
Abstract

There has been a recent reemergence in the development of oral syphilis, a sexually transmitted infection caused by the Treponema pallidum subspecies pallidum spirochaeta bacterium, with oral manifestations dependent on stage at presentation (early: primary, secondary, early latent; late: late latent, tertiary). Oral sex has contributed to the overall increase in disease spread, with the highest incidence in 25- to 29-year-old males (88% of oral cases documented in males, especially in males who have sex with males). Concurrent infections with HIV or other sexually transmitted infections are common. The lips, tongue, and palate are most commonly infected, while tonsils and gingiva may also be affected. Early primary presentation is of a painless, usually solitary ulcer (chancre) which forms about 3 weeks after inoculation (Figure 1). Early secondary presentation is about 3 to 12 weeks after chancre resolution and is the stage most oral syphilis is diagnosed. There are mucous white patches, sometimes multifocal. Condyloma lata is a papillary lesion. Latent syphilis is considered inactive disease, with serologic proof of infection, but without disease symptoms, usually >1 year after secondary syphilis. Tertiary syphilis may develop anywhere up to 15 years after initial infection, showing gumma (granulomatous inflammation) of the palate and/or tongue with atrophic luetic glossitis. Congenital manifestations are rare (screwdriver-shaped incisors and mulberry molars). Treatment involves intramuscular penicillin injections with appropriate counseling and screening for other sexually transmitted diseases.

Palate ulceration without a significant reaction in this case of oral syphilis (courtesy Dr B. L. Nelson, DDS).
The histologic features are quite nonspecific and mimic other disorders. As such, a high degree of suspicion and a low threshold for testing must be considered in all cases that show an intense chronic inflammatory infiltrate, predominately of lymphocytes and plasma cells (Figure 2). Epithelial hyperplasia, with or without ulceration, shows spongiosis with an associated inflammatory cell exocytosis (Figure 2). Vasculitis is not usually seen. A Warthin-Starry stain is difficult to interpret, as spirochetes are part of the normal oral flora. Thus, a T. pallidum immunohistochemistry study is highly specific, showing the corkscrew-shaped spirochetes (Figure 3). Serologic confirmation is recommended by either nontreponemal tests or treponemal tests. Since the histologic features are so nonspecific, aphthous ulcer, traumatic ulcer, plasma cell gingivitis, fungal infection, pseudoepitheliomatous hyperplasia, lichenoid mucositis/lichen planus, immune-mediated vesiculobullous disorders, and even dysplasia must all be considered in the differential diagnosis.
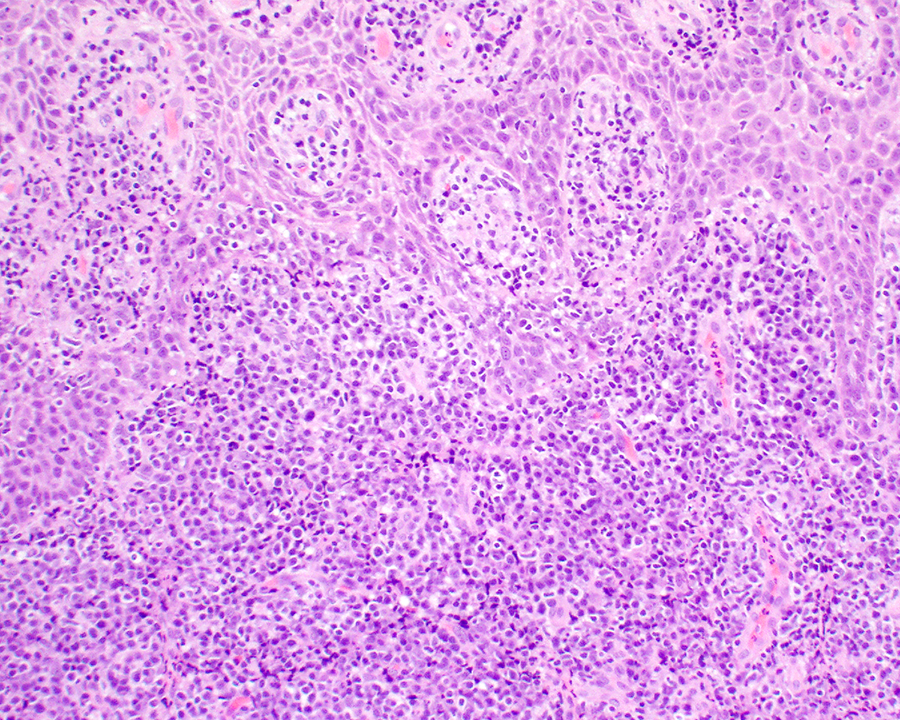
The hyperplastic surface epithelium shows lymphoid exocytosis, with a marked lymphoplasmacytic stromal infiltrate.
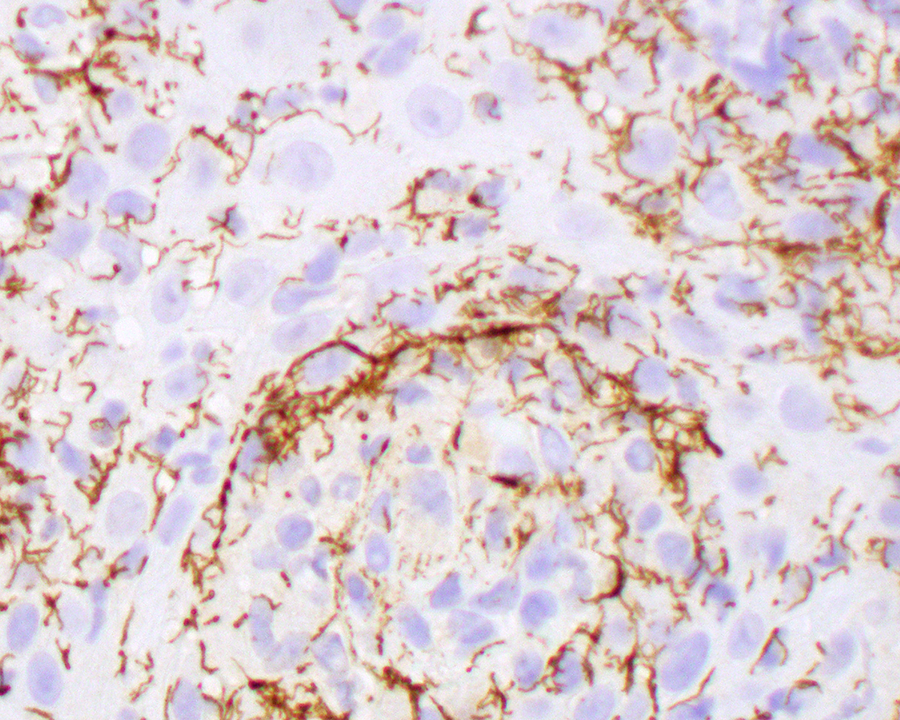
The corkscrew-shaped organisms are highlighted by this Treponema pallidum immunohistochemistry study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.