
Abstract
Background and Purpose:
Mandibulectomy remains the treatment of choice for oral cavity squamous cell carcinoma with infiltration of bone and for benign tumors with full mandibular thickness involvement. Although bone resection margins are critical for patient outcomes, intraoperative immediate bone margins assessment is inadequate, and few alternative options have been described. The purpose of this study was to describe the use of an existing intraoperative radiographic system for objective determination of bone resection margins during mandibulectomy.
Methods:
We conducted a retrospective case series of all patients at the Greater Baltimore Medical Center who underwent mandibulectomy and received intraoperative Faxitron radiography from January 1, 2016, to March 1, 2019. Patient characteristics including age, sex, diagnosis, tumor location, clinical and pathologic stage, procedure performed, and bone resection margins were reviewed.
Results:
A total of 10 patients underwent mandibulectomy with intraoperative radiography. Nine (90%) received surgery for squamous cell carcinoma, with 1 (10%) for ameloblastoma. Out of those with squamous cell carcinoma, tumor location varied, and all were clinically stage T4. Final pathologic margins were negative in all cases (10/10), though in 2 cases, close margins were assessed intraoperatively, leading to further resection or change in operative plan.
Conclusion:
Intraoperative radiographic assessment of bone resection margins is a promising technique, though further validation is required.
Introduction
Oral squamous cell carcinoma (OSCC) represents a substantial burden on health in the United States and worldwide, representing 2% to 4% of all diagnosed malignancies in the United States, resulting in over 8000 deaths annually, with this incidence projected to increase over time. 1 The diagnosis of OSCC carries a significant risk of morbidity and mortality, despite substantial advances in the fields of surgery and oncology. Rates of mortality have remained relatively constant over decades, highlighting the desperate need for further developments in diagnosis and management.
Surgery is the treatment of choice for OSCC and may be followed by chemoradiotherapy for advanced tumors. 2 Mandibulectomy is indicated when there is bone invasion, 3,4 with a goal of obtaining negative margins while reducing functional and aesthetic defects. Segmental mandibulectomy is a treatment of choice if there is full-thickness mandibular involvement.
Bone resection margins after mandibulectomy have been shown to have a significant effect on patient survival. In the study by Smits et al, patients with positive resection margins had a 5-year survival rate of 23%, compared to 35.3% in those with negative margins. 3 Rates of bone margin positivity vary significantly in the literature, ranging from as low as 2% to as high as 21%. 3,5 Unlike soft tissue, bone resection margins are not obtainable through frozen sections, due to high mineral content. 6 Therefore, histopathological confirmation of the presence of tumor cells is only available days after surgery. 5,6
Despite the importance of margins, and the long latency of traditional histopathological methods, there remain few alternatives for intraoperative assessment of resection margins during mandibulectomy other than conventional visual inspection and palpation, which may be inadequate in many cases. Intraoperative cytological assessment has been described as a promising technique, though may be limited by specimen desiccation or insufficient material. 6 In 2018, Raman spectroscopy was proposed as another method to distinguish tumor from healthy tissue, through the determination of differences in water concentrations. 5
Preoperative radiographic assessment, via computed tomography (CT), is commonly performed before mandibulectomy, though its efficacy has been debated. The CT assessment of mandibular tumor involvement has been shown to have reasonable sensitivity and specificity, though this is diminished in tumors at the retromolar trigone 7 and in patients with irregular dental sockets. 8 Clinical assessment has been shown to be a crucial component of preoperative evaluation, with higher accuracy and sensitivity than radiographic evaluations. 8 In addition to the limitations of CT, preoperative assessment cannot fully predict the extent of bone involvement due to the delay between imaging and surgery and thus is inadequate for real time and intraoperative accurate determination of tumor involvement.
The Faxitron microradiography workstation (Figure 1) was developed as a portable, simple system for intraoperative assessment of specimens during breast surgery. 9 It is a mobile station, powered by a standard AC outlet, and can be placed in the operating room for fast imaging of specimens, which can be viewed immediately through a digital image system. The Faxitron workstation is widely adopted for use during breast surgery and has been shown to decrease rates of margin positivity. 10 In this case series, we describe the use of Faxitron microradiography for the intraoperative assessment of specimen margins immediately after mandibulectomy.

Faxitron BioVision device.
Patients and Methods
We conducted a retrospective case series of all patients who underwent mandibulectomy and received intraoperative radiography at the Greater Baltimore Medical Center from January 1, 2016, to March 1, 2019. Institutional review board approval was obtained. Patient characteristics, including age, sex, diagnosis, tumor location, clinical and pathologic AJCC 8th edition stage or restage, the procedure performed, and bone resection margins were reviewed. Radiographic images of specimens were collected and compared with final pathologic margins.
Surgical Procedure
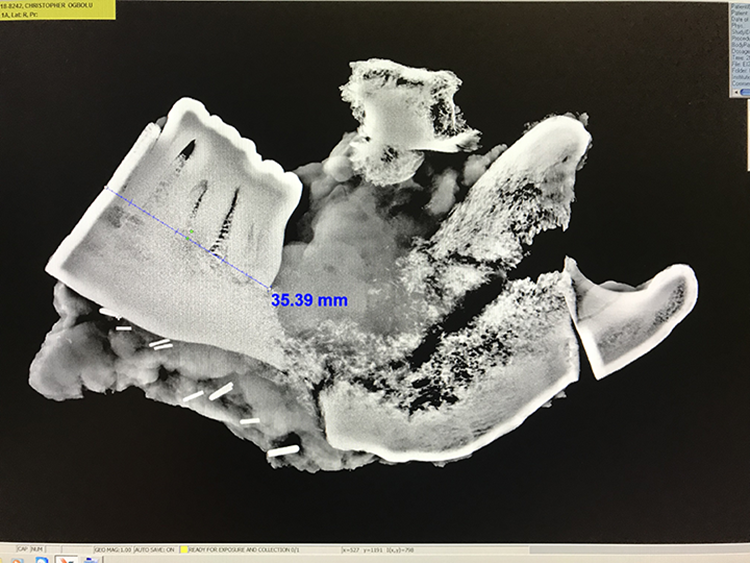
All cases were presented to the multidisciplinary tumor board, and imaging was reviewed preoperatively to determine the lines of resection in the bone margins. Only the cases with clinical and radiologic T4 or bony invasion and full-thickness benign tumor of the mandible were included in the Faxitron imaging study. Informed consent was taken. A 1.5-cm mucosal margins were measured using an intraoperative ruler for mucosal lines of resection. The mandibular specimen was immediately imaged using the Faxitron imaging apparatus in the operating room upon completion of the segmental mandibulectomy. Intramedullary bone invasion of the tumor was reviewed. The distance of the proximal and distal lines of resection to the intramedullary bone invasion or benign mandibular tumors was digitally measured in Faxitron imaging unit. A 1-cm margin was considered as adequate margin on imaging (Figure 2).

Measurements from intramedullary bony squamous cell cancer invasion to the line of resection.
Intraoperative Specimen Radiography
During the operation, the mandibular resected specimen was placed inside the Faxitron X-ray cabinet, with care to avoid oblique orientation. The cabinet door was then closed, and imaging was initiated, with automatic calibration. After the acquisition, the images were viewed by the surgeon, and measurements of margin distance were created. The line of resection was considered inadequate if the bone margins were determined to be close or less than 1 cm, after which additional bone margins were resected, added to the specimen and reimaged. The lines of resections were again remeasured and determined if greater or 1-cm margin was achieved (Figure 3).

Close bone margin requiring additional bone resection to have a 1-cm margin.
Results
A total of 10 patients underwent mandibulectomy with intraoperative specimen radiography during the reviewed period. Patient characteristics are listed in Table 1. Age ranged from 23 to 76 years, and 50% were female. Except for one benign tumor, all were squamous cell carcinomas, and location varied from the gingiva, tongue, retromolar, and mandible. Final pathologic bone resection margins were negative in all cases (10/10), though 2 cases had close margins noted during intraoperative specimen imaging, which resulted to additional bone resection in one case (Figure 3) and a change of operative plan in another case (Figure 4). For patient 6, preoperative planning was to do a segmental mandibulectomy with preservation of the mandibular condyle. However, intraoperative imaging showed a close margin, which requiring a change of operative plans to a hemi-mandibulectomy. Patient 7 on intraoperative Faxitron imaging showed close margin and requiring additional bone resection to have a 1-cm margin. Both cases have a final pathologic negative bone margin.
Surgical plan was to preserve the mandibular condyle, but lines of resection were close requiring a hemi-mandibulectomy.
Patient Characteristics.
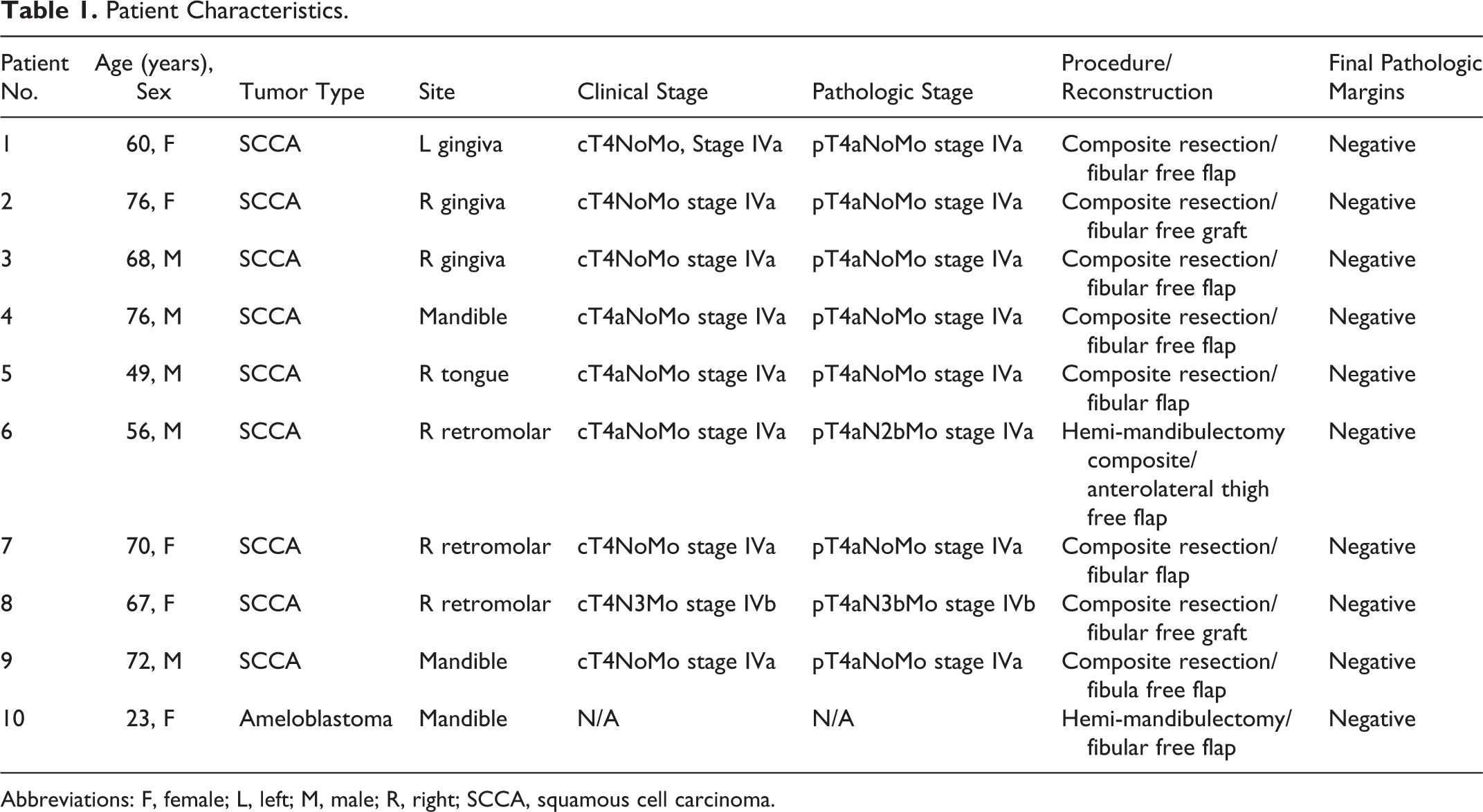
Abbreviations: F, female; L, left; M, male; R, right; SCCA, squamous cell carcinoma.
Discussion
In this case series, we describe the use of Faxitron microradiography as a viable method for intraoperative assessment of bone resection margins during mandibulectomy. The Faxitron workstation is commonly available due to its wide use during breast surgery and offers a feasible method of digitally measuring mandibular margins within the operating room. In the cases described, these radiographic results influenced clinical decision-making in 2 cases, providing evidence for the need of additional resection and possibly preventing positive margins and future reoperation. In the rest of the cases, intraoperative imaging ensured adequacy of the bone margin of resection to the operating and reconstructive team.
Our study adds to the current base of literature on intraoperative bone margin assessment. In 2014, Nieberler et al described a method for cytological assessment, in which specimen margins were scraped, placed onto slides, stained, and assessed by cytopathologists. 6 Through this method, they obtained a sensitivity of 94.4% and sensitivity of 97.5% through a reasonably short specimen preparation and assessment process. This was the first approach for assessing cortical bone specimens, though described limitations included specimen desiccation, insufficient material, and low quality cytologic preparations due to the presence of blood cells. Another limitation was the presence of false-negative results, likely due to nonrepresentative sampling, and false positives due to specimen contamination. While these results are very promising, this method currently has not been widely used.
Barroso et al investigated the use of Raman spectroscopy for the detection of tumor cells in resection surfaces in 2018. 5 Raman mapping relies on the scattering of light, emitted from a laser, from a material. This scattering is picked up, and molecular mapping can be determined. This was performed using a confocal Raman microscope; specimens were rinsed, placed in a cartridge, and mapped, with tumor cells detected through an algorithm based on water concentration. These methods provided a sensitivity of 95% and a specificity of 87%. This method is also promising, but limitations included the need to cut flat contours on the resection surface for optimal quality mapping, and Raman spectroscopy and related equipment are still not widely used or available in the clinical setting.
Our study describes a feasible and widely available system for intraoperative assessment through radiography. This has already been validated and utilized for breast surgery and can easily be adapted for use in mandibulectomy at medical centers in the United States and around the world, providing an easy, rapid method for specimen analysis. This method does not require assessment by a trained cytopathologist, although concurrent reading by a radiologist may provide additional benefit. Other advantages include the ability to image the entire specimen intraoperatively, imaging and assessment within the operating room versus waiting for final pathology, and doing reoperation if the bone margins are positive.
The major limitation of our study is the case series design; with small sample size, we cannot sufficiently validate the use of this system for bone and determine accuracy. Further analysis must be performed for validation of this method once more cases have been performed. However, the impact on operative decision-making speaks to the potential benefit for reducing reoperation and possibly improving patient outcomes, including survival.
In conclusion, the Faxitron microradiographic workstation is an existing imaging system which can quickly be adapted for quick intraoperative assessment of bone resection margins during mandibulectomy. This method allows for digital measurement of margin distance. Although the sample size was small, determination of margin negativity and the need for possible additional resection are important intraoperative tools for both the oncologic surgeon and the reconstructive plastic team. Although this method remains to be validated for use with intraoperative bone specimens imaging, it is a promising tool for addressing the critical need for better objective assessment of margins during mandibular resection.
Footnotes
Acknowledgments
David Chen, MD, Melanie Benton, MS, PA (ASCP), Mary Kay Pogar, MS, PA (ASCP), Kelly Bair, MS, PA (ASCP), Robert Palermo, MD, Chairman Department of Pathology and Laboratory.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.