
Abstract

A 23-month-old female presented to clinic with increased work of breathing, wheezing, and inspiratory stridor that had gradually worsened over the past 6 months. She had a history of biliary atresia that was corrected with a liver transplant at 10 months. Following her transplant, her immunosuppressive regimen consisted of daily tacrolimus. Direct laryngoscopy revealed diffuse submucosal lymphoid-appearing hyperplasia of multiple sites in the nasopharynx, oropharynx, and supraglottis (Figures 1 –4). The epiglottis was significantly hyperplastic and redundant, causing significant upper airway obstruction (Figures 1 and 3). Multiple biopsies were taken of the redundant mucosa of the epiglottis and the right anterior tonsillar pillar to improve airway patency. Nasopharynx evaluation revealed significant hyperplasia of the tubal tonsils circumferentially around the eustachian tube orifice.
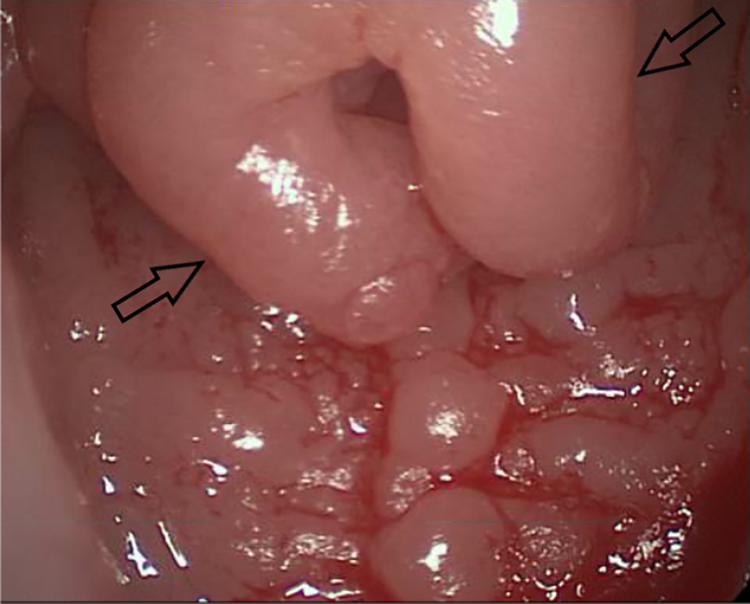
Diffuse lymphoid hyperplasia of the epiglottis (arrows).
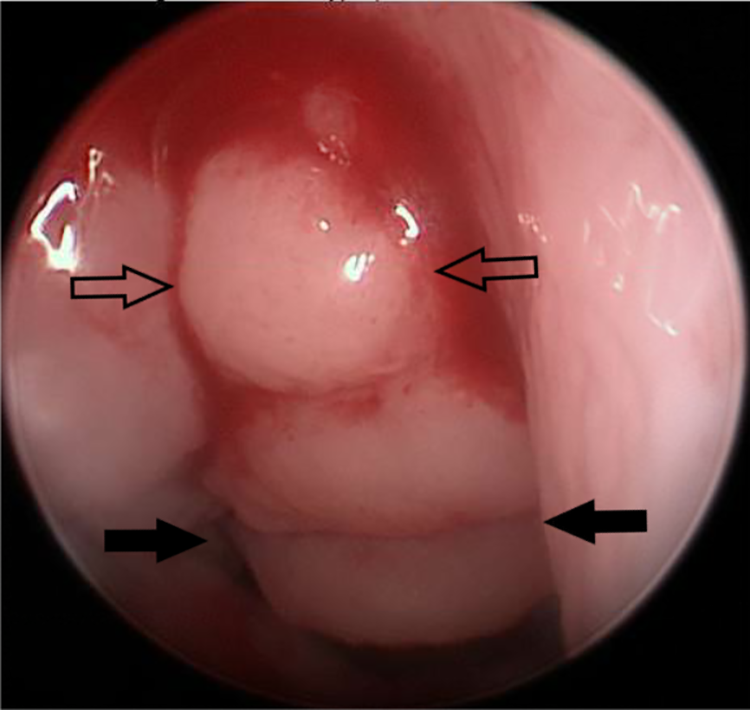
Adenoid hyperplasia (arrows) and right tubal tonsil hyperplasia (filled arrows).

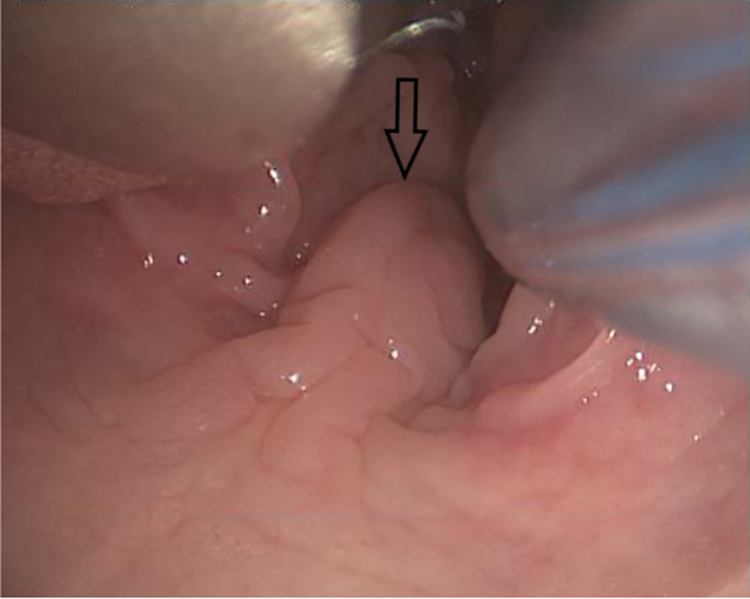
Redundant epiglottic mucosa (arrows).
Lymphoid hyperplasia involving soft palate and uvula (arrow).
The tacrolimus was discontinued following a preliminary diagnosis of post-transplant lymphoproliferative disorder (PTLD). Her pathology results were consistent with early PTLD and she was started on ganciclovir and intravenous immunoglobulin (IVIG). Follow-up direct laryngoscopy one month later revealed improving lymphoid hyperplasia of the epiglottis and a pedunculated mucosal lesion emanating from the left piriform sinus. Both of these areas were biopsied and revealed residual PTLD. She underwent an additional IVIG infusion, and follow-up direct laryngoscopy two months later revealed stable hyperplasia.
Post-transplant lymphoproliferative disorder is a heterogenous condition caused by B-cell proliferation in the setting of immunosuppressant medications. 1,2 Involvement of the airway, particularly in children, is a rare occurrence. 3 A comprehensive literature review revealed 22 cases of pediatric PTLD presenting with manifestations in the airway. 2 -17 Patients most commonly presented with stridor, respiratory distress, cough, and tonsillar enlargement. The most common anatomic locations were the tonsils and epiglottis. Most cases were treated with a reduction of immunosuppression and surgical debulking, with some utilizing antiviral agents, IVIG, chemotherapy, and steroids.
In a stridulous pediatric patient who is status post solid organ transplantation, PTLD should be on the otolaryngologist’s differential diagnosis. Early recognition and treatment of this condition can prevent potentially serious outcomes.
Footnotes
Authors' Notes
Presented as a poster at the Virginia Society for Otolaryngology Annual Meeting, April 12th, 2019, in Alexandria, VA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.