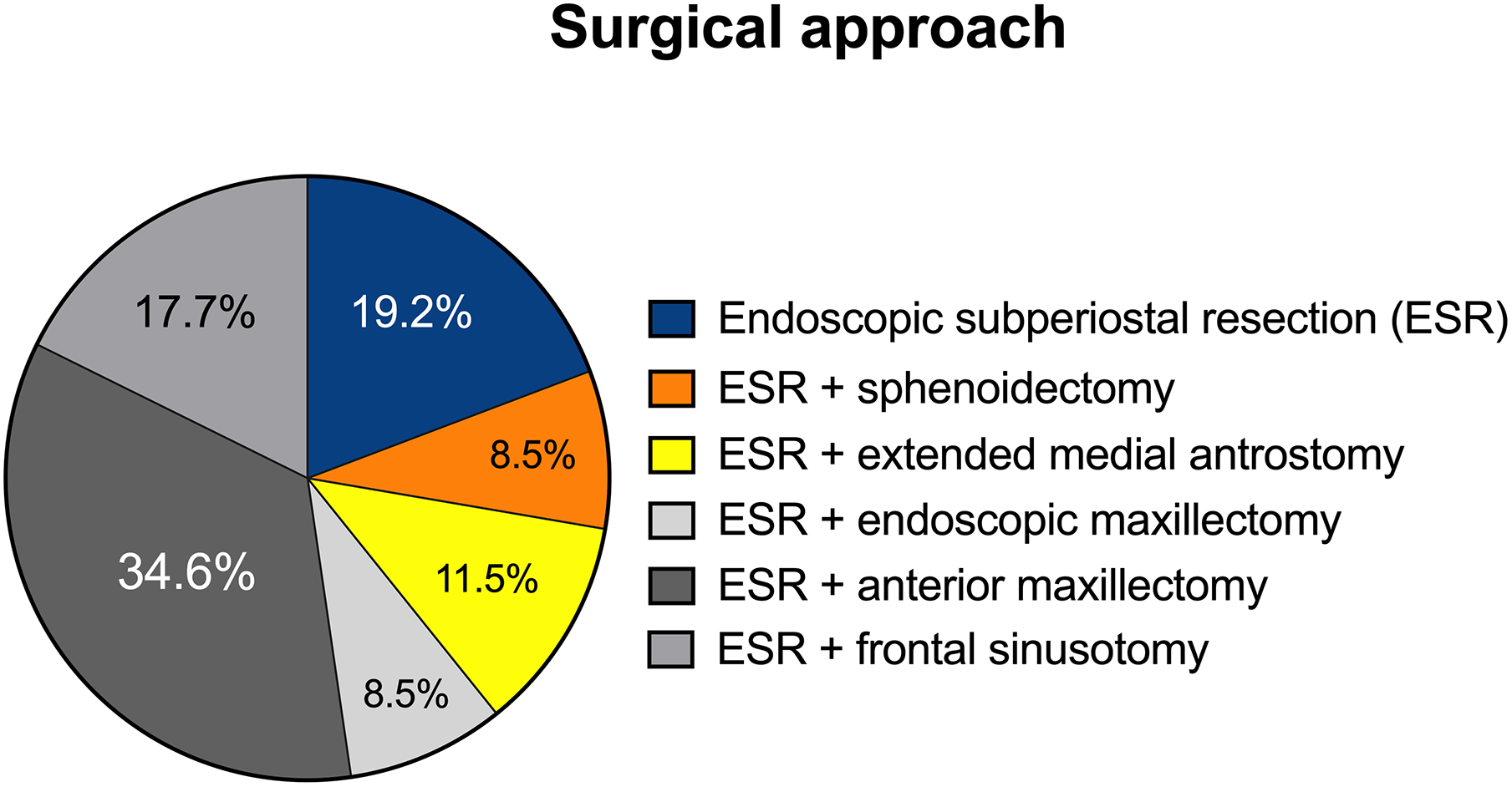
Surgical approach performed in the patients included in the study. All patients were treated with endoscopic approach based on ethmoidal subperiostal resection (ESR) associated with sphenoidotomy, maxillary antrostomy, and frontal sinus recess opening, with possible dissection of other sinuses according to the extension and the origin of the tumor.
A statistically significant difference between recurrence and persistence rates was found for each approach (P = .048 and P = .045). In particular, patients who underwent ESR alone had a higher risk of tumor persistence, while the patients treated with ESR combined with anterior maxillectomy had a higher risk to develop a recurrence. The nasolacrimal duct resection had a significant effect on recurrence rates: Only 1 patient who underwent nasolacrimal duct resection developed a recurrence, while 5 patients with no nasolacrimal duct resection developed a recurrence.
The surgical approach did not influence the survival rate in our sample; Cox regression analysis showed a P value of .834, .542, and .231, respectively, for death, death due to other causes, and death due to the sinonasal condition.
Complications occurred in 24 (18.5%) patients. Minor complications occurred in 12 (9.2%) patients: epiphora in 7 (58.3%) patients, epistaxis in 3 (25%) cases, and periorbital edema in 2 (16.7%) cases. Major complications occurred in 10 (7.7%) patients; 3 (30%) had a rhino-liquoral fistula, 4 (40%) cases a frontal mucocele, and 3 (30%) cases a lacrimal duct stenosis. The development of complications had no effect on primary outcomes (P = .341 for persistence and P = .341 for recurrence; Figure 6).
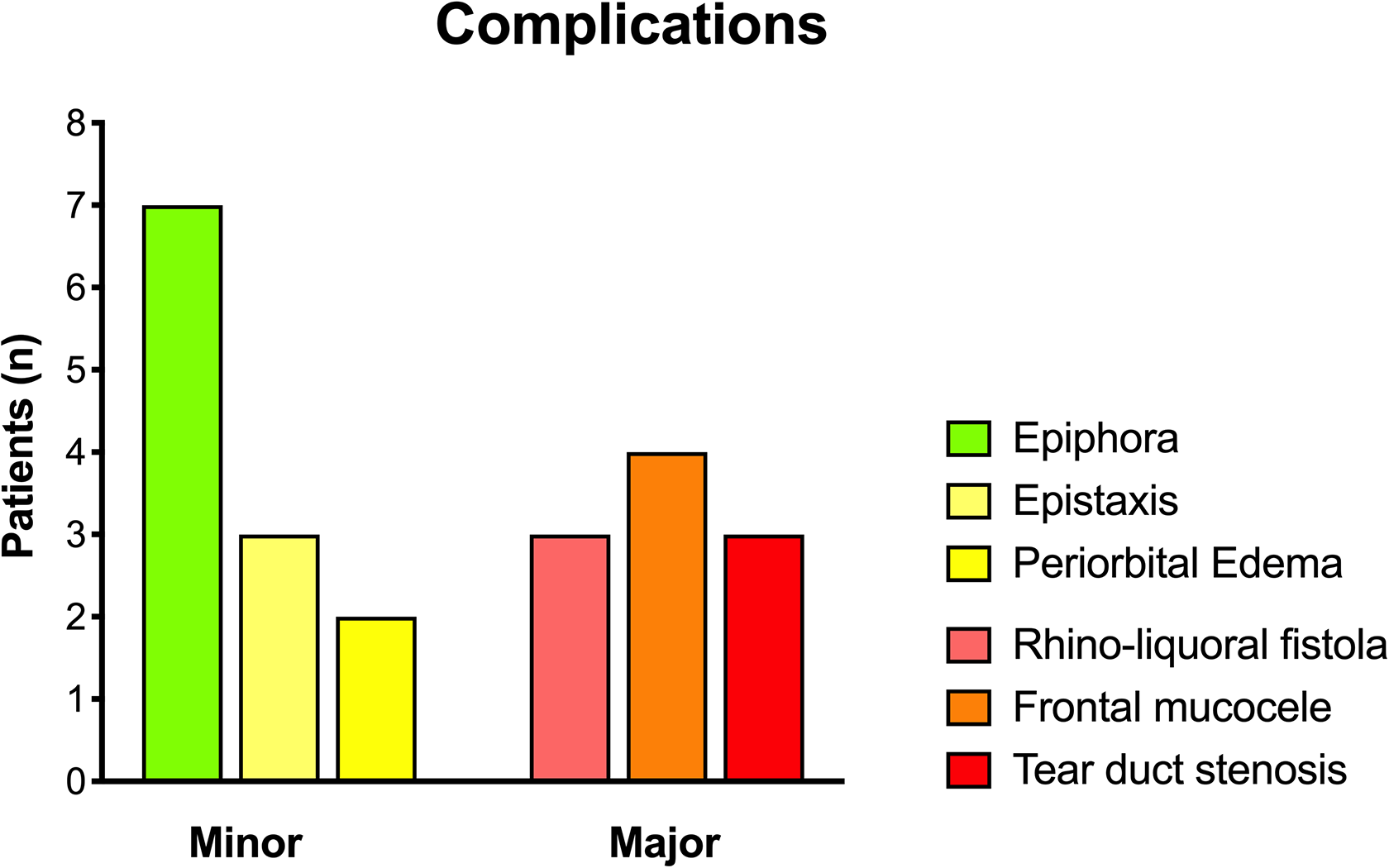
Minor and major complications occurred in our sample.
Intraoperative positive margins were found in 34 (26.1%) cases; this required an immediate enlargement of the surgical exeresis within the same surgical procedure. The risk of recurrence and persistence of IP in our sample was not influenced by the presence of intraoperative positive margins.
Discussion
Recent meta-analyses have shown a recurrence rate of sinonasal IP between 15% and 20% 21,22 ; however, there is still much controversy on the entity and role of the factors involved in IP recurrence. The aim of this multicenter retrospective study was to analyze the factors affecting the recurrence and persistence of sinonasal IP.
It is well known that IP develops more frequently in men than in women 23 ; in our sample, gender did not seem to be related to the recurrence rate, as well as age.
Among the 130 patients included in the study, almost half of them had a history of smoking; we found that smoking was significantly associated with recurrence. These data are consistent with what reported by Diaz Molina et al on a review of 61 patients with IP. 24 The present study also revealed a significant association between occupational exposure to risk factors, especially wood- and leather-related industries, textile industry, and metalworking, and IP; this is consistent with the findings reported by D’Errico et al. 25 In contrast, exposure to risk factors did not appear to play a role in therapeutic failure in our patients. This may depend on the characteristics of the sample; in fact, more than half of the patients with a history of occupational exposure were no longer actively employed at the time of the first diagnosis. Therefore, it is possible that the pathogenic role of these factors decreases upon termination of exposure.
Several studies tried to define histological parameters that could help predicting multiple recurrence such as malignant transformation. 7 According to the European Position Paper of endoscopic management of IP, the incidence of dysplasia based on current literature is 1.9% 26 ; this is significantly lower than our findings (9%). In our sample, patients with IP associated with moderate or severe dysplasia had a higher rate of recurrence compared to those with no dysplasia.
We found no statistically significant difference in recurrence rates according to Krouse stage, while we found a predictive role using the Dragonetti-Minni classification. The former only considers the origin of the tumor, not its extension; this may explain the low predictive value. Instead, the classification proposed by Dragonetti-Minni 20 appears more complete and exhaustive; moreover, it seems to have a better prognostic value on the risk of recurrence.
The side was not significantly related to a higher rate of recurrence or persistence in our sample, while lesion localization was significantly correlated with recurrence and persistence. Indeed, 7 (58.3%) cases of recurrence developed in patients with IP in the anterior maxillary sinus wall; in 3 (25%) cases, IP was in the frontal sinus. This finding may be explained by the surgical difficulty to completely remove the lesion in these anatomical sites. 14,27 -30 The elevate frequency of recurrence and persistence of disease in patients with an IP in the anterior wall of the maxillary sinus or in the frontal recess may depend on the difficulty of endoscopically approach these areas. Finally, history of previous sinonasal surgery represented an important risk factor for IP recurrence.
Based on our data, the site of origin, extension, presence of dysplasia, and previous endoscopic-only surgery can lead to an increased risk of recurrence, estimated at around 6 times greater than for patients without these characteristics. These results support the theory that an incomplete initial resection may lead to an increased likelihood for recurrence after a second resection, emphasizing the importance of a complete radical resection of IP during the first surgery. 8,31
This study has some limitations. Being a multicenter study, surgery was performed by different surgeons. Although the surgeons involved in the study had a comparable level of experience (more than 20 years of experience), some surgical differences may be present in our sample. The study showed a significant association between occupational exposure to risk factors and IP; however, exposure to risk factors did not appear to play a role in therapeutic failure in our patients. This may depend on the fact that more than half of the patients with a history of occupational exposure were no longer actively employed at the time of the first diagnosis.
In conclusion, our analysis of the cumulative risk of recurrence and persistence of IP has shown that 3 of the 4 risk factors of recurrence mainly depend on the localization of the tumor and on the surgical approach; contrarily, some factors did not seem to be related to the surgeon’s ability, such as the presence of cell dysplasia. These elements must be carefully considered during clinical evaluation and especially during the follow-up visits of patients with a diagnosis of IP.
Footnotes
Authors’ Note
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.